Limb salvage surgery in malignant tumors explain in detail with appropriate illustrative diagrams and images
Reading File
Finding Sources
Finding Sources
Searching the Web
limb salvage surgery malignant bone tumors techniques principles 2024
Finding Sources
Finding Sources
Reading Web Page
limb salvage surgery malignant tumors techniques reconstruction indications contraindications
Reading File
Reading File
Searching PubMed
limb salvage surgery bone sarcoma outcomes
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Now I have comprehensive textbook content and intraoperative images. Let me compile the full detailed answer.
Limb Salvage Surgery in Malignant Tumors
1. Introduction and Historical Context
Limb salvage surgery (LSS) - also called limb-sparing surgery - encompasses all surgical procedures designed to remove a malignant tumor from an extremity while preserving a functional limb with acceptable oncologic, functional, and cosmetic outcomes. It stands in contrast to amputation, which was historically the standard treatment for bone and soft-tissue sarcomas.
Prior to the 1980s, amputation was the norm. The shift to limb salvage was made possible by three advances working in concert:
- Effective neoadjuvant chemotherapy (especially for osteosarcoma) - shrank tumors preoperatively and addressed micrometastases
- Advanced cross-sectional imaging (CT, MRI) - allowed precise tumor mapping and surgical planning
- Improved reconstructive techniques - metal endoprostheses, allografts, and vascular/soft tissue flaps
With multimodal treatment (surgery + chemotherapy), long-term survival for osteosarcoma patients improved from approximately 20% to 70%.
2. Tumors Amenable to Limb Salvage
Bone malignancies:
- Osteosarcoma (most common; limb salvage is now the standard of care)
- Chondrosarcoma
- Ewing sarcoma
- Adamantinoma
- Malignant giant cell tumor of bone
Soft-tissue malignancies:
- Malignant fibrous histiocytoma (undifferentiated pleomorphic sarcoma)
- Fibrosarcoma
- Liposarcoma
- Rhabdomyosarcoma
- Synovial sarcoma
3. Fundamental Oncologic Principle: Surgical Margins
The single most important determinant of local control is achieving a wide (R0) surgical margin. The Enneking staging system defines surgical margin planes:
| Margin Type | Definition | Use |
|---|---|---|
| Intralesional | Plane passes through the tumor | Benign only (e.g., giant cell tumor, ABC) |
| Marginal | Plane passes through the reactive zone (satellites of tumor cells present) | Atypical lipomas, well-differentiated liposarcoma |
| Wide | Entire tumor + cuff of normal tissue surrounding it | Standard for LSS in malignancy |
| Radical | Entire anatomic compartment resected | Rare; used for highly aggressive tumors |
Wide margin in practice: Bone resection margin is at least 3 cm beyond the tumor edge as defined by MRI. A sleeve of normal muscle, fat, and soft tissue surrounds the specimen. The biopsy tract must be excised en bloc with the tumor.
4. Indications for Limb Salvage Surgery
Limb salvage is appropriate when two non-negotiable criteria are met (Miller's Review of Orthopaedics):
- Local control must be at least equal to that achievable by amputation
- The remaining limb must be functional
Specific indications (Osteosarcoma Guidelines):
- Enneking stage IIA, IIB (chemotherapy-sensitive), stage III with controllable metastases
- Good chemotherapy response even with pathologic fracture in select cases
- Wide excision margins can be achieved
- Main neurovascular bundle is not involved
Contraindications:
- Major neurovascular bundle involvement (absolute)
- Displaced pathologic fracture with tumor cell contamination
- Biopsy complications (infection, hematoma, joint contamination, poorly placed incision)
- Recurrent tumor at the same site
- Relative: Very young skeletally immature patients (addressed with expandable prostheses)
5. Preoperative Planning
Staging Workup
Before any biopsy, complete staging is required:
- MRI of the entire affected bone (whole-bone MRI to detect skip lesions)
- CT chest for pulmonary metastases
- Bone scan (technetium-99m) for polyostotic disease
- PET-CT for systemic staging
- Laboratory studies (CBC, ESR, LDH, alkaline phosphatase)
Biopsy Principles
The biopsy is as important as the definitive procedure. Key rules:
- Refer to an orthopaedic oncology specialist before biopsy
- The biopsy track is contaminated with tumor cells and must be excised en bloc with the specimen
- Use longitudinal incisions (transverse incisions cannot be excised)
- Go through a single muscle compartment - do not contaminate intermuscular planes
- Avoid neurovascular structures
- Sample the soft-tissue extension (most viable tumor for diagnosis)
- Use core needle biopsy (84-98% diagnostic accuracy) when possible
- If a bone window is made, make it oval/round, then plug with methacrylate
- Deflate tourniquet and achieve meticulous hemostasis before closure
Digital Preoperative Planning
Computer-assisted 3D surgical planning using CT/MRI data is now standard, allowing precise tumor resection planning and custom prosthesis design.
