Cephalohematoma
Reading File
Finding Sources
Searching PubMed
cephalohematoma newborn birth trauma
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Here is a thorough overview of cephalohematoma based on authoritative textbook sources.
Cephalohematoma
Definition and Anatomy
A cephalohematoma is a subperiosteal collection of blood in the newborn, occurring between the periosteum and the outer surface of the skull bone. It is caused by rupture of the diploic and/or emissary veins, typically as a result of birth trauma.
Because the periosteum adheres tightly to the various suture lines, the hemorrhage is strictly confined and does not cross suture lines - this is the defining anatomical feature that distinguishes it from other birth-related scalp injuries.
- Rosen's Emergency Medicine, p. 3138
- Fitzpatrick's Dermatology, Vol. 1
Anatomical Diagram
The diagram below shows where cephalohematoma sits relative to other birth-related scalp injuries:
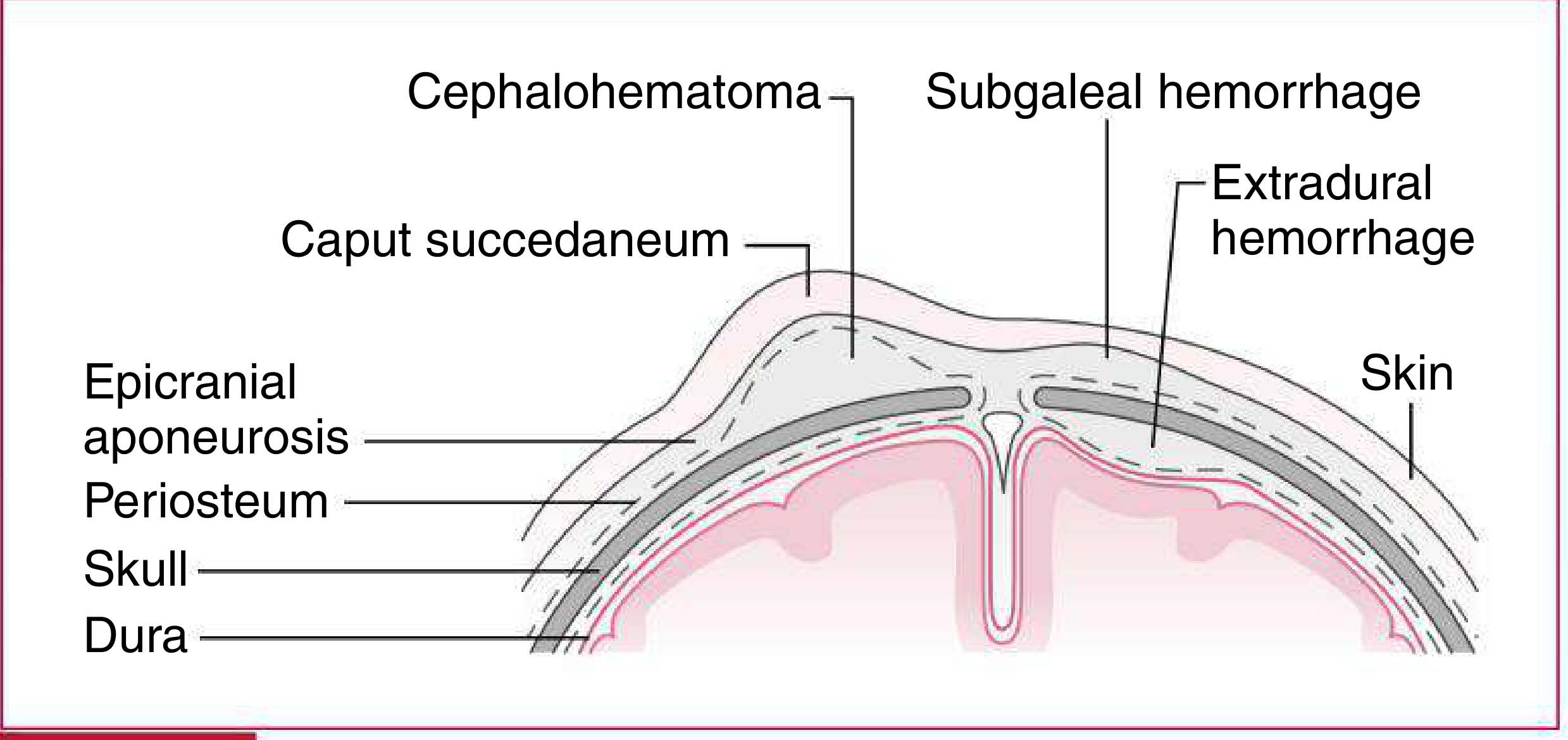
Harriet Lane Handbook, 23rd ed. - Types of extradural fluid collections in newborn infants
Comparison: Birth-Related Extradural Fluid Collections
The table below (from Harriet Lane Handbook) contrasts the three main entities:
| Feature | Caput Succedaneum | Cephalohematoma | Subgaleal Hemorrhage |
|---|---|---|---|
| Location | At point of contact; can extend across sutures | Usually over parietal bones; does not cross sutures | Beneath epicranial aponeurosis; may extend to orbits or nape of neck |
| Findings | Vaguely demarcated; pitting edema, shifts with gravity | Distinct margins; initially firm, more fluctuant after 48 hr | Firm to fluctuant, ill-defined borders; may have crepitus or fluid waves |
| Timing | Maximal at birth; resolves in 48-72 hr | Increases after birth for 12-24 hr; resolution over weeks | Progressive after birth; resolution over weeks |
| Severity | Minimal | Rarely severe | May be severe, especially with associated coagulopathy |
Harriet Lane Handbook, 23rd ed., Table 18.3
Etiology and Risk Factors
- Birth trauma - the most common cause
- Vacuum extraction - particularly associated with cephalohematoma formation
