Explain the MRCP MRI
Reading File
Finding Sources
Finding Sources
Searching the Web
MRCP MRI magnetic resonance cholangiopancreatography technique indications interpretation
Reading File
Reading File
Reading File
Loading Image
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative textbooks and images. Let me compile the full answer.
MRCP - Magnetic Resonance Cholangiopancreatography
What Is MRCP?
MRCP is a non-invasive MRI-based technique that selectively images fluid within the biliary tree and pancreatic ductal system. It is a technical refinement of standard MRI, not a separate scanner - it uses the same MRI machine but with a specialized pulse sequence protocol. It has largely replaced diagnostic ERCP for evaluating the biliary system because it carries no procedural risk.
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease, p. 342
- Mulholland and Greenfield's Surgery, p. 2788
Physics and Mechanism
The key principle is heavily T2-weighted imaging:
- Fluid has a very long T2 relaxation time. With very long echo times (TE), virtually all solid tissues lose their signal and appear dark (low intensity).
- Bile in the biliary tree, the gallbladder, and fluid in the pancreatic duct retain their signal because of their long T2 - they appear bright white on the resulting image.
- Solid material, such as a bile duct stone (choledocholithiasis), has a short T2 and appears as a well-defined dark filling defect within the bright bile duct.
- The result is a "myelogram-like" image of the ductal system, produced without any contrast injection or endoscopy.
This is analogous in principle to MR angiography, except the goal is imaging static or slow-moving fluid rather than flowing blood.
- Yamada's Textbook of Gastroenterology, p. 2745
No oral or IV contrast is required for standard MRCP. Solid structures (liver, pancreas, surrounding tissue) are suppressed and appear dark, while fluid-filled structures (ducts, gallbladder, pancreatic duct) are highlighted.
Technique and Sequences
The standard protocol uses T2-weighted sequences, acquired in two main ways:
| Acquisition Type | Description |
|---|---|
| Thick-slab (single-shot) | A single thick coronal projection (20-70 mm), acquired in one breath-hold (~1 sec). Gives a quick overview resembling a conventional cholangiogram. |
| Thin-slice 3D | Multiple thin slices (1-3 mm) acquired over several breath-holds, then reconstructed into MIP (Maximum Intensity Projection) images. Better resolution for small stones and strictures. |
Common sequences used:
- HASTE (Half-Fourier Acquisition Single-Shot Turbo Spin Echo)
- SSFSE (Single-Shot Fast Spin Echo)
- Turbo spin echo (TSE) with navigator triggering for respiratory motion
Standard parameters (example): TR ~2500-3000 ms, TE ~500-700 ms, 1 mm slice, 320×320 matrix, FOV 350 mm, coronal oblique.
Modified/Advanced MRCP Techniques
1. Secretin-Stimulated MRCP (sMRCP)
- Secretin is given IV, which stimulates exocrine pancreatic secretion, dilating the pancreatic duct and improving visualization.
- Indications: detecting pancreatic duct anomalies or strictures, characterizing communications between the pancreatic duct and pseudocysts/fistulas, evaluating sphincter of Oddi dysfunction.
- Harrison's 22e notes sMRCP as an appropriate alternative to ERCP for evaluating exocrine pancreatic function.
2. Functional (Hepatobiliary Contrast) MRCP
- IV administration of lipophilic gadolinium agents excreted by the hepatobiliary system (e.g., gadoxetate disodium / Eovist/Primovist).
- Useful for detecting post-liver transplant biliary leaks and strictures.
- Also used for post-surgical biliary anatomy evaluation.
