Discuss the management of laryngotracheal stenosis in detail for 50 marks with diagram and flow charts from Scott Brown, Cummings, stell and marans, Zakir Hussain, dhingra, hazarika and related articles with recent advances according to rguhs university
Reading File
Finding Sources
Finding Sources
Searching PubMed
laryngotracheal stenosis management treatment
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Finding Sources
Reading File
Reading File
Here is the complete 50-mark answer on Management of Laryngotracheal Stenosis as per RGUHS standards, compiled from Scott-Brown's, Cummings, and related textbooks in the medical library, with 2025-2026 PubMed literature for recent advances.
MANAGEMENT OF LARYNGOTRACHEAL STENOSIS
50-Mark Answer | RGUHS ENT Examination
INTRODUCTION
Laryngotracheal stenosis (LTS) is abnormal narrowing of the laryngotracheal complex causing airway obstruction. The narrowest site in the adult airway is the glottis (subglottis in infants). Airflow resistance is proportional to stenosis length but inversely proportional to the 4th power of the radius (Poiseuille's law: R = 8nl/πr⁴) - hence even mild narrowing dramatically increases resistance.
Post-intubation injury in ICU is now the most common cause (~50%), replacing infections since antibiotics and mechanical ventilation became widespread. - Scott-Brown's, Chapter 76
AETIOLOGY
| Cause | Frequency |
|---|---|
| Post-intubation (ICU ventilation) | 50.3% (34.3% subglottic + 16% tracheal) |
| Bilateral vocal cord mobility impairment | 16.67% |
| Wegener's / GPA granulomatosis | 10% |
| Idiopathic subglottic stenosis | 8.67% |
