ecg showing sinus arrest, what are next step as a junior doctor
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
I now have comprehensive information from multiple authoritative sources. Here is a structured clinical response:
ECG Showing Sinus Arrest — Next Steps as a Junior Doctor
What Is Sinus Arrest?
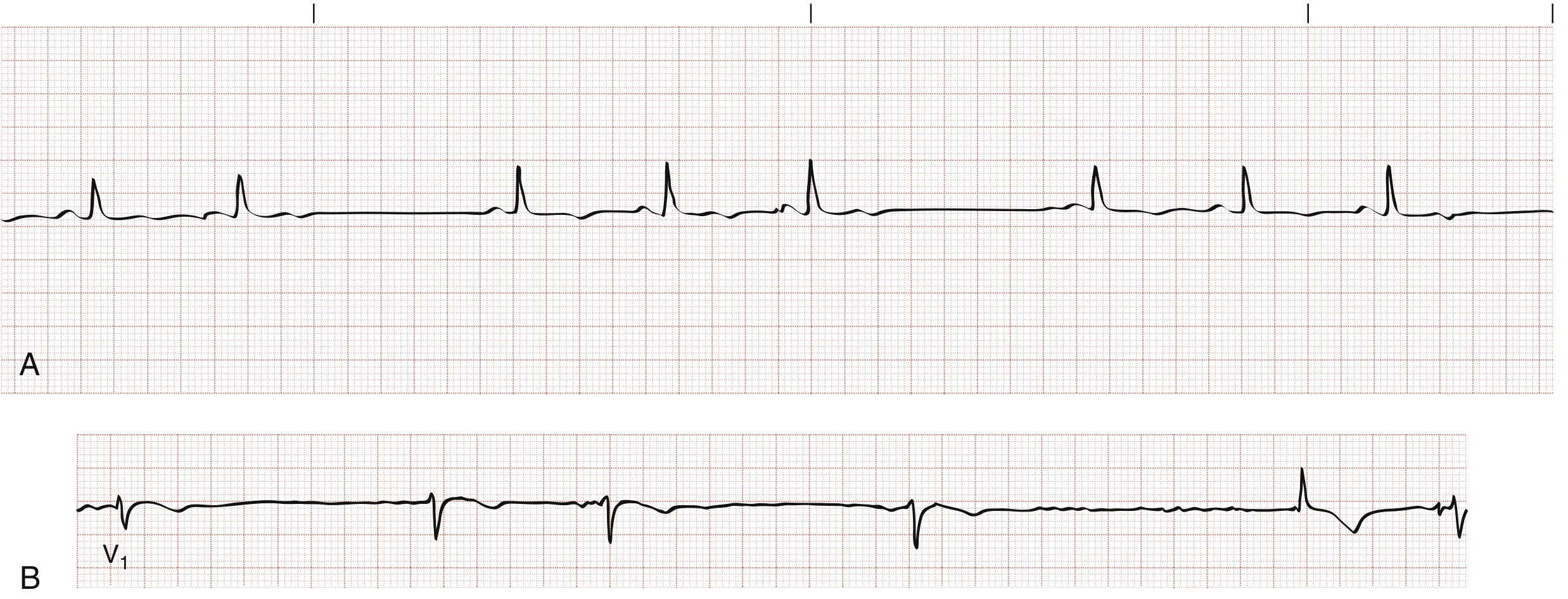
Sinus arrest = failure of the SA node to generate an impulse, producing a pause on ECG where there are no P waves and the P-P interval delimiting the pause is not a multiple of the basic P-P interval (this distinguishes it from SA exit block, where the pause is a multiple).
If no escape pacemaker fires, the result is ventricular asystole. — Braunwald's Heart Disease
Step 1: Assess the Patient Immediately (ABCDE)
Is the patient symptomatic? This is the key decision point.