Indications
MRCP is indicated in a wide range of pancreaticobiliary disorders:
Biliary:
- Choledocholithiasis (common bile duct stones)
- Benign biliary strictures (post-inflammatory, post-surgical)
- Malignant biliary strictures (cholangiocarcinoma, pancreatic head cancer, Klatskin tumor)
- Primary sclerosing cholangitis (PSC)
- Mirizzi syndrome
- Congenital anomalies (choledochal cysts, biliary atresia, anomalous pancreaticobiliary junction)
- Post-surgical biliary anatomy and complications (anastomotic strictures, leaks)
- IgG4-related sclerosing cholangitis
- HIV/AIDS cholangiopathy
Pancreatic:
- Pancreas divisum
- Chronic pancreatitis (irregular ductal dilation, side branch dilation)
- Pancreatic cystic tumors (IPMN, mucinous cystadenoma)
- Pancreatic pseudocysts and fistulas
- Acute pancreatitis with atypical features
General:
- Evaluation of jaundice (superior to US and CT for biliary tract obstruction)
- Suspected biliary obstruction without infection where ERCP is not immediately needed
Diagnostic Performance
| Condition | Sensitivity | Specificity |
|---|---|---|
| Choledocholithiasis | 81-100% | 96-100% |
| Biliary strictures (benign/malignant) | High | High |