| Supraglottic stenosis | 5.7% |
| Post-tracheostomy | ~2% |
| Glottic web, papillomatosis, trauma | Remainder |
(Table 76.1, Scott-Brown's - 600 consecutive cases, National Centre for Airway Reconstruction)
Pathophysiology of post-intubation LTS: ET tube cuff pressure → ischemic mucosal necrosis → ulceration → perichondritis → cartilage resorption → healing by fibrosis and wound contracture → stenosis. Injuries occur primarily at the posterior glottis (tube tip pressure) and subglottis (cuff pressure). - Cummings, Chapter 67
CLASSIFICATION
Myer-Cotton Grading System (most widely used)
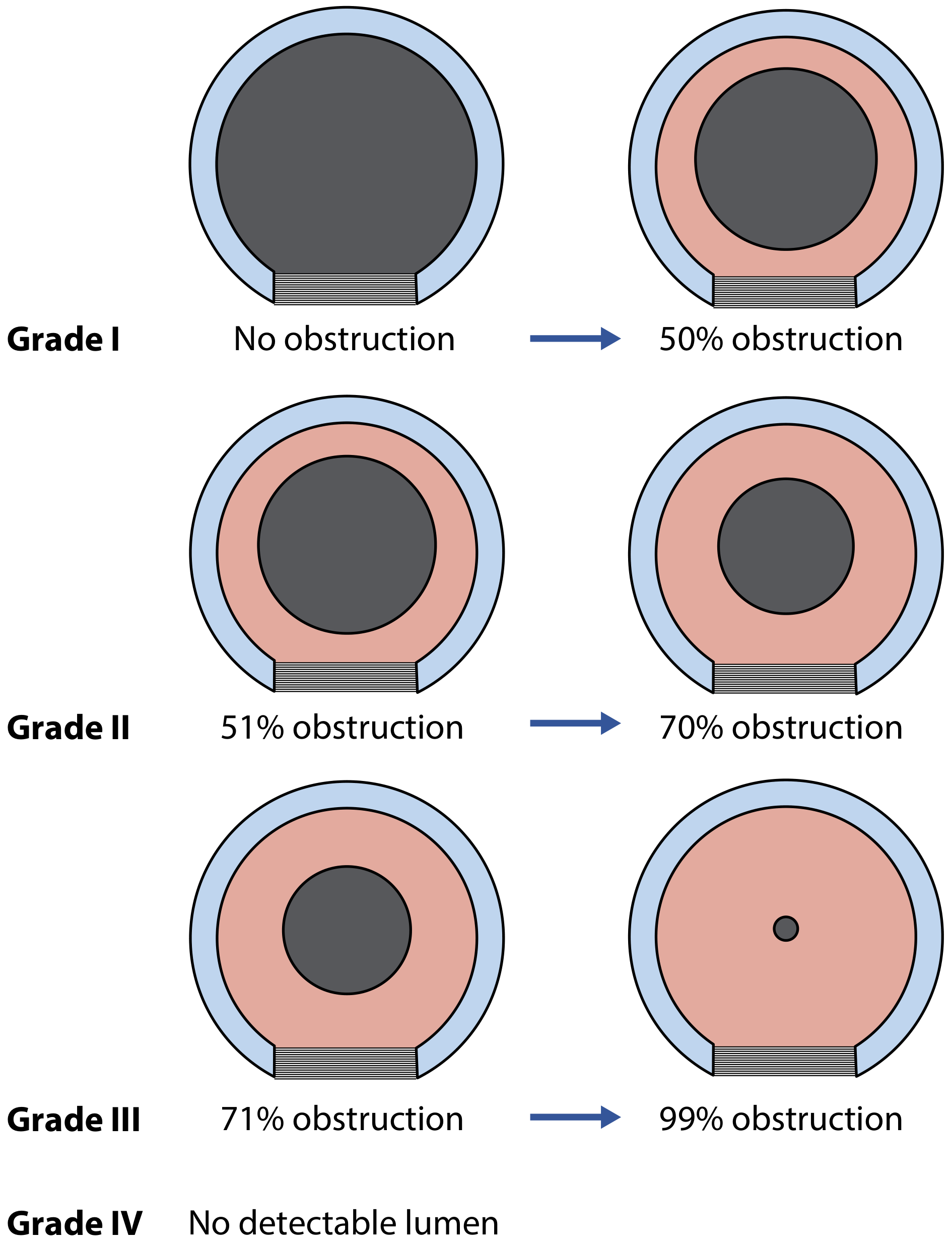
Fig. 1 - Myer-Cotton grading system for subglottic stenosis. (Scott-Brown's / Cummings)
| Grade | Obstruction | Management Implication |
|---|---|---|
| I | 0-50% | Conservative/endoscopic |
| II | 51-70% | Endoscopic or open |
| III | 71-99% | Usually open |
| IV | No lumen | CTR or tracheostomy |
Other classifications:
- McCaffrey (tracheal stenosis) - 4 stages based on length and location
- Bogdasarian (posterior glottic stenosis) - Types I-IV based on scar extent
- Cotton Staging (for LTR planning) - Stages 1-3 based on tracheostomy dependence
DIAGNOSIS
Symptoms: Exertional dyspnoea (main symptom; patients reduce activity to compensate), stridor (biphasic in fixed stenosis), dysphonia, chronic cough, dysphagia. Often misdiagnosed as asthma or COPD.
Investigations:
- Flexible fiberoptic laryngoscopy - vocal fold mobility, dynamic airway assessment
- Microlaryngoscopy and Bronchoscopy (MLB) - Gold standard; stages severity, measures dimensions