| Symptomatic | Features |
|---|---|
| Haemodynamically unstable | Hypotension, syncope/pre-syncope, chest pain, acute pulmonary oedema, altered consciousness |
| Haemodynamically stable | Asymptomatic, normal BP, well-perfused |
Emergent treatment is required if HR <50–60 bpm with hypotension or hypoperfusion. A patient with a "low-normal" HR who is simultaneously in shock may also need rhythm-directed therapy. — Tintinalli's Emergency Medicine
Step 2: Call for Help
- Senior doctor/registrar immediately if patient is symptomatic or unstable
- Alert the resuscitation team if there is haemodynamic compromise or prolonged asystole
Step 3: Urgent Investigations
Run these in parallel while monitoring:
| Investigation | Rationale |
|---|---|
| 12-lead ECG (if not done) | Confirm rhythm, look for signs of inferior MI (ST elevation in II, III, aVF), AV block, ischaemia |
| Continuous cardiac monitoring | Track rate, pauses, escape rhythms |
| IV access + bloods: U&E, Mg, Ca, glucose, TFTs | Electrolyte abnormalities (hyperkalaemia), hypothyroidism |
| ABG / SpO2 | Hypoxia as a reversible cause |
| Drug history review | β-blockers, calcium-channel blockers, digoxin, amiodarone, antiarrhythmics (class I agents) are common culprits |
| Troponin / cardiac enzymes | Rule out acute MI — inferior/posterior MI can cause SA node ischaemia |
| Echo (if available) | Structural/cardiomyopathy assessment |
Step 4: Identify and Treat the Underlying Cause
Common reversible causes (the "4 H's and 4 T's" plus drug causes):
- Drugs: β-blockers, CCBs, digoxin toxicity, membrane-active antiarrhythmics, cardiac glycosides — Fuster & Hurst's The Heart
- Inferior/posterior MI: SA node ischaemia ± Bezold-Jarisch reflex — Harrison's 22E
- Excessive vagal tone: vasovagal, carotid sinus hypersensitivity, sleep apnoea
- Metabolic: hypoxia, hypothermia, hyperkalaemia, hypothyroidism
- Intrinsic disease: sick sinus syndrome (SSS), fibrosis, cardiomyopathy, myocarditis
Step 5: Acute Treatment (Symptomatic Patient)
If haemodynamically unstable:
-
Atropine 0.5–1 mg IV — repeat every 3–5 minutes, max 3 mg total
- Effective for sinus arrest because it is vagolytic, enhancing SA node automaticity — Rosen's / Braunwald's
- Not effective in post-transplant hearts (use isoprenaline 2–10 mcg/min instead)
-
If atropine fails:
- Transcutaneous pacing — most appropriate method for the acutely symptomatic patient; confirm electrical capture (paced spike + QRS) then mechanical capture (palpable pulse)
- Isoprenaline/dopamine/adrenaline infusion as a bridge to pacing
-
Transvenous pacing — if transcutaneous fails or for more prolonged support; requires specialist expertise
Drug treatment is generally a temporary bridge to pacing unless the cause is fully reversible. — Tintinalli's
Step 6: Asymptomatic / Incidental Sinus Arrest
- Transient sinus arrest (especially during sleep) may have no clinical significance if escape rhythms prevent asystole — Braunwald's
- Still requires close monitoring, investigation for reversible causes, and senior review
- Withhold/reduce offending medications if a drug cause is identified
Step 7: Disposition and Long-Term Planning
| Scenario | Management |
|---|---|
| Reversible cause found and corrected | Monitor, outpatient follow-up |
| Recurrent/symptomatic, no reversible cause | Permanent pacemaker — indicated for symptomatic sinus node disease (SSS) — Braunwald's / Rosen's |
| Tachy-Brady syndrome | Permanent pacemaker + rate-controlling therapy for tachycardia |
| Digoxin toxicity with serious features (HR <40, sinus arrest, ventricular arrhythmia) | Digoxin-specific Fab antibody fragments — Rosen's |
Quick Summary
Sinus Arrest on ECG
│
├── ASSESS: Symptomatic? (BP, GCS, perfusion)
│
├── CALL FOR HELP (senior + resus if unstable)
│
├── 12-lead ECG + monitoring + bloods + drug history
│
├── Reversible cause? → Treat it
│
├── Symptomatic/unstable?
│ ├── YES → Atropine IV → Transcutaneous pacing → Senior/ICU
│ └── NO → Monitor closely, investigate, senior review
│
└── Long-term → Permanent pacemaker if symptomatic & no reversible cause
Key sources: Rosen's Emergency Medicine; Braunwald's Heart Disease; Tintinalli's Emergency Medicine; Harrison's Principles of Internal Medicine 22E; Fuster & Hurst's The Heart
This is a shared conversation. Sign in to Orris to start your own chat.