Thyroid
Asking for Preferences
Reading File
Finding Sources
Searching PubMed
"thyroid disorders" AND "hypothyroidism OR hyperthyroidism"
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Here is a comprehensive overview of thyroid disorders, drawn from Robbins & Kumar Basic Pathology, Goldman-Cecil Medicine, and Harrison's Principles of Internal Medicine.
Thyroid Disorders
Physiology & Regulatory Axis
The thyroid gland weighs 10–20 g and consists of two lobes connected by an isthmus. It is composed of follicular cells (which produce T4 and T3) and parafollicular C-cells (which produce calcitonin). Follicular cells organize into units surrounding a colloid center containing thyroglobulin.
HPT Axis (negative feedback):
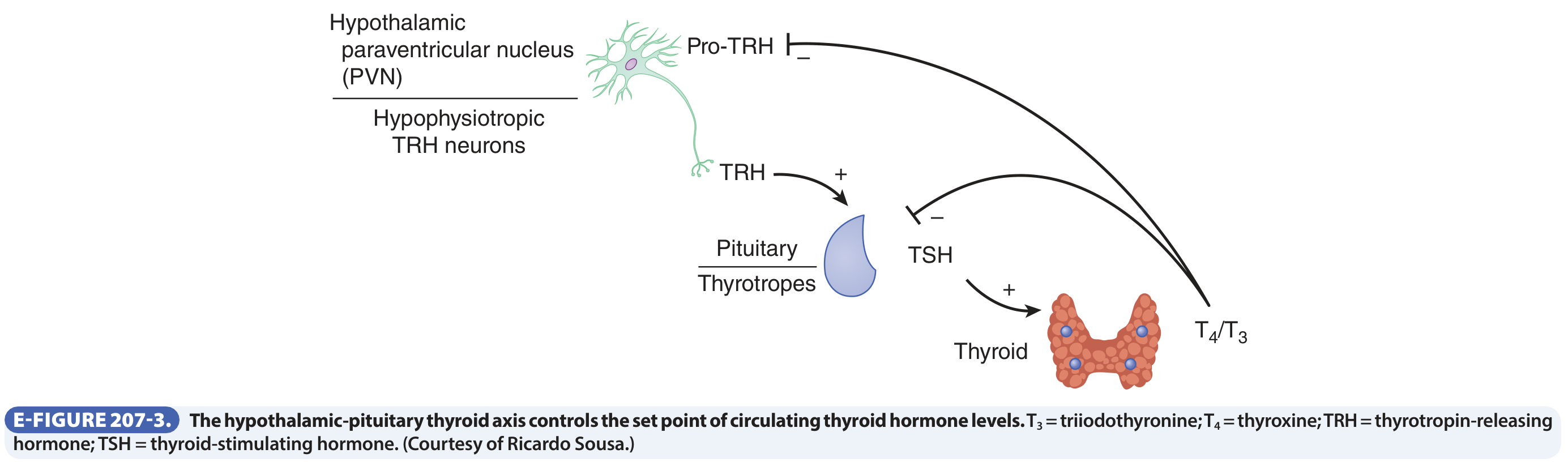
- Hypothalamic TRH → pituitary TSH → thyroid T4/T3 synthesis
- T3 and T4 feed back to suppress both TRH and TSH
- T3 is the biologically active form (10× greater receptor affinity); most circulating T4 is converted to T3 in peripheral tissues
- Iodine (~150 µg/day dietary intake) is essential; it is actively transported into follicular cells by the sodium-iodide symporter (NIS)
Classification of Thyroid Disorders
| Category | Condition | Direction of T4/T3 | TSH |
|---|---|---|---|
| Hyperthyroidism | Graves disease, toxic MNG, toxic adenoma | ↑ | ↓ |
| Hypothyroidism | Hashimoto thyroiditis, iodine deficiency, iatrogenic | ↓ | ↑ (primary) |
| Thyroiditis | De Quervain, postpartum, Hashimoto | Variable | Variable |
| Goiter | Iodine deficiency, MNG | Variable | Variable |
1. Hyperthyroidism (Thyrotoxicosis)
Causes (in order of frequency):
- Graves disease — ~85% of cases; autoimmune TSH receptor-stimulating antibodies (TRAb)
- Toxic multinodular goiter
- Toxic (hyperfunctioning) adenoma
- Transient: thyroiditis, iodine-induced (Jod-Basedow)
Clinical Features:
| System | Manifestations |
|---|---|
| Constitutional | Heat intolerance, weight loss despite ↑ appetite, sweating, warm/flushed skin |
| Cardiovascular | Palpitations, tachycardia, high-output heart failure (elderly) |
| GI | Hypermotility, diarrhea, malabsorption |
| Neuromuscular | Anxiety, tremor, irritability; proximal myopathy (~50%) |
| Ocular | Lid lag, wide staring gaze; exophthalmos (Graves-specific) |
Special situations:
- Thyroid storm — abrupt severe thyrotoxicosis (often precipitated by infection, surgery, or stopping anti-thyroid drugs); life-threatening cardiac arrhythmias
- Apathetic hyperthyroidism — blunted presentation in elderly; discovered on workup for unexplained weight loss or new cardiovascular disease
Diagnosis:
- ↓ TSH is the single most sensitive screening test (suppressed even in subclinical disease)
- ↑ Free T4; occasionally T3 toxicosis with normal/low T4
- Radioactive iodine uptake (RAIU): diffusely ↑ in Graves, focally ↑ in toxic adenoma, ↓ in thyroiditis
Treatment:
- Thioamides (methimazole, propylthiouracil) — first-line medical therapy
- Radioactive iodine-131 (¹³¹I) — definitive treatment; contraindicated in pregnancy
- Beta-blockers — symptomatic relief (palpitations, tremor)
- Surgery — thyroidectomy for large goiters or when other treatments fail
- Thyroid eye disease (Graves): teprotumumab (IGF-1R antagonist) is an approved biologic therapy
2. Hypothyroidism
Causes (Primary):
| Cause | Mechanism |
|---|---|
| Hashimoto thyroiditis | Autoimmune destruction |
| Iodine deficiency | Most common cause worldwide (affects ~2 billion) |
| Iatrogenic (surgery, radiation, ¹³¹I) | Loss of thyroid tissue |
| Drugs (lithium, amiodarone) | Interfere with synthesis |
| Congenital (thyroid dysgenesis) | 1 in 3500 births |
| Immune checkpoint inhibitors | Drug-induced autoimmunity |
Secondary (Central): TSH deficiency from pituitary/hypothalamic failure — rare, accounts for ~1% of cases.