- CT neck + chest - defines anatomy, cartilage integrity, multilevel disease
- Spirometry/Flow-volume loop - Fixed stenosis: flat top both inspiration and expiration; variable extrathoracic: limits inspiration; variable intrathoracic: limits expiration
- FEES/Videofluoroscopy - mandatory if swallowing impairment suspected (poor outcomes post-reconstruction if even minor aspiration present)
- Antireflux evaluation (LPR is a risk factor)
MDT required: ENT surgeon, thoracic surgeon, pulmonologist, anaesthetist, radiologist, pathologist, speech-language therapist, dietician. - Scott-Brown's, p. 1126
MANAGEMENT FLOWCHART (Cummings, Fig. 209.7)
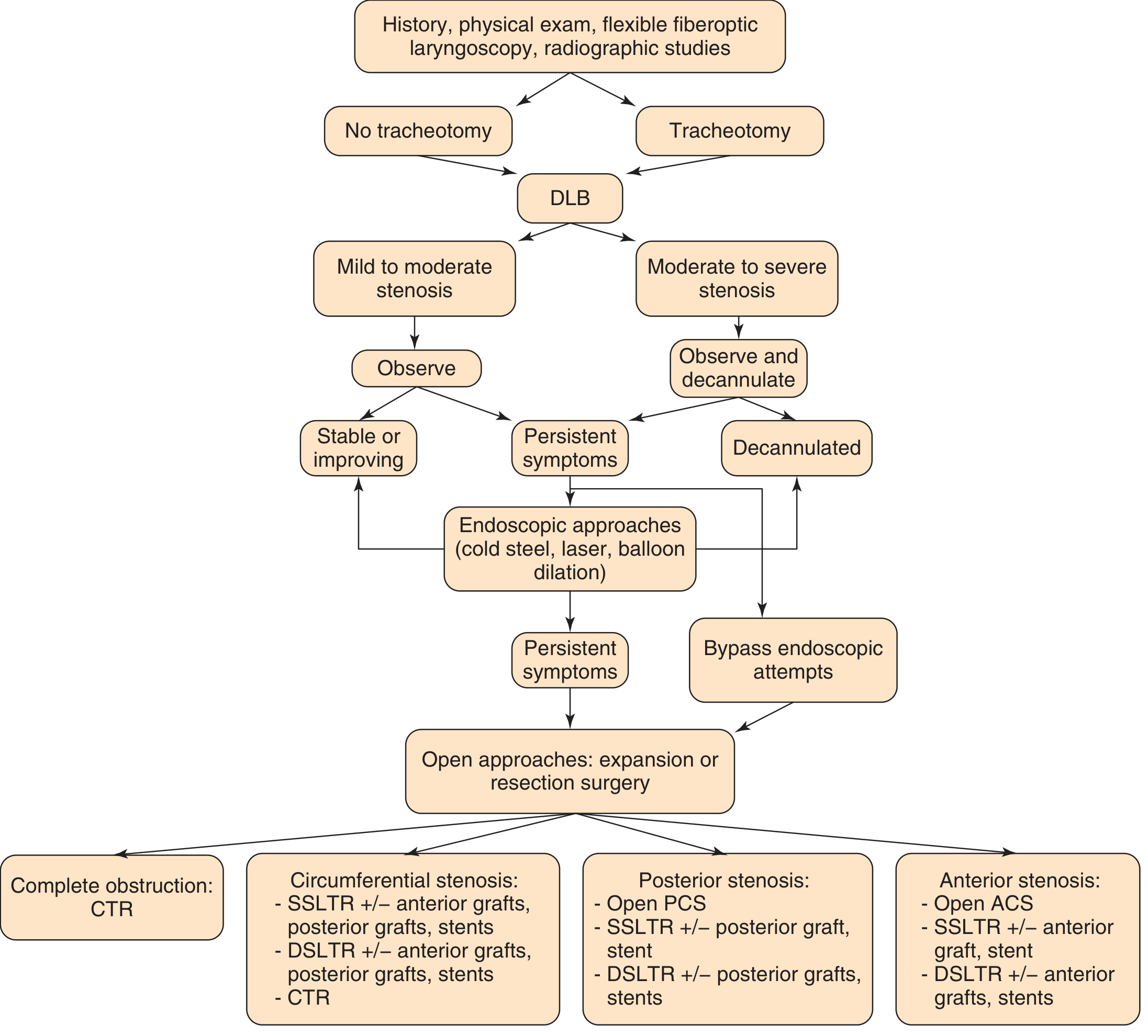
Fig. 2 - General algorithm for management of laryngeal stenosis. ACS = anterior cricoid split; CTR = cricotracheal resection; DLB = direct laryngoscopy and bronchoscopy; DSLTR = double-stage laryngotracheal reconstruction; PCS = posterior cricoid split; SSLTR = single-stage laryngotracheal reconstruction. (Cummings Otolaryngology)
DECISION-MAKING FRAMEWORK
┌──────────────────────────────────────────────────────────────┐
│ LARYNGOTRACHEAL STENOSIS │
│ History → MLB → CT → Spirometry → FEES → MDT review │
└────────────────────────┬─────────────────────────────────────┘
│
┌────────────────────┼────────────────────┐
│ │ │
SYSTEMIC DISEASE GRADE I-II GRADE III-IV
(GPA, TB, sarcoid) SOFT STENOSIS HARD FIBROTIC
│ │ │
TREAT CAUSE ENDOSCOPIC CARTILAGE
FIRST MANAGEMENT INTACT?
│ │ / \
↓ ↓ YES NO
After control: Laser + Balloon │ │
consider ± MMC ± Steroid ENDOSCOPIC OPEN SURGERY
endoscopic/open Repeat every TRIAL DIRECTLY
3-4 weeks │
│ Fails after
Success? 3 sessions?
