Basal ganglia
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have comprehensive material. Let me compile the full answer.
Basal Ganglia
Anatomy and Components
The basal ganglia are a collection of gray matter nuclei located deep within the white matter of the cerebral hemispheres. The main components are:
| Structure | Subdivision | Notes |
|---|---|---|
| Striatum | Caudate nucleus + Putamen | Receives virtually ALL inputs to the BG; "neostriatum"; cellular bridges give striated appearance |
| Globus pallidus | Internal (GPi) + External (GPe) | Primary output nucleus |
| Subthalamic nucleus (STN) | - | Diencephalon; only excitatory output nucleus within BG |
| Substantia nigra | Pars compacta (SNc) + Pars reticulata (SNr) | SNc = dopaminergic; SNr = inhibitory output |
Associated structures include the nucleus accumbens and ventral pallidum (limbic/reward circuits), and the ventral anterior/ventral lateral thalamus (relay back to cortex). The internal capsule passes through the space between the caudate and putamen, carrying corticospinal fibers.
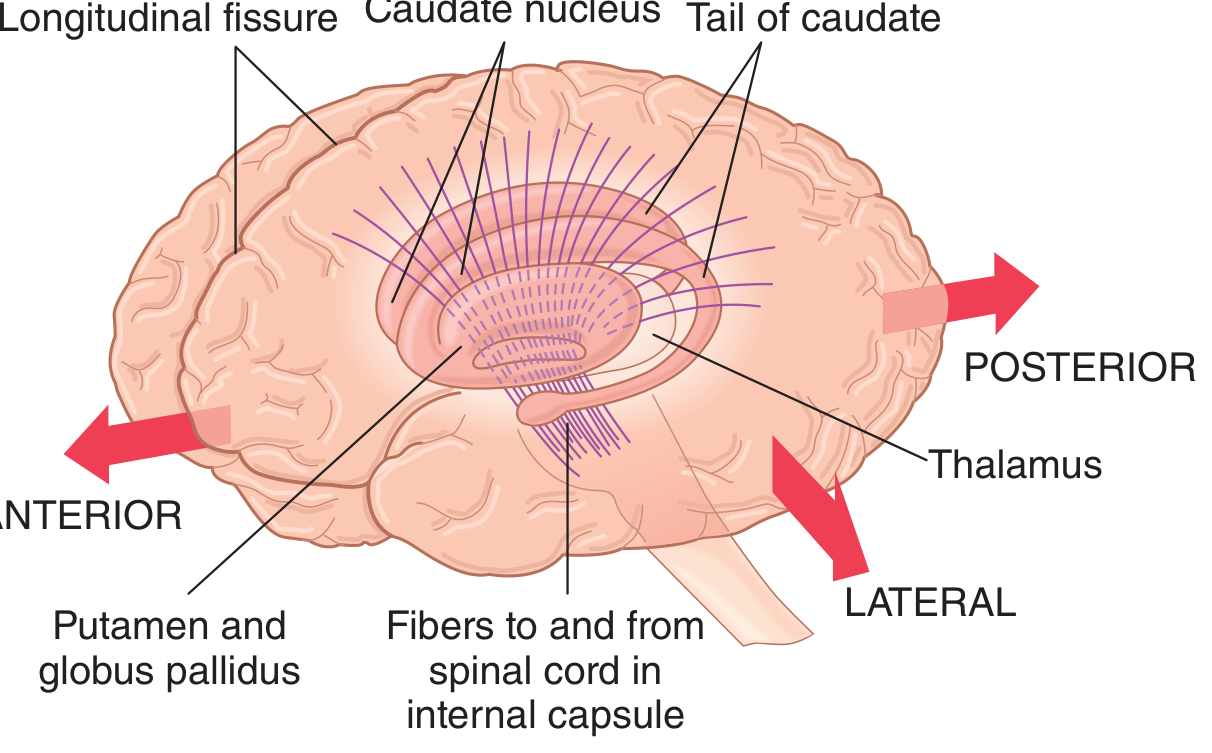
Fig. 57.9 - Anatomical relations of the basal ganglia to the cerebral cortex and thalamus (Guyton & Hall)
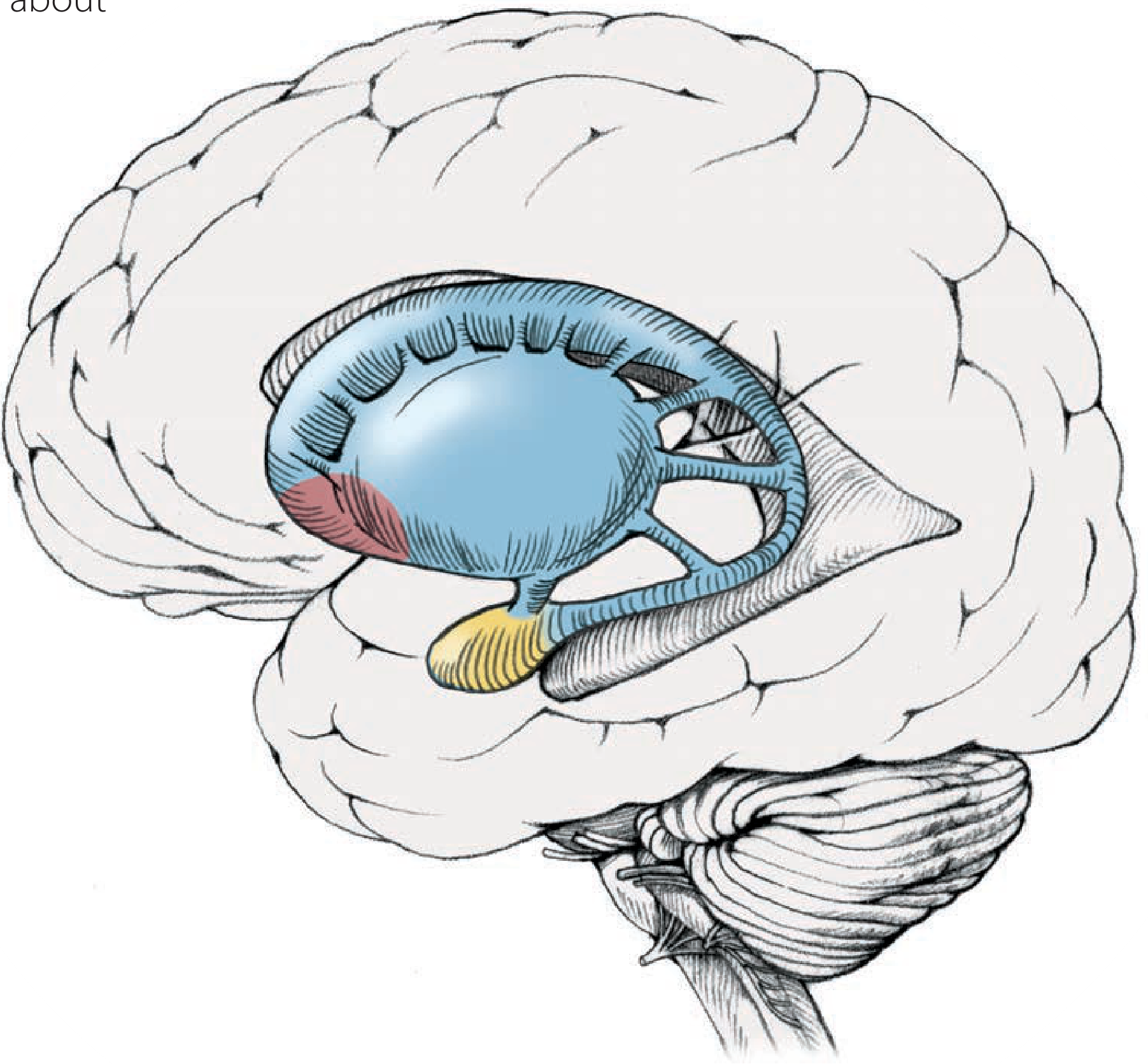
Basal ganglia in situ - striatum (blue), globus pallidus (red), subthalamic nucleus (yellow) (Neuroanatomy through Clinical Cases)
Inputs and Outputs
- Inputs (afferents): Almost all areas of the cerebral cortex project topographically onto the striatum, with a critical input from the motor cortex. The substantia nigra pars compacta sends a major dopaminergic input back to the striatum.
- Outputs (efferents): The striatum projects to the globus pallidus and substantia nigra. The GPi and SNr project (inhibitory) to the thalamus, which then projects excitatory signals back to the motor cortex. The BG do NOT project directly to the spinal cord or brainstem motor neurons.
Neuronal Circuitry: Direct vs. Indirect Pathways
The basal ganglia modulate thalamo-cortical output via two opposing pathways. Their net balance controls the level of motor activity.