6. Neoadjuvant (Preoperative) Therapy
For high-grade bone sarcomas (especially osteosarcoma), neoadjuvant chemotherapy is given before surgery:
- Regimens: MAP (Methotrexate, Adriamycin/doxorubicin, Cisplatin) or similar
- Goals: Reduce tumor volume, facilitate limb salvage, address micrometastases, allow assessment of chemotherapy response
- Surgery is performed within 3 weeks of completing chemotherapy
- If the tumor grows >30% of maximum diameter or breaks through the pseudocapsule during chemotherapy, surgery proceeds immediately
Chemotherapy response grading (Huvos system):
- Grade I: Little/no effect
- Grade II: Some necrosis but viable tumor remains
- Grade III: >90% necrosis
- Grade IV: Complete necrosis (best prognosis)
Radiation therapy plays a limited role for most bone tumors (which are relatively radio-resistant), but is used for:
- Ewing sarcoma, lymphoma, myeloma (radiosensitive)
- Soft-tissue sarcomas: pre- or post-op to enable marginal resection instead of amputation
- Brachytherapy catheters placed at time of resection for high local dose delivery
7. Surgical Techniques of Reconstruction
After en bloc tumor resection, reconstruction of the resulting bone and soft-tissue defect is required. The choice depends on tumor site, patient age, bone quality, and extent of resection.
7A. Tumor Endoprosthesis (Metallic Megaprosthesis) - Most Common
The most widely used reconstruction technique for periarticular resections in adults. A custom or modular metal implant replaces the resected bone segment and joint.