/ \ │
Yes No OPEN SURGERY
│ │
Follow ┌─┴───────────────────┐
up │ │
ADULT PEDIATRIC
│ │
┌───────┤ ┌─────┤
│ │ │ │
CTR Tracheal SSLTR DSLTR
(preferred) Resection ± ant/post rib graft
MANAGEMENT IN DETAIL
I. CONSERVATIVE / MEDICAL MANAGEMENT
- Observation: Grade I SGS; children with mild SGS (airway grows with age)
- Treat underlying cause: GPA → cyclophosphamide + steroids/rituximab; TB → ATT; sarcoid → systemic steroids
- Antireflux therapy: PPI twice daily + alginate suspension (routine perioperative)
- Systemic steroids: Adjunct in inflammatory phase
- Racemic epinephrine nebulization: Acute mucosal edema reduction
- Inhaled corticosteroids: Early mild stenosis
II. ENDOSCOPIC MANAGEMENT
Appropriate for: Grades I-II (always), Grades III-IV (trial), soft/inflammatory lesions, patients unfit for open surgery.
A. Balloon Dilation
- Applies uniform radial pressure (unlike rigid dilators which apply shearing force)
- High-pressure airway balloons; sized to age
- Combined with radial incisions for best results
- Effective for short, thin, web-like stenoses
B. CO2 Laser Excision
- Radial cuts at 12, 3, and 9 o'clock positions
- Preserves posterior commissure to prevent re-stenosis
- Fiber-based systems (thulium CO2) for improved accuracy and access
- Useful for early granulation tissue stenosis
- NOT repeated if no improvement (worsens injury)
C. Intralesional Corticosteroid
- Triamcinolone acetonide (Depo-Medrone 40 mg/mL, up to 3 mL)
- Injected before or after dilation
- Common in practice despite controversial evidence
D. Topical Mitomycin-C (MMC)
- Alkylating agent → inhibits fibroblast proliferation and scar reformation
- Applied via pledgets (0.4 mg/mL for ~4 minutes) after dilation/scar lysis
- Best on young granulation tissue; less effective on mature scar
- Risk: fibrinous exudate causing acute airway obstruction
- Cummings, p. 1875-1878
E. Endoscopic Stents
- T-tubes (Montgomery), silicone stents as temporary/palliative
- Metal stents (SEMS) only for malignant stenosis
- Risks: mucosal ischemia, granulation, infection
Outcome: ~65% success for post-intubation LTS. Fails with: cartilage damage, length >3 cm, obesity, aspiration. Rule of 3: By the 3rd endoscopic session, decision for open surgery should be made. - Scott-Brown's, p. 1128
III. OPEN SURGICAL MANAGEMENT
A. Anterior Cricoid Split (ACS)
- Indication: Neonates/infants failing extubation
- Midline division of cricoid + upper tracheal rings anteriorly
- Patient intubated post-op; extubated after 5-7 days in ICU
- Augmented with auricular/thyroid cartilage graft if needed
- Contraindicated in ventilator-dependent patients
- Success rate: 35-88%
B. Laryngotracheal Reconstruction (LTR) - Gold standard for pediatric SGS
Cartilage grafts:
- Rib cartilage (6th/7th rib) - most common; shaped as a boat/keel graft
- Auricular conchal cartilage (smaller defects)