Epidemiology: ~5% prevalence in the US/Europe; predominantly subclinical; higher in women; risk increases with age.
Clinical Features:
| System | Manifestations |
|---|---|
| Constitutional | Cold intolerance, weight gain, fatigue, dry skin |
| Cardiovascular | Bradycardia, pericardial effusion |
| GI | Constipation |
| Neuromuscular | Lethargy, impaired concentration, delayed DTRs |
| Myxedema | Severe longstanding hypothyroidism → non-pitting edema, altered consciousness (myxedema coma) |
Subclinical hypothyroidism: Normal T4/T3, TSH 4.5–20 mIU/L; treatment decision depends on TSH level, symptoms, age, and antibody status.
Diagnosis: ↑ TSH (overt: usually >20 mIU/L), ↓ free T4; positive anti-TPO and anti-thyroglobulin antibodies in Hashimoto.
Treatment: Levothyroxine (T4) — oral replacement; titrate to normalize TSH.
3. Hashimoto Thyroiditis (Chronic Lymphocytic Thyroiditis)
The most common cause of hypothyroidism in iodine-sufficient regions. Female:male ratio = 10–20:1; peak onset 45–65 years.
Pathogenesis — two key mechanisms:
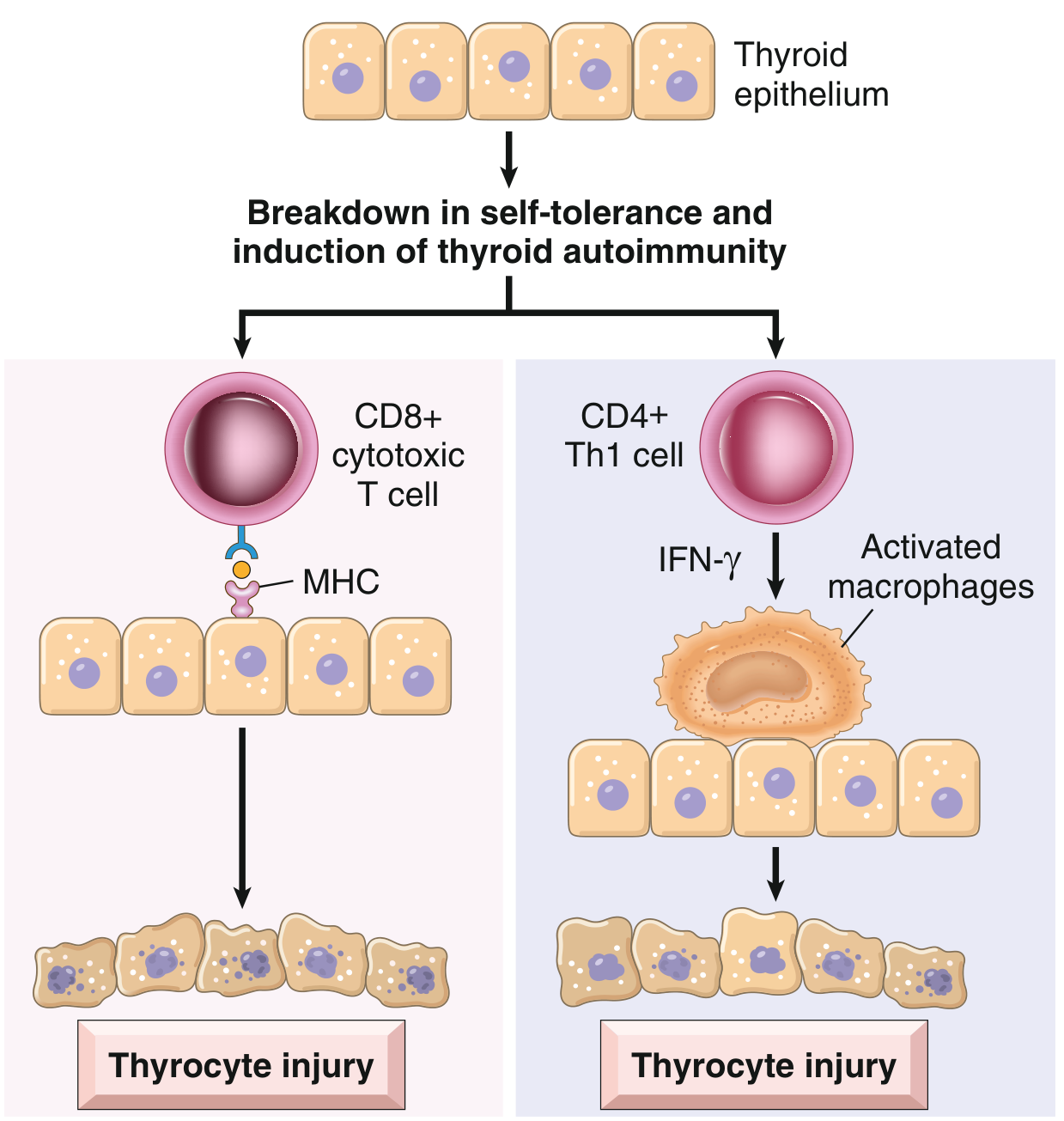
- CD8+ cytotoxic T cells directly kill thyroid epithelial cells via MHC-I recognition
- CD4+ Th1 cells produce IFN-γ → macrophage activation → follicular destruction
Genetic associations: CTLA4 polymorphisms; ~40% concordance in monozygotic twins.
Morphology: Diffuse lymphocytic infiltration with germinal centers; atrophic follicles lined by eosinophilic Hürthle (oxyphil) cells; progressive fibrosis.
Clinical course:
- Painless goiter + gradual hypothyroidism (often middle-aged woman)
- Transient thyrotoxicosis ("hashitoxicosis") can precede hypothyroidism due to follicle rupture and hormone release
- Elevated risk of primary thyroid lymphoma (B-cell)
4. Thyroiditis — Summary
| Type | Cause | Pain | RAIU | Clinical Course |
|---|---|---|---|---|
| Hashimoto | Autoimmune | No | ↓ | Progressive hypothyroidism |
| De Quervain (Subacute granulomatous) | Post-viral | Yes | ↓ | Triphasic: hyper → hypo → euthyroid |