Advantages: Immediate weight-bearing, reliable function, no risk of disease transmission
Disadvantages: Risk of aseptic loosening, infection, mechanical failure; may require revision
Disadvantages: Risk of aseptic loosening, infection, mechanical failure; may require revision
Applications by site:
- Distal femur (most common): Rotating hinged custom or assembled prosthesis; stem must be ≥12 cm
- Proximal femur: Bipolar hemiarthroplasty replacement
- Proximal tibia: Requires gastrocnemius muscle flap for soft-tissue coverage and extensor mechanism reconstruction
- Proximal humerus: Half-shoulder (hemiarthroplasty); Malawer type I resection is standard
Expandable prostheses: Used in skeletally immature children to accommodate growth (can be expanded 1-1.5 cm at a time non-invasively).
Intraoperative view of distal femur resection and endoprosthetic reconstruction:
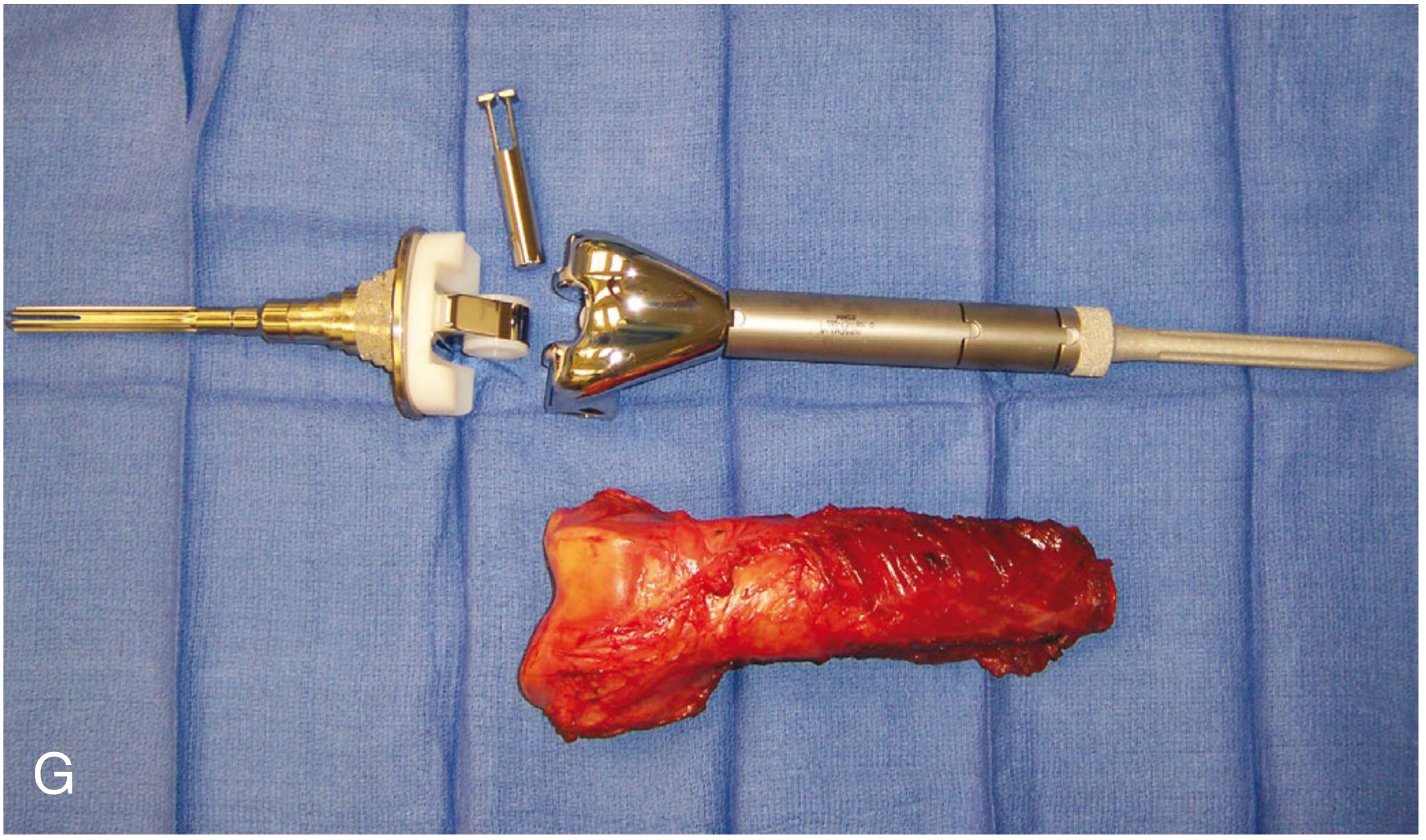
Above: The resected distal femur specimen (bottom) compared alongside the assembled modular tumor endoprosthesis (top) - Campbell's Operative Orthopaedics 15th Ed, Fig. 26.43G
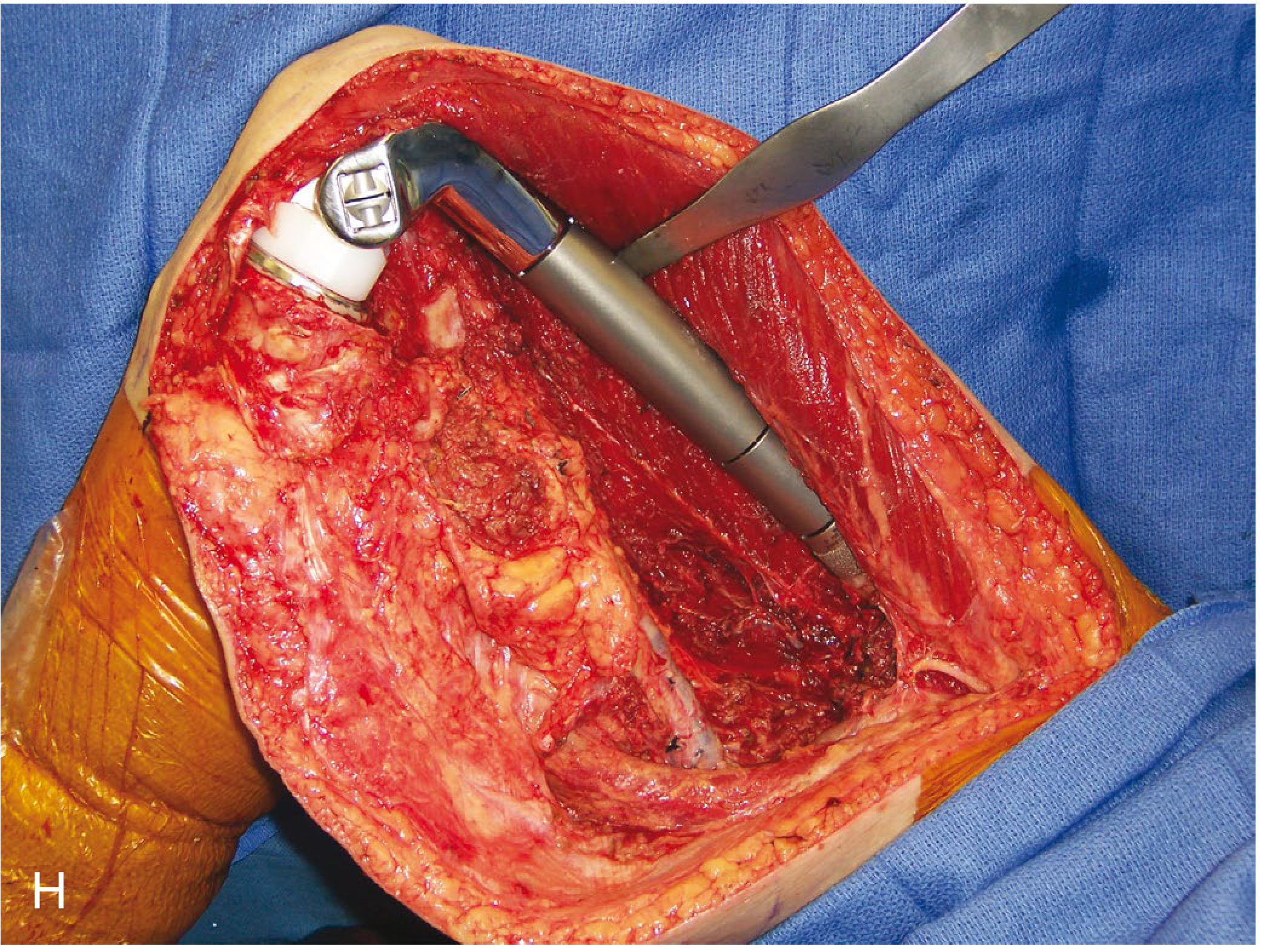
Above: Endoprosthesis being trialed in situ during distal femur reconstruction - Campbell's Operative Orthopaedics 15th Ed, Fig. 26.43H
7B. Osteoarticular Allograft
Cadaveric bone graft used to reconstruct the resected segment including the articular surface. This preserves the biological joint surface and allows reattachment of ligaments and tendons.