- Thyroid cartilage (pedicled, vascularized)
- Nasal septal cartilage
| Stage | Type | When Used |
|---|---|---|
| SSLTR | Single-stage; ETT as stent; extubate at 7-10 days | Grade II-III, no tracheostomy dependence |
| DSLTR | Double-stage; suprastomal stent; tracheostomy removed later | Grade III-IV, severe posterior stenosis, failed SSLTR |
- Anterior LTR: anterior cricoid split + anterior graft (for anterior and circumferential stenosis)
- Posterior LTR: posterior cricoid split + posterior graft (for posterior glottic stenosis)
- Combined: both grafts for severe circumferential stenosis
- Decannulation rates: 85-95%
C. Cricotracheal Resection (CTR) - Preferred in ADULTS
- Resects anterior cricoid lamina + stenotic segment
- Thyrotracheal anastomosis to residual posterior cricoid shell
- Advantages over LTR: no donor site morbidity, better voice outcomes, no glottic surgery, near-normal mucosalized airway
- Maximum resection: 4-6 cm in adults (with release procedures)
- Success rate: 90-95%
Technique highlights:
- Collar incision; cricothyroid muscle dissected and reflected (protecting RLN)
- Superior cut: inferior thyroid cartilage → below cricothyroid joints
- Inferior cut: one ring below first normal tracheal ring
- Anterior pedicled wedge of cricoid preserved for lumen enlargement
- Thyrotracheal anastomosis; suprahyoid release for tension relief
- Chin-to-chest sutures (7-10 days); stent (ETT, T-tube, or suprastomal)
- Return to OR at day 7-10 for inspection
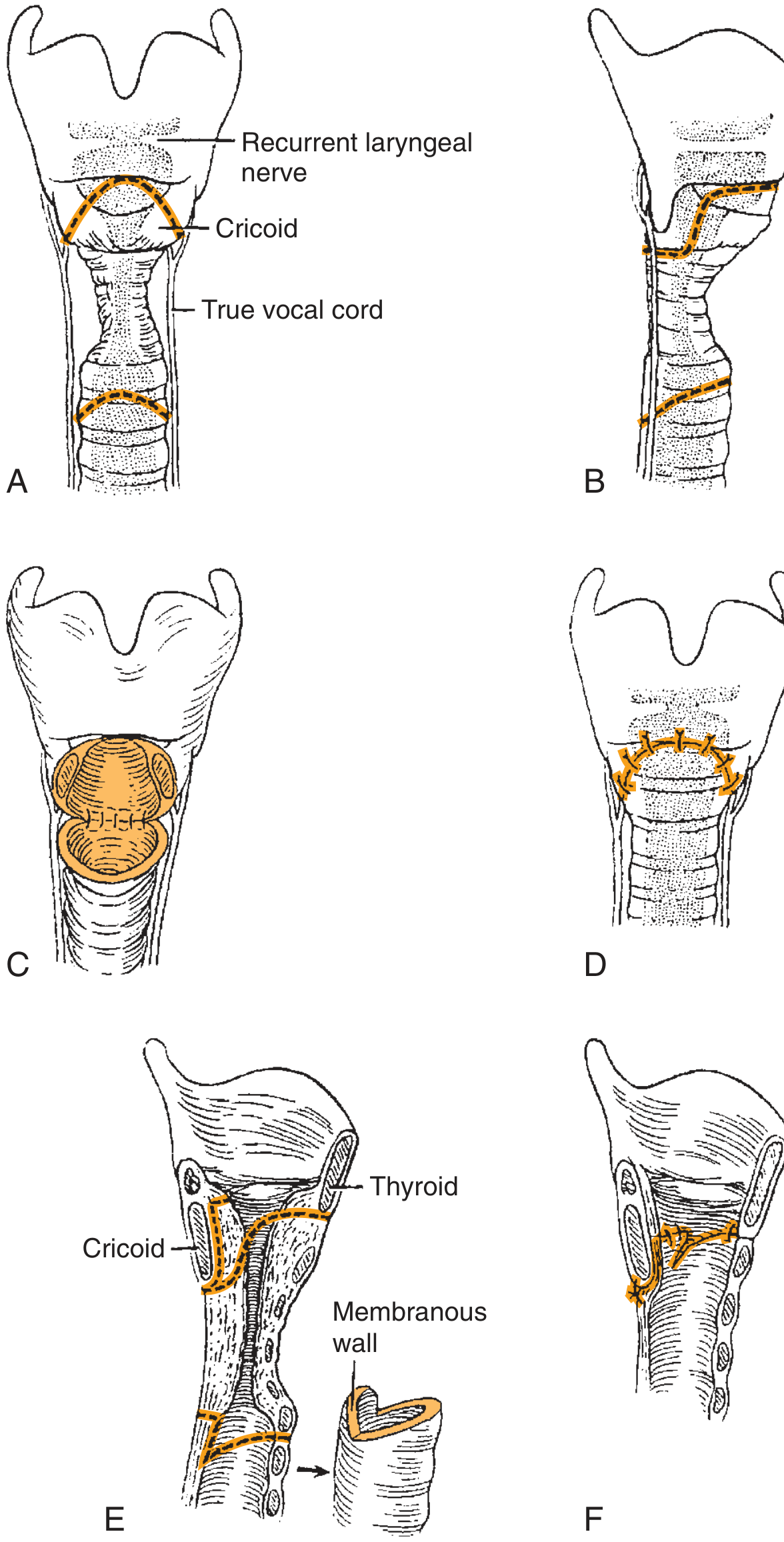
Fig. 3 - CTR: Partial cricoid resection with thyrotracheal anastomosis. Note the preservation of posterior cricoid lamina and recurrent laryngeal nerve location. (Cummings, Fig. 209.18)
D. Tracheal Resection and Primary Anastomosis
- For isolated tracheal stenosis (post-intubation, post-tracheostomy)
- Release procedures to reduce anastomotic tension:
- Suprahyoid laryngeal release
- Pulmonary hilar release
- Cervical flexion sutures (chin to chest)
E. Tracheostomy
- Permanent palliation; bridge to definitive surgery; emergency airway
IV. MANAGEMENT BY STENOSIS TYPE
| Type | Preferred Approach |
|---|---|
| Grade I-II SGS | Endoscopic (laser + balloon) |
| Grade III pediatric SGS | SSLTR ± graft |
| Grade IV pediatric SGS | DSLTR + ant/post graft |
| Adult subglottic | CTR (preferred) |
| Posterior glottic (Type I-II) | Endoscopic ± SSLTR + post graft |
| Posterior glottic (Type III-IV) | Open PCS + SSLTR/DSLTR + posterior graft |
| Tracheal stenosis only | Tracheal resection + anastomosis |
| Idiopathic SGS | Endoscopic (serial); CTR for long-term cure |
| GPA/Wegener's | Immunosuppression first; endoscopic for stenosis |
RECENT ADVANCES (2021-2026)
- Endoscopic management expansion to severe (Grade III) stenosis with lower morbidity - [Pinzas et al., Thorac Surg Clin 2025, PMID: 39515893]