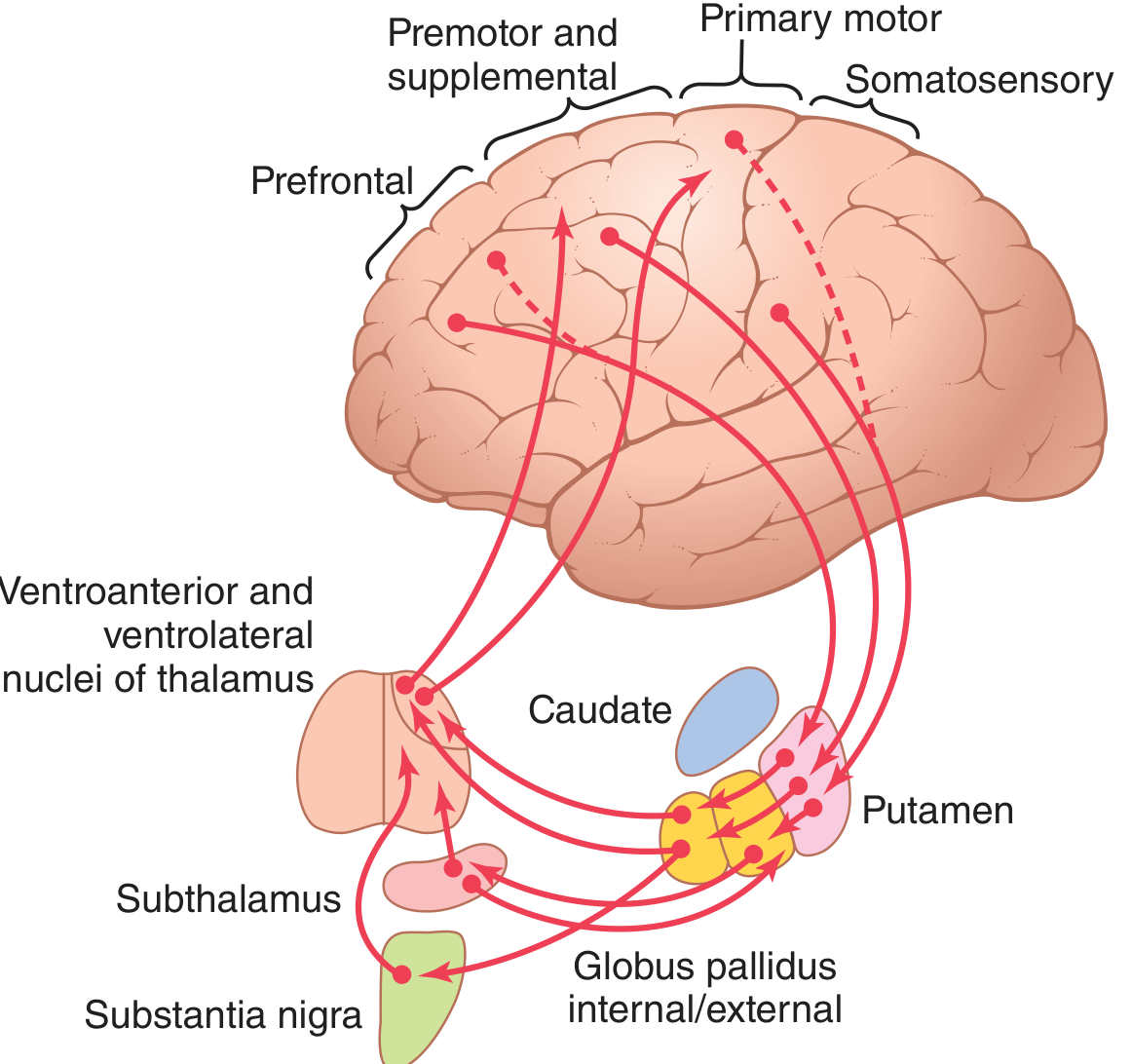
Fig. 57.11 - Putamen circuit through the basal ganglia for subconscious execution of learned motor patterns (Guyton & Hall)
Direct Pathway (facilitatory - net excitatory effect on cortex)
Cortex → Striatum → GPi/SNr → Thalamus → Cortex
- Cortex excites the striatum (glutamate)
- Striatum inhibits GPi/SNr (GABA)
- GPi/SNr inhibition is reduced, so thalamus is released from inhibition
- Thalamus excites the cortex (glutamate)
- Net effect: increased motor activity
Indirect Pathway (inhibitory - net inhibitory effect on cortex)
Cortex → Striatum → GPe → STN → GPi/SNr → Thalamus → Cortex
- Cortex excites the striatum
- Striatum inhibits GPe (GABA)
- GPe inhibition is reduced, releasing the STN from inhibition
- STN excites GPi/SNr (glutamate)
- GPi/SNr strongly inhibits the thalamus (GABA)
- Thalamic excitation of cortex is suppressed
- Net effect: decreased motor activity
The direct pathway is excitatory and the indirect pathway is inhibitory. They are carefully balanced - a disturbance in one causes either an increase or decrease in motor activity, which is the basis of basal ganglia diseases. - Costanzo Physiology 7th Edition
Dopamine's Role (Nigrostriatal Pathway)
The substantia nigra pars compacta (SNc) sends dopaminergic projections to the striatum. Dopamine has opposing effects in the two pathways:
- D1 receptors (direct pathway): Dopamine is excitatory - activates the direct pathway → more movement
- D2 receptors (indirect pathway): Dopamine is inhibitory - suppresses the indirect pathway → less inhibition of movement
So dopamine, overall, facilitates movement by simultaneously enhancing the direct (go) pathway and suppressing the indirect (no-go) pathway.