Advantages: Biologic reconstruction; natural joint surface; tendon/ligament can be sutured to allograft
Disadvantages: Risk of allograft fracture (10-20%), nonunion at host-allograft junction, infection, disease transmission, late joint collapse
Disadvantages: Risk of allograft fracture (10-20%), nonunion at host-allograft junction, infection, disease transmission, late joint collapse
Use: Around the knee, proximal tibia, proximal humerus in younger patients
7C. Allograft-Prosthesis Composite (APC)
A hybrid technique combining a metallic endoprosthesis with a cortical allograft sleeve. The prosthesis provides stability while the allograft allows soft tissue (tendons, ligaments) reattachment. Useful when bone stock is insufficient for standard prosthesis fixation.
7D. Allograft Arthrodesis
An intercalary allograft replaces the resected segment and the joint is fused (arthrodesed). Fixed with an intramedullary nail plus plates at the allograft-host junctions.
Result: Stable but stiff limb
Complications: High complication rates (nonunion, fracture, infection)
Use: Around the knee in patients who require heavy labor or sports participation
Complications: High complication rates (nonunion, fracture, infection)
Use: Around the knee in patients who require heavy labor or sports participation
7E. Intercalary Reconstruction (Diaphyseal Tumors)
When only the diaphysis (shaft) is involved and the joint can be preserved:
- Intercalary allograft (cortical strut graft) fixed with intramedullary nail
- Vascularized fibula graft - provides living bone with blood supply, especially valuable in children; can be combined with allograft ("biological reconstruction")
- Extracorporeal radiation therapy (ECRT): The resected tumor bone is irradiated ex vivo (50-300 Gy single fraction), sterilized, and reimplanted. Provides anatomically perfect size-matched autograft; preserves joint; economical. Can be combined with vascularized or non-vascularized fibular graft.
7F. Rotationplasty (Van Nes Procedure)
