How to manage if pneumothorax is on mediastinum side?
Reading File
Finding Sources
Finding Sources
Searching PubMed
tension pneumothorax management treatment
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading Article
PMID: 40383767
I now have comprehensive information. Here is the full answer:
Tension Pneumothorax with Mediastinal Shift - Management
When a pneumothorax causes mediastinal shift (structures pushed toward the opposite side), it is by definition a tension pneumothorax - a life-threatening emergency requiring immediate action.
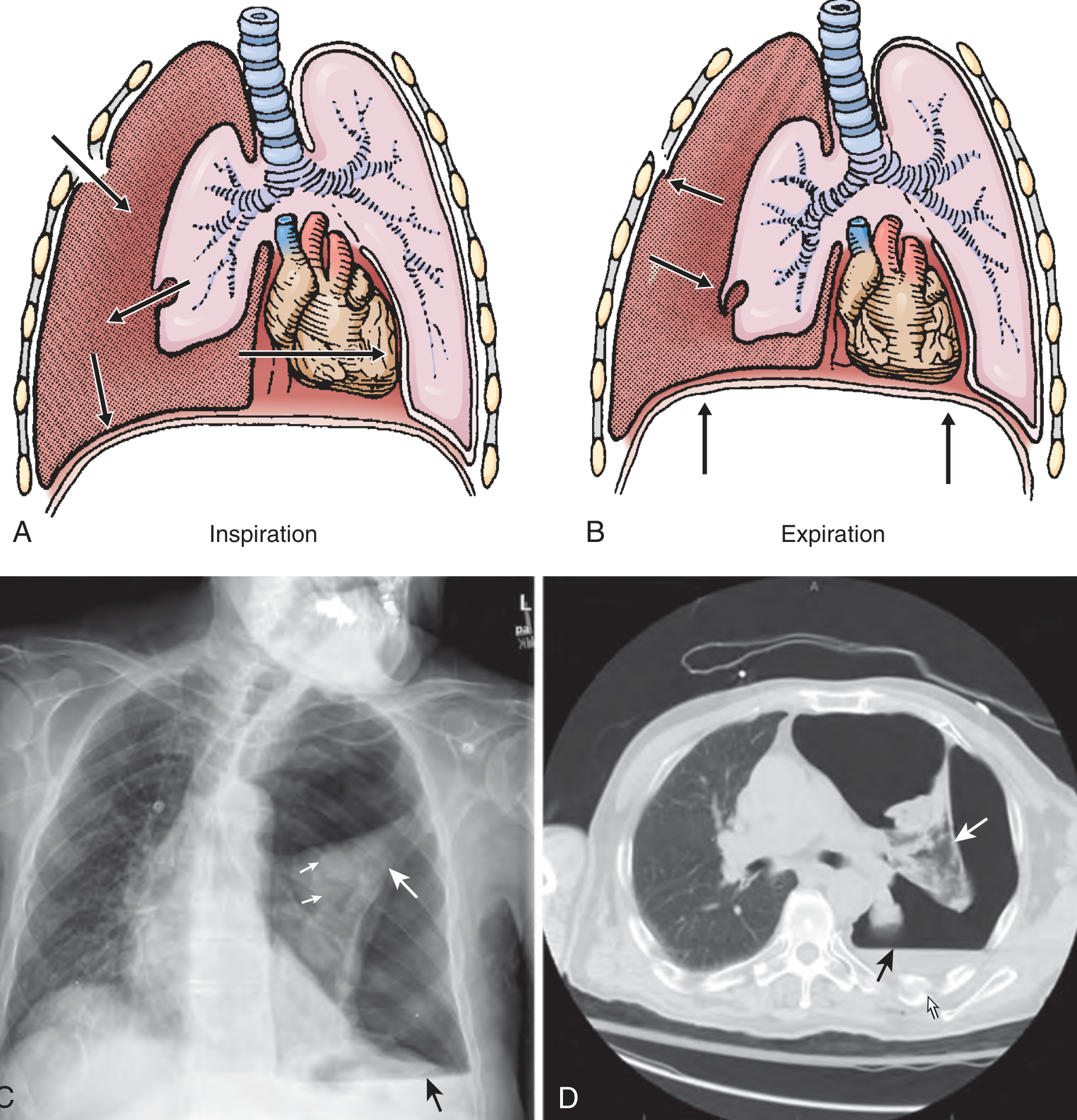
A & B: Mechanism - air enters through one-way valve during inspiration but cannot escape. C: CXR showing total left lung collapse with mediastinal shift to right. D: CT confirming findings.