Two Major Functional Circuits
1. Putamen Circuit - Execution of Learned Motor Patterns
- Inputs: premotor cortex, supplementary motor area, somatosensory cortex
- Path: Cortex → Putamen → GPi → Thalamus (VA/VL) → Primary motor cortex
- Function: Controls complex, subconscious motor patterns (writing, throwing, vocalization, eye movements)
- Damage: athetosis (globus pallidus lesion), hemiballismus (subthalamic lesion), chorea (putamen lesions)
2. Caudate Circuit - Cognitive Control of Motor Sequences
- Inputs: association cortex (frontal, parietal, occipital, temporal lobes)
- Path: Cortex → Caudate → GPi → Thalamus (VA/VL) → Prefrontal/premotor/supplementary cortex
- Function: Plans and sequences motor acts based on thought (cognitive motor planning); signals return to accessory motor areas for building sequential patterns lasting 5+ seconds
- Does NOT feed directly back to primary motor cortex - feeds the planning areas
Other Functions
Beyond motor control, the basal ganglia contribute to:
- Memory and habit learning - initiation, execution, and termination of learned motor tasks
- Cognitive functions - attention, working memory, decision-making (frontal-striatal circuits)
- Affective/emotional control - limbic circuits via nucleus accumbens (reward, motivation)
- Eye movement control - via the superior colliculus
- Timing and scaling - determining speed and amplitude of movements
Diseases of the Basal Ganglia
| Disease | Pathology | Movement Type | Mechanism |
|---|---|---|---|
| Parkinson's disease | Degeneration of SNc dopamine neurons | Hypokinetic: rigidity, akinesia, resting tremor | Loss of dopamine → indirect pathway overactive + direct pathway underactive → excess inhibition of thalamus |
| Huntington's disease | Destruction of striatal GABAergic and cholinergic neurons | Hyperkinetic: choreoathetosis, dementia | Loss of indirect pathway inhibition → thalamus overactive → excess cortical excitation |
| Hemiballismus | Subthalamic nucleus lesion | Wild flailing movements of one limb | STN lesion → GPi not driven → thalamus released from inhibition |
| Athetosis | Globus pallidus lesion | Continuous writhing movements (hand/arm/face) | Loss of basal ganglia output regulation |
| Chorea | Multiple putamen lesions | Flicking movements (hands, face) | Disrupted striatal output |
Treatment of Parkinson's: L-dopa (dopamine precursor), dopamine agonists (bromocriptine), or deep brain stimulation of the STN or GPi to reduce excess inhibitory output.
Summary of Neurotransmitters
| Pathway | Neurotransmitter | Effect |
|---|---|---|
| Cortex → Striatum | Glutamate | Excitatory |
| Striatum → GPe (indirect) | GABA | Inhibitory |
| Striatum → GPi/SNr (direct) | GABA | Inhibitory |
| GPe → STN | GABA | Inhibitory |
| STN → GPi/SNr | Glutamate | Excitatory |
| GPi/SNr → Thalamus | GABA | Inhibitory |
| Thalamus → Cortex | Glutamate | Excitatory |
| SNc → Striatum | Dopamine | D1 (excitatory)/D2 (inhibitory) |
Sources:
- Guyton and Hall Textbook of Medical Physiology, Ch. 57
- Costanzo Physiology 7th Edition, Ch. 3
- Neuroanatomy through Clinical Cases 3rd Edition, Ch. 16
- Bradley and Daroff's Neurology in Clinical Practice
This is a shared conversation. Sign in to Orris to start your own chat.