MRCP is superior to conventional ultrasound and CT for detecting biliary tract obstruction. It can resolve both intra- and extrahepatic biliary structures, and it allows evaluation of the intrahepatic bile duct anatomy in detail.
- Sleisenger and Fordtran's GI and Liver Disease, p. 1341
MRCP Images
Fig. 1 - Choledocholithiasis on MRCP vs ERCP
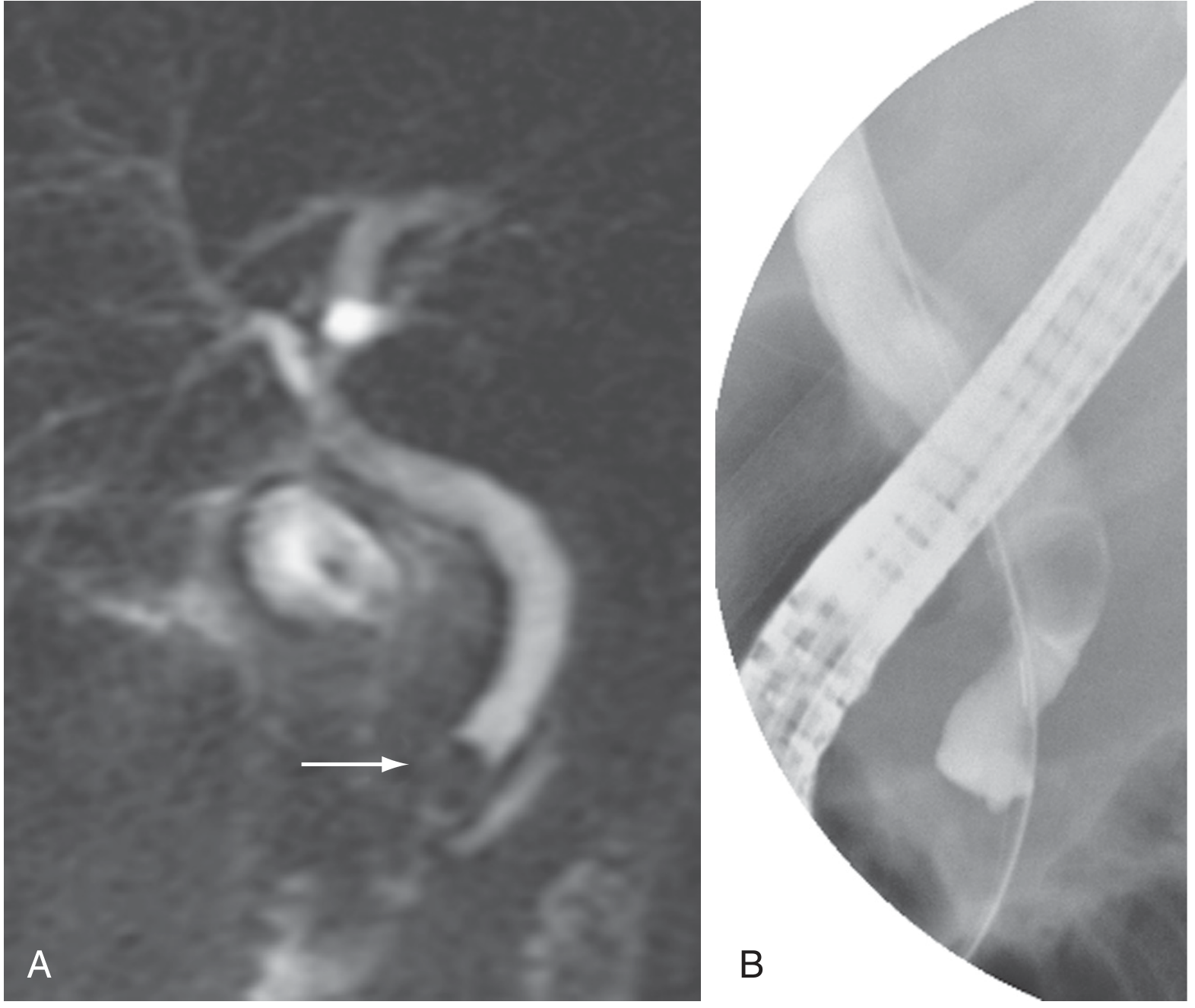
MRCP (A) shows a dark filling defect in the distal bile duct (arrow) = stone. ERCP (B) confirms the same finding. - Sleisenger and Fordtran's GI and Liver Disease
Fig. 2 - IgG4-Related Disease (Biliary Confluence Stricture)
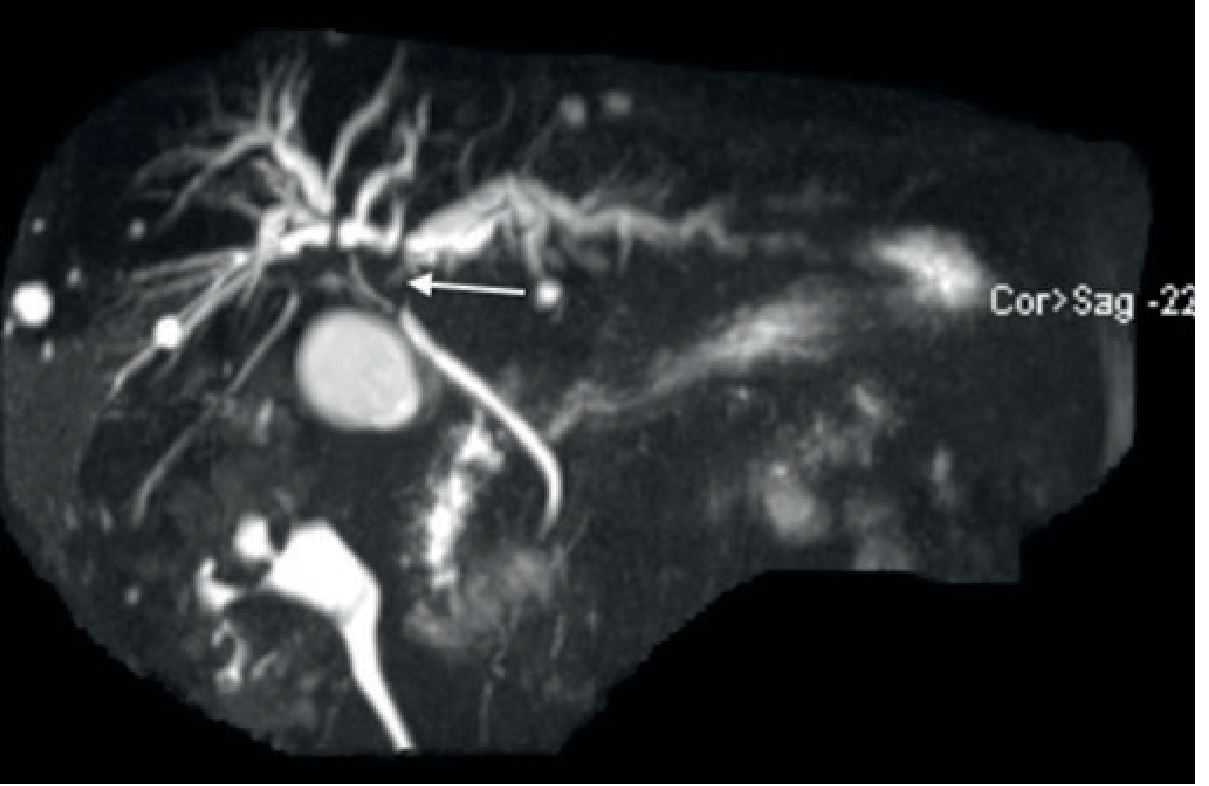
MRCP demonstrating a stricture at the biliary confluence (arrow). Differential: Klatskin tumour vs IgG4-related disease. - Grainger & Allison's Diagnostic Radiology
Fig. 3 - Mirizzi Syndrome
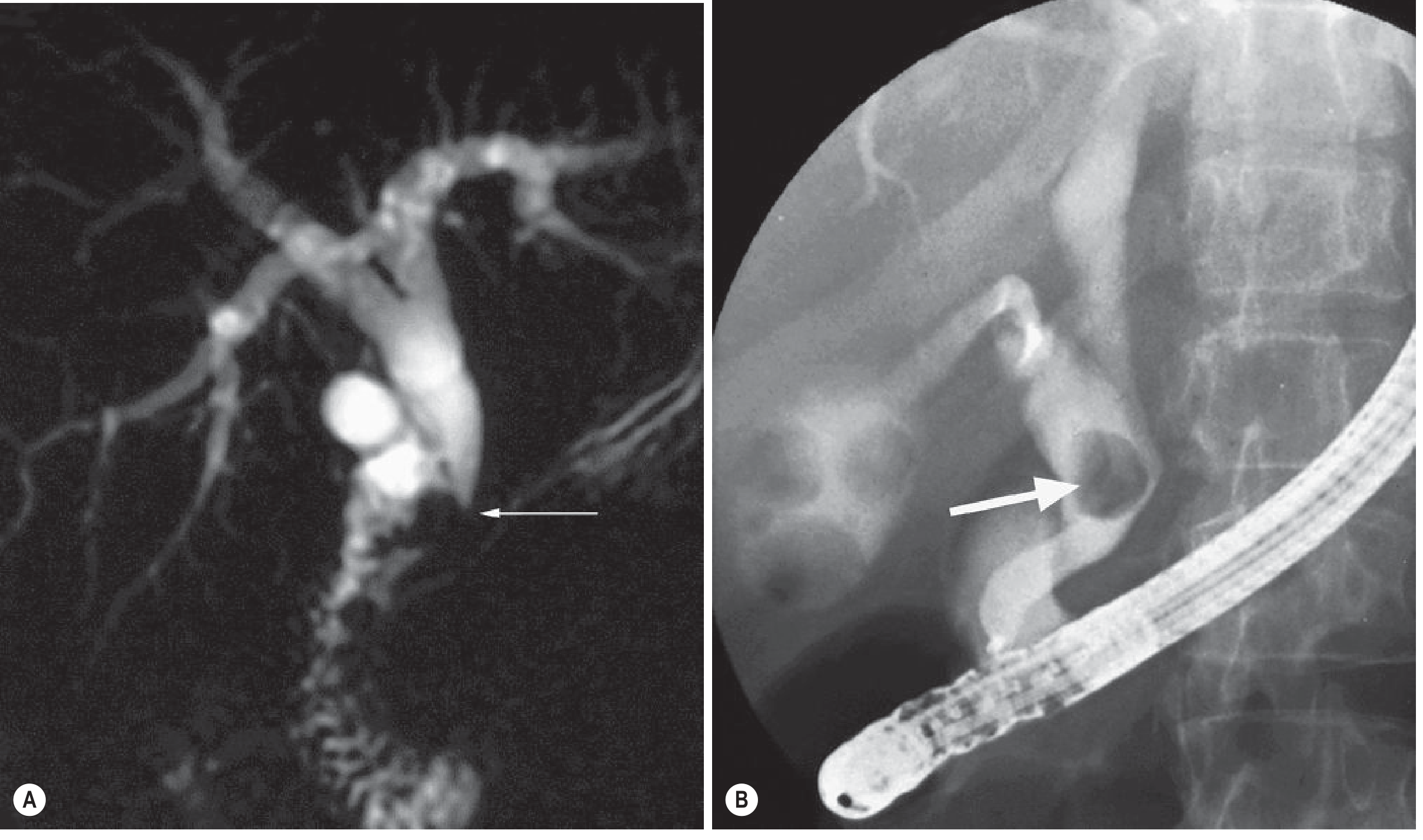
MRCP (A) shows a stricture of the lower common duct caused by a stone lying in an expanded cystic duct. ERCP (B) confirms this. Multiple gallbladder stones are also visible. - Grainger & Allison's Diagnostic Radiology
MRCP vs. ERCP - Key Comparison
| Feature | MRCP | ERCP |
|---|---|---|
| Invasiveness | Non-invasive | Invasive (endoscopic) |