Pathophysiology
Air accumulates under positive pressure via a one-way valve mechanism (from lung, airway, or chest wall). It:
- Collapses the ipsilateral lung completely
- Pushes the mediastinum toward the opposite side
- Compresses the SVC/IVC, reducing venous return and cardiac preload
- Compresses the contralateral lung, worsening hypoxia
The result is combined respiratory and circulatory failure that is rapidly fatal if untreated.
- Roberts and Hedges' Clinical Procedures in Emergency, p. 264
- Current Surgical Therapy 14e, p. 1310
Clinical Recognition (Diagnose Clinically - Do NOT Wait for CXR)
| Finding | Detail |
|---|---|
| Air hunger / tachypnea | Often the earliest sign |
| Hypoxia | Due to lung collapse |
| Absent breath sounds | On the affected side |
| Hyperresonance | On the affected side |
| Tracheal deviation | Away from the affected side |
| Distended neck veins | May be absent if hypovolemic |
| Hypotension + tachycardia | Due to reduced cardiac output |
| Increased ventilator resistance | In intubated patients - earliest sign |
Differentiate from cardiac tamponade: Both cause JVD, hypotension, and restlessness - but tamponade causes muffled heart sounds with no tracheal deviation and symmetric breath sounds.
- Current Surgical Therapy 14e
- Bailey and Love's Short Practice of Surgery 28th Ed
Management - Step by Step
STEP 1: Immediate Needle Decompression (Emergency)
Do not delay for imaging. This converts tension pneumothorax to a simple pneumothorax.
Sites (choose one):
- 2nd intercostal space, midclavicular line (2nd ICS MCL) - traditional ATLS approach; insert needle just above the 3rd rib to avoid the neurovascular bundle
- 4th-5th intercostal space, anterior axillary line - recommended by Rosen's; preferred in obese patients and may be more reliable
Technique:
- Large-bore needle/angiocatheter (14-gauge), at least 5 cm long (ideally 7 cm)
- A rush of air confirms correct placement
- Immediate improvement in vital signs expected
A 2025 meta-analysis (n = 8,046) found a 32.84% failure rate when the needle did not penetrate the pleural cavity - longer needles (7 cm) significantly reduce failure. For left-sided tension pneumothorax, the 2nd MCL is safer to avoid cardiac injury; for right-sided cases, either the 2nd MCL or 5th midaxillary line is acceptable. - Ahmad et al., World J Emerg Surg, 2025 (PMID 40383767)
STEP 2: Chest Tube (Tube Thoracostomy) - Definitive Treatment
-
Perform immediately after (or instead of, in the ED setting) needle decompression
-
In the ED, it may be just as fast to insert a chest tube directly
-
Alternatively, finger thoracostomy (without inserting the tube yet) can provide immediate relief
-
The chest tube drains residual air and any associated blood (hemopneumothorax)
-
Re-expansion of the lung usually seals the lung defect
-
Rosen's Emergency Medicine
STEP 3: Supportive Measures
- High-flow supplemental oxygen (100% O2 speeds nitrogen absorption)
- IV access, fluid resuscitation for hemodynamic instability
- Continuous monitoring (SpO2, BP, HR, ECG)
- If on positive pressure ventilation (PPV): temporarily disconnect from ventilator during decompression - PPV actively drives more air in and worsens tension
STEP 4: Post-Stabilization
- Confirm chest tube position with CXR
- Ensure lung re-expansion; if not re-expanded consider bronchial plug, contralateral tension, or malpositioned tube
- Treat underlying cause (e.g., close open chest wound with occlusive dressing - three-sided, to allow air escape)
Special Situations
| Situation | Action |
|---|---|
| Open (sucking) chest wound | Apply 3-sided occlusive dressing first; place chest tube; do NOT fully seal without a tube (risks converting to tension) |
| Ventilated patient | Disconnect from ventilator briefly during decompression; has highest risk of developing tension PTX |
| Penetrating chest trauma | Consider prophylactic chest tube before starting mechanical ventilation even if no PTX evident on imaging |
| Bilateral pneumothorax | Mediastinal shift may be absent - do not rely on it; decompress both sides |
| Asthma/emphysema on PPV | High-pressure ventilation is a common cause; have low threshold to decompress |
- Roberts and Hedges', Bailey and Love's, Rosen's EM
Key Principle
"Tension pneumothorax is diagnosed clinically, constituting a life-threatening emergency. Chest x-rays are not necessary to confirm the diagnosis, and delays to definitive treatment significantly increase the risk of circulatory collapse and cardiorespiratory arrest." - Current Surgical Therapy 14e
The sequence is: Recognize clinically → Needle decompress immediately → Follow with chest tube → Supportive care → Identify and treat the underlying cause.
This is a shared conversation. Sign in to Orris to start your own chat.