- Fiber-based lasers (thulium, CO2 fiber): improved precision and access to difficult anatomical sites
- Bioresorbable stents (PGLA-based): experimental; avoids repeat endoscopy for stent removal
- Tracheal allotransplantation with immunosuppression: for long-segment disease
- Tissue engineering/bioengineered trachea: decellularized scaffolds seeded with autologous stem cells (clinical trials ongoing)
- Idiopathic SGS - hormonal research: estrogen/progesterone roles being studied; GLP-1 agonists as anti-fibrotics
- TORS (Transoral Robotic Surgery): for posterior glottic and supraglottic lesions
- 3D virtual bronchoscopy + dynamic CT: for preoperative planning and surveillance
- Comprehensive imaging protocols for functional airway assessment - [Romero-Sanchez et al., Radiographics 2025, PMID: 40638414]
- Single-stage CTR in pediatrics: extending adult CTR success to children with favorable anatomy - [Smith & Buck, Expert Rev Respir Med 2022, PMID: 36347385]
- Updated classification systems: incorporating CT, endoscopic, and functional parameters - [Zhao et al., MedComm 2025, PMID: 39866837]
COMPLICATIONS
| Complication | Notes |
|---|---|
| Restenosis | Most common; managed by repeat procedures |
| Anastomotic dehiscence | Life-threatening in CTR/tracheal resection |
| RLN injury | Dysphonia/aspiration risk |
| Dysphagia | After CTR or tracheal resection |
| Granulation tissue | Around stents; requires endoscopic removal |
| Decannulation failure | After LTR in complex cases |
| Aspiration pneumonia | Prior aspiration = poor reconstruction outcome |
KEY PEARLS FOR RGUHS EXAM
- The best chance for successful repair lies in the initial operation - so correct case selection is paramount
- Resistance is proportional to 1/r⁴ - doubling radius reduces resistance 16-fold
- Endoscopy fails if: cartilage damage, length >3 cm, obesity, aspiration - proceed to open surgery
- CTR preferred over LTR in adults (no donor site morbidity, better voice outcomes, higher success)
- Maximum tracheal/laryngeal resection in adults: 4-6 cm with release procedures
- Rule of 3 endoscopies: convert to open if no improvement by 3rd procedure
- MMC: best on young scars, not effective on mature fibrosis
- Idiopathic SGS = middle-aged women, high recurrence after endoscopy → CTR is curative
- FEES/swallow assessment is mandatory before any reconstruction (aspiration = poor outcome)
- Systemic disease (GPA, TB) must be treated before surgical reconstruction
References:
- Scott-Brown's Otorhinolaryngology HNS (8th ed.) Chapter 76
- Cummings Otolaryngology HNS (7th ed.) Chapters 67 and 209
- KJ Lee's Essential Otolaryngology
- Dhingra's Diseases of Ear, Nose & Throat
- Hazarika's ENT and HNS (Clinical methods and operative)
- Stell & Maran's Operative Head & Neck Surgery
- Zakir Hussain's Operative ENT
This is a shared conversation. Sign in to Orris to start your own chat.