Pharmacology about psvt and treatment
Reading File
Finding Sources
Finding Sources
Searching PubMed
"paroxysmal supraventricular tachycardia" AND treatment
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a complete pharmacology reference on PSVT and its treatment, drawn from Harrison's 22E, Braunwald's Heart Disease, Tintinalli's Emergency Medicine, Goodman & Gilman's, and the Washington Manual.
Paroxysmal Supraventricular Tachycardia (PSVT) - Pharmacology & Treatment
Definition & Mechanism
PSVT is a clinical syndrome characterized by a rapid, regular tachycardia with abrupt onset and termination. The underlying mechanism in most cases is reentry:
| Mechanism | Proportion |
|---|---|
| AV Nodal Reentrant Tachycardia (AVNRT) | ~65-80% |
| AV Reentrant Tachycardia (AVRT) via accessory pathway | ~20-30% |
| Focal Atrial Tachycardia | ~5% |
In AVNRT, a reentrant circuit is established within the dual pathway physiology of the AV node (fast and slow pathways). The slow pathway conducts antegrade and the fast pathway conducts retrograde, producing nearly simultaneous atrial and ventricular activation. In AVRT (e.g., WPW syndrome), the reentrant loop involves the AV node and an accessory pathway (Kent bundle).
- Fuster and Hurst's The Heart, 15th Edition
- Harrison's Principles of Internal Medicine 22E (2025)
ECG Features

ECG of PSVT showing rapid, regular, narrow-complex tachycardia
| Feature | Finding |
|---|---|
| QRS width | Narrow (<100 ms) unless aberrant conduction |
| Rate | 130-300 bpm (typically 170-180 bpm) |
| P waves | Buried in QRS (~70%) or retrograde P waves adjacent to QRS (~30%) |
| Onset/offset | Abrupt |
| Rhythm | Regular |
- Tintinalli's Emergency Medicine
Treatment Algorithm
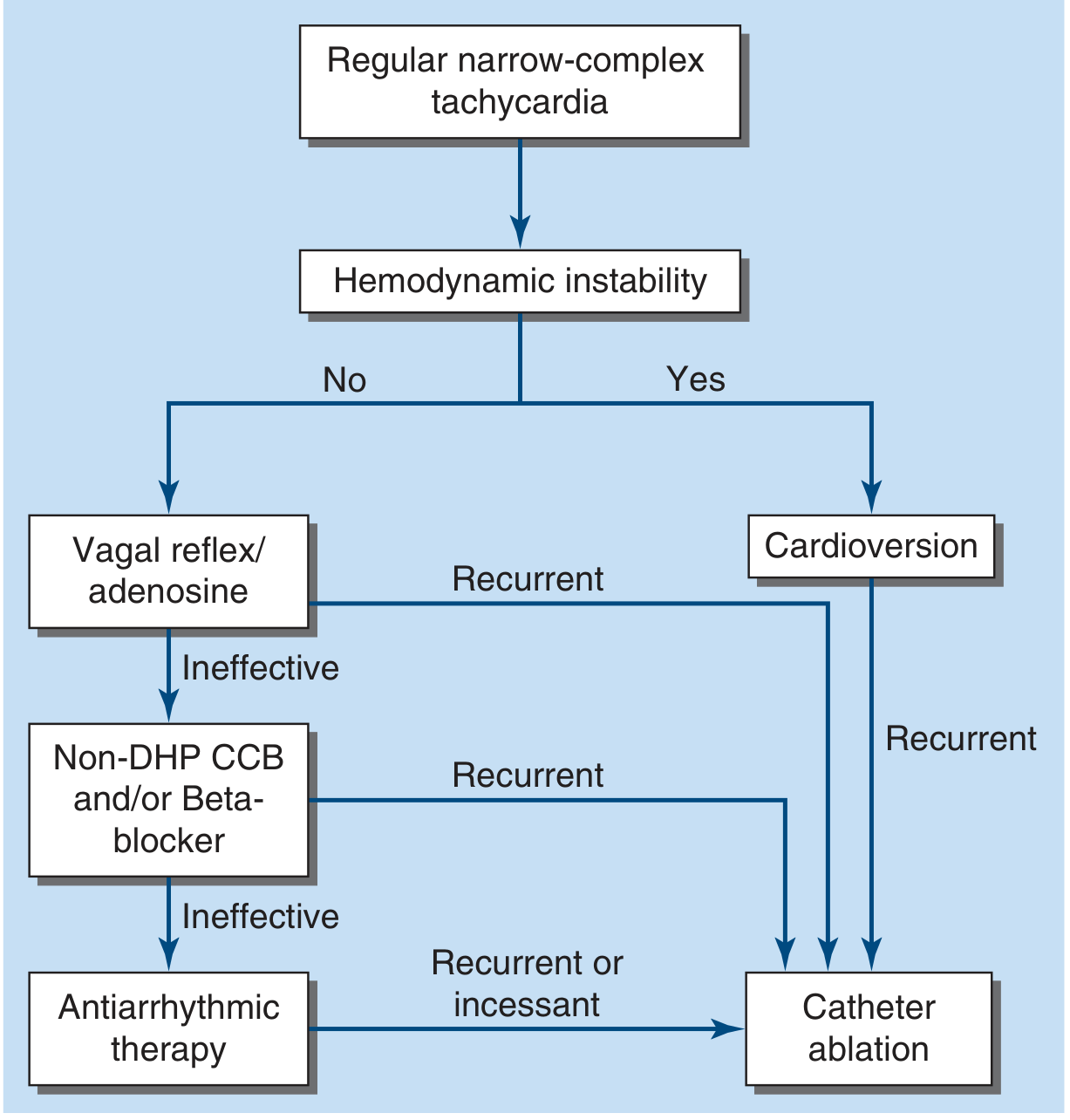
PSVT treatment algorithm - Harrison's Principles of Internal Medicine 22E (2025)
Step 1 - Hemodynamic Assessment
- Unstable (hypotension, unconsciousness, respiratory distress): Synchronized DC cardioversion (50-100 J biphasic) - immediately
- Stable: Proceed with vagal maneuvers then pharmacotherapy
Step 2 - Vagal Maneuvers (First-Line for Stable PSVT)
| Maneuver | Technique |
|---|---|
| Valsalva maneuver | Forced expiration against closed glottis; patient can self-administer |
| Modified Valsalva | Supine with legs elevated after strain phase; increases venous return and vagal tone |
| Carotid sinus massage | 5-10 sec unilateral pressure; avoid if carotid bruits or prior stroke history |
Vagal maneuvers work by transiently increasing AV nodal refractoriness, interrupting the reentry circuit. A 2024 meta-analysis (PMID 38235710) confirmed the modified Valsalva significantly improves PSVT conversion rates.
Step 3 - Pharmacotherapy
Drug 1: Adenosine (First-Choice IV Drug)
Class: Endogenous purine nucleoside; not classified in the Singh-Vaughan Williams system.
Mechanism of Action:
- Activates cardiac A1 adenosine receptors