- Forceps delivery - a less common but recognized association
Clinical Features
- Appears as a firm, well-delimited swelling, usually over one parietal bone (unilateral)
- Does not cross suture lines (key distinguishing feature)
- Increases in size over the first 12-24 hours after birth as blood continues to accumulate, then gradually resolves
- Becomes more fluctuant after 48 hours
- Usually unilateral, though bilateral cases occur
Complications
- Neonatal jaundice (hyperbilirubinemia) - as the hematoma resorbs, breakdown of red blood cells releases bilirubin, which can contribute to or worsen neonatal jaundice
- Calcification - the hematoma may calcify rather than fully resorb, leaving a hard bony prominence; this usually remodels over months to years
- Underlying skull fracture - a linear skull fracture may be present beneath the hematoma; clinically significant in a minority of cases
- Infection/abscess - rare but recognized complication; aspiration should be avoided due to infection risk
Management
- Conservative (watchful waiting) is the standard approach for uncomplicated cases
- The lesion resolves spontaneously over several weeks to a few months
- Do not aspirate - aspiration risks introducing infection with no clinical benefit in most cases
- Monitor for jaundice and treat hyperbilirubinemia if significant (phototherapy as needed)
- If an underlying skull fracture is suspected clinically, imaging (skull X-ray or CT) may be warranted
- Reassure parents that calcification, if it occurs, typically remodels with skull growth
Key Differentiating Points (Quick Reference)
| Feature | Cephalohematoma | Caput Succedaneum |
|---|---|---|
| Layer | Subperiosteal | Subcutaneous |
| Suture lines | Does NOT cross | Crosses freely |
| Onset | Appears hours after birth | Present at birth |
| Consistency | Firm, then fluctuant | Soft, pitting edema |
| Resolution | Weeks | 48-72 hours |
Sources:
- Fitzpatrick's Dermatology, Vol. 1 - "Caput Succedaneum and Cephalohematoma"
- Harriet Lane Handbook, 23rd ed. - Table 18.3, Figure 18.3
- Rosen's Emergency Medicine - "Scalp Injuries," p. 3138
This is a shared conversation. Sign in to Orris to start your own chat.