A specialized option for large tumors of the distal femur or proximal tibia in children. The tumor-bearing segment is resected; the remaining lower leg is rotated 180° and the ankle joint functions as the new knee joint. A below-knee prosthesis is fitted.
Advantages: Biologically superior function; no metal implant; accommodates growth
Disadvantages: Significant body image concerns; unconventional appearance
Best suited to: Young children with large tumors where conventional prosthesis would fail with growth
Disadvantages: Significant body image concerns; unconventional appearance
Best suited to: Young children with large tumors where conventional prosthesis would fail with growth
8. Specific Anatomic Sites
8A. Distal Femur (Most Common Site - Osteosarcoma)
The distal femur accounts for the majority of osteosarcoma cases. Pre-chemotherapy X-rays show the classic aggressive periosteal reaction, Codman's triangle, and sunburst pattern:

Above: AP and lateral X-ray of osteosarcoma of the distal femur prior to resection - Campbell's Operative Orthopaedics 15th Ed, Fig. 26.43A-B
Surgical steps (Technique 26.17):
- Lateral approach to the femur
- Wide dissection to include the biopsy tract en bloc
- Neurovascular structures (popliteal vessels, sciatic nerve) identified and preserved
- Bone cut at least 3 cm proximal to tumor margin confirmed by intraoperative fluoroscopy
- Specimen removed; length measured
- Femoral canal reamed; minimum 12-cm stem prosthesis
- Tibial cut perpendicular to tibial axis; trial components placed
- Cement fixation; close over drains
- Local/free flaps as needed for soft-tissue coverage
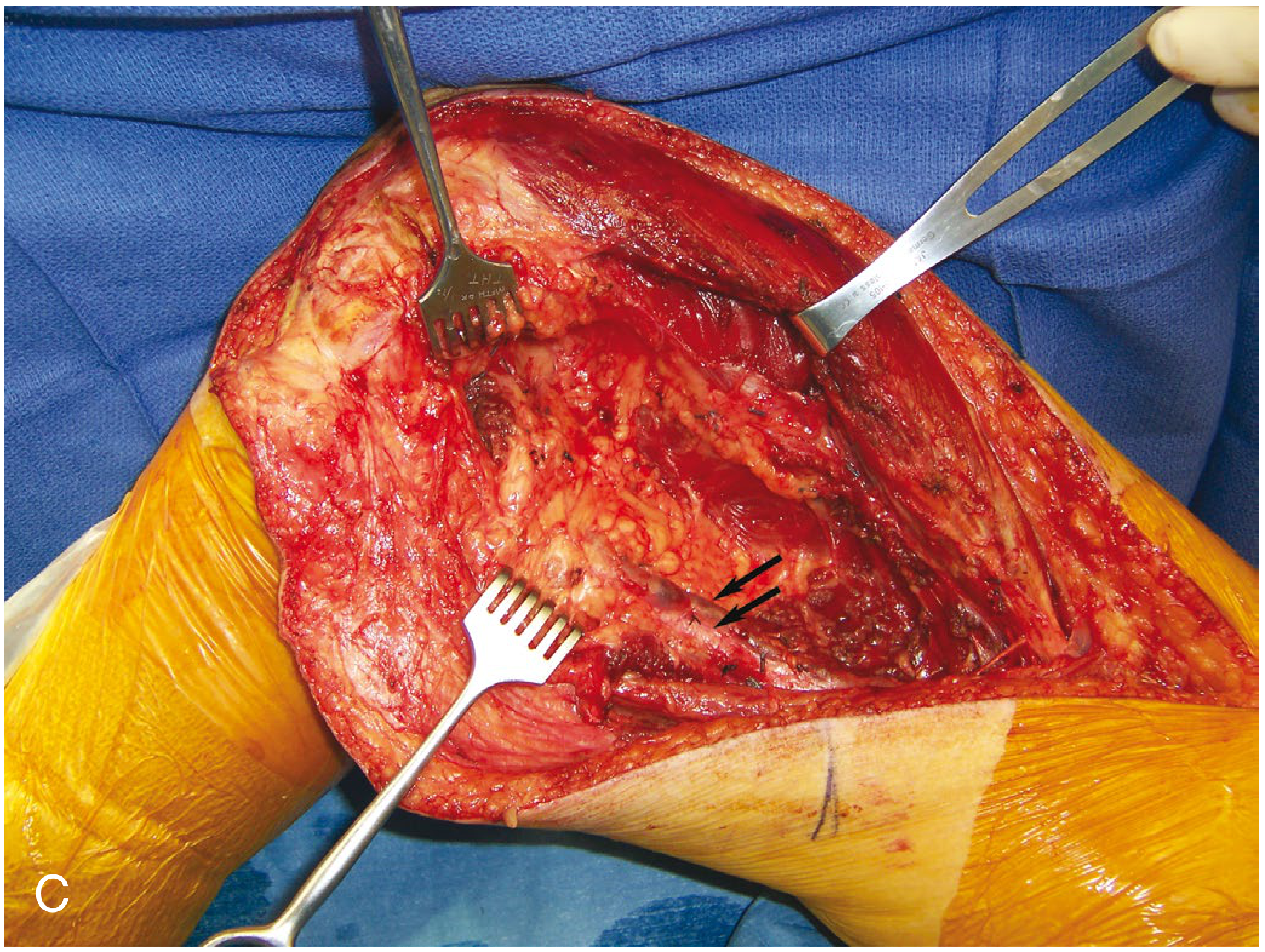
Intraoperative exposure:
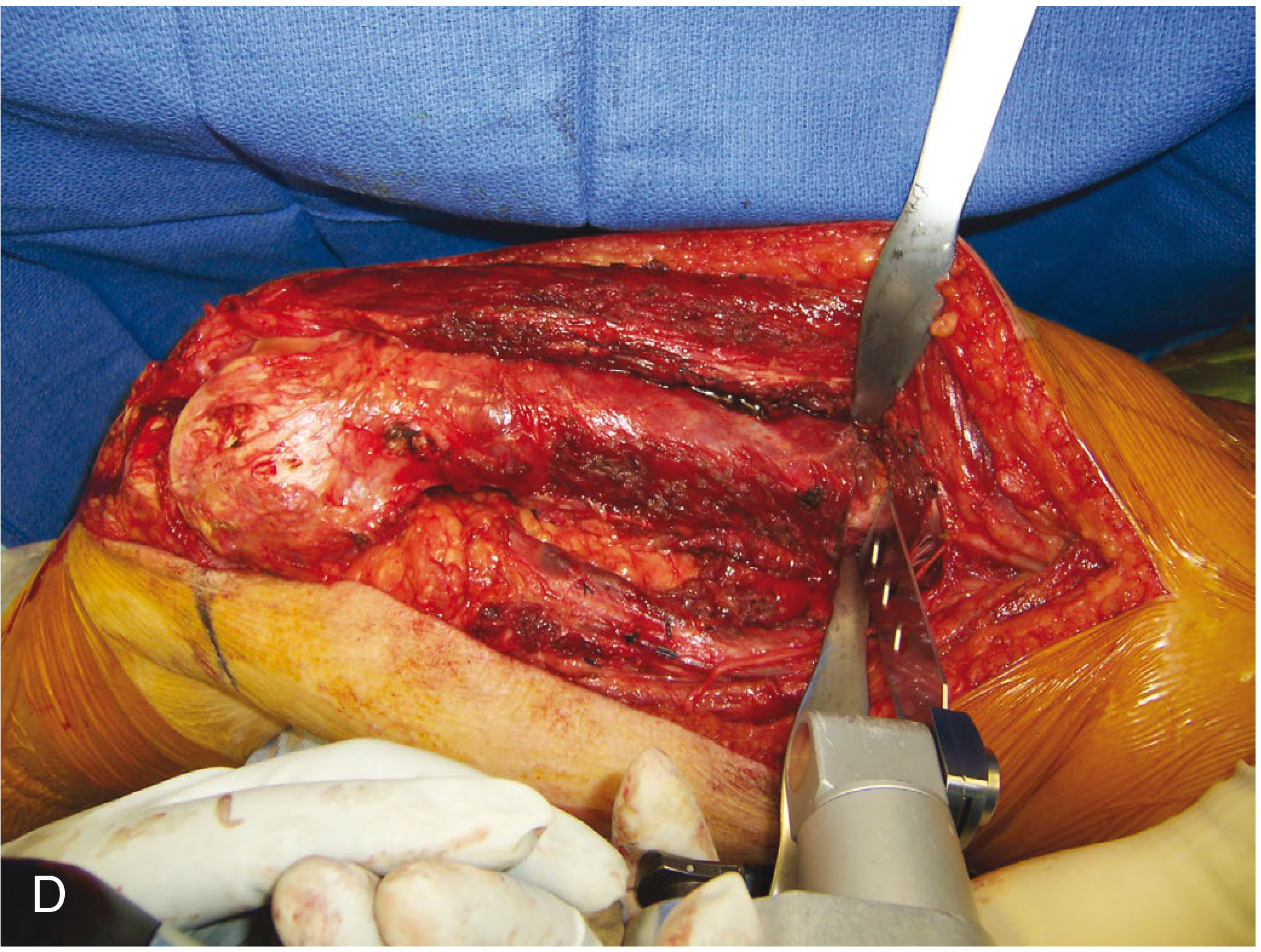
Above: Wide surgical exposure during distal femur osteosarcoma resection, showing tumor mass and adjacent structures - Campbell's Operative Orthopaedics 15th Ed
Above: Intraoperative osteotomy during distal femur resection - Campbell's Operative Orthopaedics 15th Ed
Local recurrence rate: 5-10% after wide resection = equivalent to transfemoral amputation. No survival advantage has been demonstrated for amputation over limb salvage when wide margins are obtained.