- Increases K+ conductance via G-protein (Gi/Go) → hyperpolarization of AV nodal cells
- Antagonizes catecholamine-stimulated adenylyl cyclase → decreases cAMP, ICaL, and pacemaker current (If)
- Produces transient, profound AV nodal block (A-H interval prolongation) lasting only a few seconds
- Does NOT affect normal accessory pathways (WPW)
Pharmacokinetics:
- Half-life: 1-6 seconds (fastest acting drug in clinical use)
- Eliminated by erythrocytes and vascular endothelium via adenosine deaminase (to inosine) and phosphorylation (to AMP)
- Effects seen on first pass through circulation
Dosage (Adult):
| Dose | Route | Notes |
|---|---|---|
| 6 mg rapid IV bolus | Peripheral vein, followed by 20 mL NS flush | Initial dose |
| 12 mg IV bolus | If no response in 1-2 min | Repeat dose |
| 3 mg IV | Central line, post-transplant, or on dipyridamole | Reduced initial dose |
| Maximum single dose | 18 mg | Higher doses unlikely to work |
| Pediatric (<50 kg) | 0.05-0.3 mg/kg |
Drug Interactions:
| Drug | Effect | Action |
|---|---|---|
| Methylxanthines (theophylline, caffeine) | Competitive receptor antagonist; blocks adenosine | Increase dose |
| Dipyridamole | Blocks nucleoside transporter; prolongs adenosine effect | Decrease dose (use 3 mg) |
| Carbamazepine | Potentiates adenosine | Reduce dose |
Adverse Effects: Transient flushing, dyspnea, chest discomfort, anxiety (very brief, <30 seconds). May precipitate AF in up to 15% of patients.
Contraindications:
- 2nd or 3rd degree AV block or sick sinus syndrome (without pacemaker)
- Known hypersensitivity
- Severe bronchospasm/active wheezing (may aggravate)
- WPW with AF - AV node block will force conduction down accessory pathway, potentially causing life-threatening rapid ventricular rate; do not use
- Post-cardiac transplant patients (supersensitive - reduce dose to 3 mg)
Indications beyond PSVT: Diagnostic unmasking of AF, atrial flutter, or VT when etiology of narrow-complex tachycardia is uncertain; some right ventricular outflow tract VTs that are adrenergically driven.
- Braunwald's Heart Disease; Roberts and Hedges' Clinical Procedures in Emergency
Drug 2: Non-Dihydropyridine Calcium Channel Blockers (Verapamil, Diltiazem)
Class: Class IV antiarrhythmic (Singh-Vaughan Williams)
Mechanism of Action:
- Block L-type (ICaL) calcium channels in AV nodal tissue
- Slow AV nodal conduction and increase refractoriness
- Break reentry circuits dependent on slow-response (calcium-dependent) AV nodal tissue
Drugs and Doses:
| Drug | IV dose | Onset |
|---|---|---|
| Verapamil | 5-10 mg IV over 2 min (repeat 5-10 mg in 15-30 min) | 2-5 min |
| Diltiazem | 0.25 mg/kg IV over 2 min (repeat 0.35 mg/kg) | 2-5 min |
Oral (for long-term or "pill-in-pocket" use):
- Verapamil 40-120 mg TID or SR formulation
- Diltiazem 30-120 mg TID or extended-release formulation
Adverse Effects: Hypotension (more prolonged than adenosine), negative inotropy (caution in LV dysfunction), bradycardia.