| Contrast needed | None (standard) | Fluoroscopic contrast |
| Therapeutic capability | No | Yes (sphincterotomy, stone extraction, stent) |
| Complication risk | Minimal | Pancreatitis ~5%, mortality ~0.2% |
| Cost | High (comparable to ERCP) | High |
| Biliary obstruction sensitivity | 81-100% | >90% |
| Intrahepatic duct visualization | Excellent | Limited |
| Proximal lesions | Excellent | Limited |
| Tissue sampling | No | Yes (biopsy, brushings) |
Current practice: MRCP is used first for diagnostic evaluation of the biliary/pancreatic system. ERCP is reserved for cases where therapeutic intervention is anticipated or when MRCP is non-diagnostic.
Contraindications and Limitations
Absolute contraindications (MRI-related):
- Cardiac pacemakers
- Automatic implantable cardioverter-defibrillators (AICDs)
- Certain cerebral aneurysm clips
- Ferromagnetic metallic implants
Limitations:
- Cannot perform therapeutic maneuvers (stone extraction, stenting)
- Extended scan time - problematic for claustrophobic or restless patients
- Cannot stage thoracoabdominal organs simultaneously as well as CT
- Higher cost than ultrasound or CT
- Gadolinium-based contrast agents (used for functional MRCP) carry risk of nephrogenic systemic fibrosis in patients with renal failure - use lower doses or avoid in renal insufficiency
- False positives: Pneumobilia (air in the bile ducts) can mimic filling defects
- Motion artifacts if patient cannot breath-hold
- Cannot biopsy suspicious lesions
Pitfalls in Interpretation
- Pneumobilia mimics stones as dark filling defects
- Normal variants (e.g., low insertion of the cystic duct) can be misinterpreted as strictures
- Susceptibility artifacts from surgical clips after prior cholecystectomy can obscure the bile duct
- Very small stones (<3 mm) may be missed
- Papillary stenosis or sphincter of Oddi dysfunction may require secretin-stimulated MRCP for optimal assessment
Summary
MRCP is the preferred non-invasive imaging study for the pancreaticobiliary system. It exploits the long T2 relaxation of bile and ductal fluid to produce bright ductal images against a dark background, without contrast or endoscopy. It has excellent sensitivity and specificity for stones, strictures, and congenital anomalies. When therapeutic intervention is needed, ERCP follows as the next step.
This is a shared conversation. Sign in to Orris to start your own chat.