8B. Proximal Tibia (2nd Most Common Site)
- Historically treated with knee disarticulation (children) or long transfemoral amputation (adults)
- Now: Endoprosthetic reconstruction with routine gastrocnemius flap for extensor mechanism reconstruction and soft-tissue coverage
- Contraindications: Popliteal vessel involvement, displaced pathologic fracture, joint contamination from biopsy, recurrent tumor
- A mobile knee with active extension is an achievable goal
8C. Proximal Femur
- Bipolar hemiarthroplasty most common
- Hip abductor muscle sacrifice leads to Trendelenburg gait - a significant functional limitation
8D. Proximal Fibula (Malawer Technique)
- Wide local resection with sacrifice of common peroneal nerve (leads to foot drop)
- Popliteal vessels and tibial nerve preserved
- Vascular supply to the extremity maintained via posterior tibial artery
8E. Proximal Humerus and Upper Extremity
- Even with sacrifice of one or two major nerves, upper extremity limb salvage provides better function than prosthetic fitting after amputation
- Malawer type I resection (intraarticular) is standard for proximal humeral tumors
- Reconstruction: Half-shoulder prosthesis or allograft-prosthesis composite
Example: Proximal humeral osteosarcoma before and after limb salvage with plate fixation reconstruction:
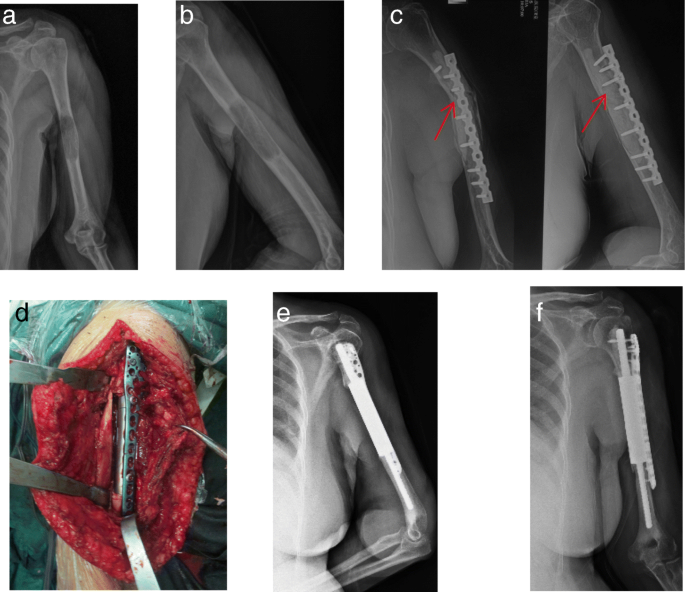
Above: Proximal humeral sarcoma (a-b), failed fixation at follow-up shown by red arrows (c), intraoperative view of reconstruction (d), and post-op X-rays at 6 months (e) and 12 months (f)
9. Soft-Tissue Reconstruction
After bone resection, adequate soft-tissue coverage is essential:
- Local muscle flaps: Gastrocnemius flap (standard for proximal tibia); vastus lateralis flap
- Free flaps: Latissimus dorsi, rectus abdominis for large defects
- Rotational fasciocutaneous flaps: For wound coverage
Neoadjuvant radiation can hinder wound healing; in these cases a non-irradiated tissue flap is required.