Contraindications: WPW with AF/flutter (same risk as adenosine; may accelerate conduction down accessory pathway), decompensated heart failure, severe hypotension.
Drug 3: Beta-Blockers
Class: Class II antiarrhythmic
Mechanism of Action:
- Block beta-1 adrenergic receptors in AV node
- Reduce sympathetic enhancement of AV nodal conduction
- Slow AV nodal conduction, prolong ERP of AV node
- Effective in AVNRT by interrupting the reentrant circuit
Drugs and Doses (acute IV):
| Drug | IV Dose |
|---|---|
| Metoprolol | 5 mg IV over 5 min (can repeat x3) |
| Esmolol | 500 mcg/kg loading dose, then 50-200 mcg/kg/min infusion (very short-acting) |
| Atenolol | 5 mg IV over 5 min |
Oral (chronic suppression): Metoprolol succinate, atenolol, propranolol.
Adverse Effects: Hypotension, bradycardia, bronchospasm (avoid in reactive airway disease), negative inotropy.
Drug 4: Procainamide
Class: Class IA antiarrhythmic
Mechanism: Slows conduction velocity, decreases automaticity and excitability in atrial, ventricular, and Purkinje tissue; increases refractoriness; prolongs QT interval.
Use in PSVT: Reserved for wide-complex tachycardia where PSVT with aberrancy vs VT is unclear, or for WPW-related preexcited tachycardias.
Dose: 20-50 mg/min IV until arrhythmia terminates, hypotension occurs, QRS widens >50%, or total 17 mg/kg.
Contraindications: 2nd/3rd degree AV block, SLE, prolonged QT, severe LV dysfunction.
Drug 5: Antidromic AVRT / Preexcited AF (WPW) - Special Case
In antidromic AVRT or preexcited AF with WPW, standard AV-nodal blocking agents (adenosine, verapamil, diltiazem, digoxin) are contraindicated because they may enhance antegrade accessory pathway conduction and precipitate ventricular fibrillation.
Preferred agents:
- Ibutilide (IV) - prolongs refractoriness of accessory pathway
- Procainamide (IV)
- Flecainide (IV or oral; Class IC)
- DC cardioversion (if unstable)
Chronic/Long-Term Pharmacotherapy
| Arrhythmia | First Choice | Alternative |
|---|---|---|
| AVNRT | Beta-blockers, Non-DHP CCB, digoxin | Flecainide, propafenone, sotalol, amiodarone |
| Orthodromic AVRT | Beta-blockers, Non-DHP CCB | Flecainide, propafenone |
| Antidromic AVRT / WPW | Catheter ablation preferred | Flecainide, procainamide |
Note: Catheter ablation is the definitive treatment and is preferred for recurrent, symptomatic PSVT. Success rates: AVNRT ~96%, AVRT ~95%, with rare complications. Most patients with recurrent episodes are candidates for ablation.
- Washington Manual of Medical Therapeutics
Quick Drug Summary Table
| Drug | Class | Mechanism | Route | Key Caution |
|---|---|---|---|---|
| Adenosine | Purine nucleoside | A1 receptor → ↑K+ conductance, ↓AV conduction | IV bolus only | WPW+AF, theophylline antagonism |
| Verapamil | Class IV CCB | Block ICaL in AV node | IV / oral | Hypotension, WPW+AF |
| Diltiazem | Class IV CCB | Block ICaL in AV node | IV / oral | Hypotension, heart failure |
| Metoprolol/Esmolol | Class II β-blocker | Block β1 → slow AV conduction | IV / oral | Bronchospasm, hypotension |
| Procainamide | Class IA | Na+ channel block, ↓conduction | IV | QT prolongation, lupus-like syndrome |
| Flecainide | Class IC | Na+ channel block | IV / oral | Structural heart disease contraindicated |
| Ibutilide | Class III | ↑refractoriness via K+ channels | IV | QT prolongation, polymorphic VT |
Key Teaching Points
- Adenosine is drug of first choice for acute termination of stable PSVT - give rapidly as IV bolus followed by 20 mL NS flush because its half-life is only 1-6 seconds.
- Theophylline/caffeine blocks adenosine receptors (competitive antagonism); dipyridamole potentiates adenosine (blocks its uptake).
- Never use AV-nodal blockers (adenosine, verapamil, diltiazem, digoxin) in WPW with AF/flutter - risk of VF.
- Wide-complex tachycardia should be treated as VT until proven otherwise.
- Catheter ablation is the definitive cure for recurrent PSVT with >95% success rate.
Sources: Harrison's Principles of Internal Medicine 22E (2025, McGraw Hill); Braunwald's Heart Disease; Tintinalli's Emergency Medicine; Roberts and Hedges' Clinical Procedures in Emergency Medicine; Washington Manual of Medical Therapeutics; Goodman & Gilman's Pharmacological Basis of Therapeutics
This is a shared conversation. Sign in to Orris to start your own chat.