| Postpartum/Painless | Autoimmune | No | ↓ | Biphasic; 10% of pregnancies |
| Riedel | Fibroinflammatory | No | ↓ | Hard "woody" goiter; rare |
Postpartum thyroiditis: Occurs within 12 months post-delivery; T3:T4 ratio <20 (reflecting stored hormone release, not new synthesis) — distinguishes it from Graves disease. TPO antibodies positive; TRAb negative.
5. Goiter
Thyroid enlargement from any cause. Can be:
- Diffuse (Graves, Hashimoto, iodine deficiency)
- Multinodular (MNG) — commonest thyroid disorder globally; TSH levels variable; requires evaluation for hot vs cold nodules
Iodine deficiency → ↓ T4/T3 → ↑ TSH → thyroid hyperplasia → goiter. Addressed worldwide by iodized salt.
Investigations at a Glance
| Test | Use |
|---|---|
| Serum TSH | Best initial screening test for any thyroid disorder |
| Free T4 | Confirms overt hypo/hyperthyroidism |
| T3 | Useful in T3 toxicosis (where T4 may be normal/low) |
| Anti-TPO, anti-TG antibodies | Hashimoto; postpartum thyroiditis |
| TSH receptor antibody (TRAb) | Graves disease (stimulating); replaces RAIU scanning in most cases |
| Radioactive iodine uptake (RAIU) | Differentiates causes of thyrotoxicosis; evaluates nodules |
| Ultrasound | Best anatomic imaging; guides FNA for nodule risk stratification |
| FNA biopsy | Evaluates thyroid nodules with suspicious features |
⚠️ Biotin interference: Patients taking >100 mg/day biotin can have spuriously low TSH and high T4/T3 on some assays — results normalize after stopping biotin for 2–3 days.
Key Drug Effects on Thyroid
| Drug | Effect |
|---|---|
| Amiodarone (40% iodine) | Hypo- or hyperthyroidism |
| Lithium | Hypothyroidism (blocks T4/T3 release) |
| Immune checkpoint inhibitors | Autoimmune thyroiditis → hypothyroidism |
| Tyrosine kinase inhibitors | Hypothyroidism |
| Interferon-α | Autoimmune thyroid disease |
Sources: Robbins & Kumar Basic Pathology, p. 729–733; Goldman-Cecil Medicine, Ch. 207; Harrison's Principles of Internal Medicine 22E, Ch. 207
This is a shared conversation. Sign in to Orris to start your own chat.