10. Four Key Questions When Deciding Limb Salvage vs. Amputation
(Campbell's Operative Orthopaedics, 15th Ed)
| Question | Evidence |
|---|---|
| 1. Survival difference? | No study proves survival advantage of amputation over LSS when wide margins are achieved; local recurrence rate is equivalent (5-10%) |
| 2. Morbidity comparison? | LSS has greater perioperative and long-term morbidity (infection, wound dehiscence, DVT, flap necrosis, blood loss); amputation requires fewer re-operations acutely |
| 3. Functional outcomes? | Patients with prosthetic knee replacement show higher walking velocity and more efficient gait vs. transfemoral amputees; upper extremity LSS almost always functionally superior |
| 4. Psychosocial outcomes? | LSS patients have less early anxiety, better body image; amputees may equalize at 2-5 year follow-up with good rehabilitation support |
Important caveat: After initially successful limb salvage, one-third of long-term survivors may ultimately require amputation due to complications (infection, mechanical failure, local recurrence, nonunion).
11. Complications
| Category | Specific Complications |
|---|---|
| Early | Wound dehiscence, hematoma, infection, flap necrosis, DVT/PE, blood loss, nerve injury |
| Implant-related | Aseptic loosening, periprosthetic fracture, mechanical failure, bushing wear |
| Biological reconstruction | Allograft fracture, nonunion at host-allograft junction, late graft collapse |
| Oncologic | Local recurrence (5-10%), requiring revision or amputation |
| Growth | Leg length discrepancy in children (addressed with expandable prostheses) |
| Radiation-related | Radiation sarcoma (~10 year lag), osteonecrosis, pathologic fracture (29% at 5 years in thigh treated with RT + wide resection with periosteal stripping) |
12. Outcomes and Prognosis
- Local recurrence rate: 5-10% for distal femur osteosarcoma after LSS (equivalent to transfemoral amputation)
- 5-year survival (osteosarcoma with limb salvage + chemotherapy): ~65-75%
- Functional outcomes (MSTS/TESS scores): Generally good to excellent for distal femur and proximal humeral reconstructions; proximal femoral reconstructions have more functional compromise due to abductor sacrifice
- A 2023 meta-analysis (PMID: 36821561) confirmed equivalence of endoprosthetic reconstruction vs. allograft reconstruction with respect to local recurrence, but endoprostheses had higher reoperation rates for mechanical complications
- A 2025 systematic review (PMID: 40444083) confirmed joint-preserving approaches around the knee are safe in selected osteosarcoma patients with excellent epiphyseal response to chemotherapy
13. Advances and Future Directions
- 3D printing / patient-specific implants: Custom-made pelvic and complex anatomic site prostheses with near-anatomic geometry
- Computer-assisted surgery (CAS) and intraoperative navigation: Real-time guidance for tumor margin verification
- Expandable prostheses: Non-invasive (magnetic) expansion for growing children (PHENIX, STANMORE types)
- Extracorporeal radiation therapy (ECRT): Biological reconstruction using the patient's own irradiated bone; combines economy with anatomic fit
- Targeted immunotherapy and checkpoint inhibitors: Improving chemotherapy response rates, expanding the pool of LSS candidates
- Vascularized composite allografts: Provide living bone for intercalary reconstruction in pediatric patients
Summary Diagram
MALIGNANT LIMB TUMOR
│
▼
STAGING & BIOPSY
(MRI, CT, bone scan; longitudinal biopsy, biopsy tract marked)
│
▼
NEOADJUVANT CHEMOTHERAPY
(for high-grade: osteosarcoma, Ewing sarcoma)
│
▼
ASSESS RESECTABILITY
┌─────────────────────────────┐
│ Wide margin achievable? │
│ Neurovascular bundle free? │
│ Functional limb expected? │
└─────────────────────────────┘
YES │ NO │
│ │
▼ ▼
LIMB SALVAGE AMPUTATION
SURGERY (LSS)
│
▼
EN BLOC RESECTION
(wide margin, biopsy tract excised)
│
▼
RECONSTRUCTION
┌──────────────────────────────────┐
│ Endoprosthesis (most common) │
│ Osteoarticular allograft │
│ Allograft-prosthesis composite │
│ Arthrodesis (allograft/rod) │
│ Intercalary graft (ECRT/VFG) │
│ Rotationplasty (children) │
└──────────────────────────────────┘
│
▼
SOFT-TISSUE COVERAGE
(gastrocnemius/free flap as needed)
│
▼
ADJUVANT CHEMOTHERAPY
± RADIOTHERAPY
│
▼
REHABILITATION & SURVEILLANCE
Sources:
- Campbell's Operative Orthopaedics 15th Ed 2026, Chapter 26: Tumors, pp. 1091-1217
- Miller's Review of Orthopaedics 9th Edition, Chapter 9: Musculoskeletal Tumors, pp. 827-831
- Hovav O, et al. "Limb salvage surgery reconstructive techniques following long-bone lower limb oncological resection: a systematic review and meta-analysis." ANZ J Surg. 2023 Nov [PMID: 36821561]
- Zheng K, et al. "Systematic Review of joint preservation limb salvage in osteosarcoma around the knee." Front Oncol. 2025 [PMID: 40444083]
- Osteosarcoma Limb-Salvage Treatment Guideline. PMC7454155
Local control must be at least equal to that achievable by amputation what does this mean
This is a conceptual question that I can explain clearly from the material already in our context, without needing additional tool calls.
What "Local Control Equal to Amputation" Means
Local control refers to the ability to eliminate all tumor cells at the primary site - preventing the cancer from growing back in the same limb where it started (called local recurrence).
The Core Idea
When surgeons say limb salvage must achieve "local control at least equal to amputation," they mean:
The chance of the tumor coming back in that limb after LSS must be no higher than it would be if the limb were simply amputated.
Why Amputation Was the Gold Standard for Local Control
Amputation removes the entire limb - bone, muscle, blood vessels, skin - all in one go. There is virtually no tumor-containing tissue left behind. Local recurrence is extremely unlikely because there is simply nothing left for the tumor to grow in.
So amputation set the benchmark for local control.
The Problem LSS Has to Overcome
In limb salvage, the limb stays. The surgeon cuts around the tumor, leaving the rest of the limb intact. This raises a legitimate concern:
- What if microscopic tumor cells remain at the edges of the cut?
- What if satellite tumor deposits in the reactive zone are not fully removed?
- Could the tumor grow back in the preserved tissue?
If limb salvage left residual tumor cells and caused a high local recurrence rate, it would be an oncologically inferior operation - you'd be saving the limb at the cost of the patient's life.
How This Criterion Is Satisfied in Practice
The criterion is met by achieving a wide (R0) surgical margin - meaning the tumor is removed with a cuff of completely normal, tumor-free tissue on all sides.
| Situation | Local Recurrence Rate |
|---|---|
| Distal femur osteosarcoma - Wide resection + LSS | 5-10% |
| Distal femur osteosarcoma - Transfemoral amputation | 5-10% |
| Hip disarticulation | ~1-2% (lower, but no survival advantage) |
The numbers are equivalent. This is the data that validated limb salvage as oncologically acceptable.
A Practical Example
Imagine a patient with osteosarcoma of the distal femur:
- Amputation would remove the femur, knee, tibia, and foot. Local recurrence risk: ~5%.
- Limb salvage with wide resection (3 cm bone margin beyond the tumor + cuff of soft tissue) + endoprosthesis: Local recurrence risk: ~5-10%.
Because these numbers are equivalent, the surgeon can justify saving the limb - the patient is not being put at greater oncologic risk just to keep their leg.
When This Criterion CANNOT Be Met
If the tumor involves major neurovascular structures (e.g., the popliteal artery is encased by tumor), you cannot get a wide margin without removing those structures - and removing them means the limb is non-functional or non-viable anyway. In this situation:
- A wide margin is not achievable with LSS
- Local recurrence risk would be unacceptably high
- Amputation becomes the oncologically correct choice
This is why neurovascular involvement is an absolute contraindication to limb salvage.
The Bottom Line
The criterion is essentially asking:
"Are we cutting out enough normal tissue around this tumor that we can confidently say no cancer cells are left behind - just as confidently as if we had removed the whole limb?"
If yes → proceed with limb salvage.
If no → amputation is required to protect the patient's life.
If no → amputation is required to protect the patient's life.
Saving the limb is only justified if it does not compromise the chance of curing the cancer.
This is a shared conversation. Sign in to Orris to start your own chat.