rotator cuff injuries orthopedics
Reading File
Finding Sources
Searching PubMed
"rotator cuff"[MeSH Terms] AND "tears"[MeSH Terms]
Reading File
Reading File
Reading File
Searching PubMed
"rotator cuff" AND repair
Reading File
Reading File
Loading Image
Reading File
Excellent. I now have comprehensive content from multiple authoritative sources. Let me compile the full answer.
Rotator Cuff Injuries - Orthopedic Overview
Anatomy of the Rotator Cuff
The rotator cuff is a musculotendinous unit composed of four muscles and their tendons, forming a cuff around the glenohumeral joint:
| Muscle | Nerve | Primary Action |
|---|---|---|
| Supraspinatus | Suprascapular (C5-C6) | Initiates abduction (0-15°) |
| Infraspinatus | Suprascapular (C5-C6) | External rotation |
| Teres Minor | Axillary (C5-C6) | External rotation |
| Subscapularis | Upper/Lower subscapular (C5-C6) | Internal rotation |
Together they function as dynamic stabilizers of the humeral head within the glenoid, counteracting the superior pull of the deltoid during arm elevation.
Pathophysiology and Disease Continuum
Rotator cuff disease is a continuum, not a discrete event. It progresses through:
- Mild impingement (subacromial outlet narrowing)
- Partial-thickness tear - articular-sided, bursal-sided, or interstitial
- Full-thickness tear - crescent, U-shaped, L-shaped, or massive contracted
- Rotator cuff tear arthropathy - end-stage with glenohumeral joint destruction
Key principle: "Bursa is bad" - bursal-side tears are more ominous than articular-side tears and progress more rapidly.
The pathophysiology involves a combination of factors:
- Decreased vascularity and cellularity of the tendon with aging (a critical "watershed zone" at the supraspinatus insertion)
- Collagen fiber changes
- Posterior capsular tightness causing cephalad humeral head migration
- Mechanical impingement under the coracoacromial arch
- External factors: trauma, repetitive overhead activities, corticosteroid use, systemic conditions (RA, lupus, renal osteodystrophy)
Tears most commonly begin at the anterolateral edge of the supraspinatus and progress posteriorly to involve the infraspinatus, then teres minor.
Classification
DeOrio & Cofield Classification (by size)
| Grade | Tear Size |
|---|---|
| Small | < 1 cm |
| Medium | 1-3 cm |
| Large | 3-5 cm |
| Massive | > 5 cm (two tendons) |
Note: Classification size does not predict prognosis.
By Depth
- Partial-thickness tears: articular-sided (PASTA lesion), bursal-sided, interstitial/intrasubstance
- Full-thickness tears: tendon torn completely from footprint
MRI Appearance of Rotator Cuff Tears
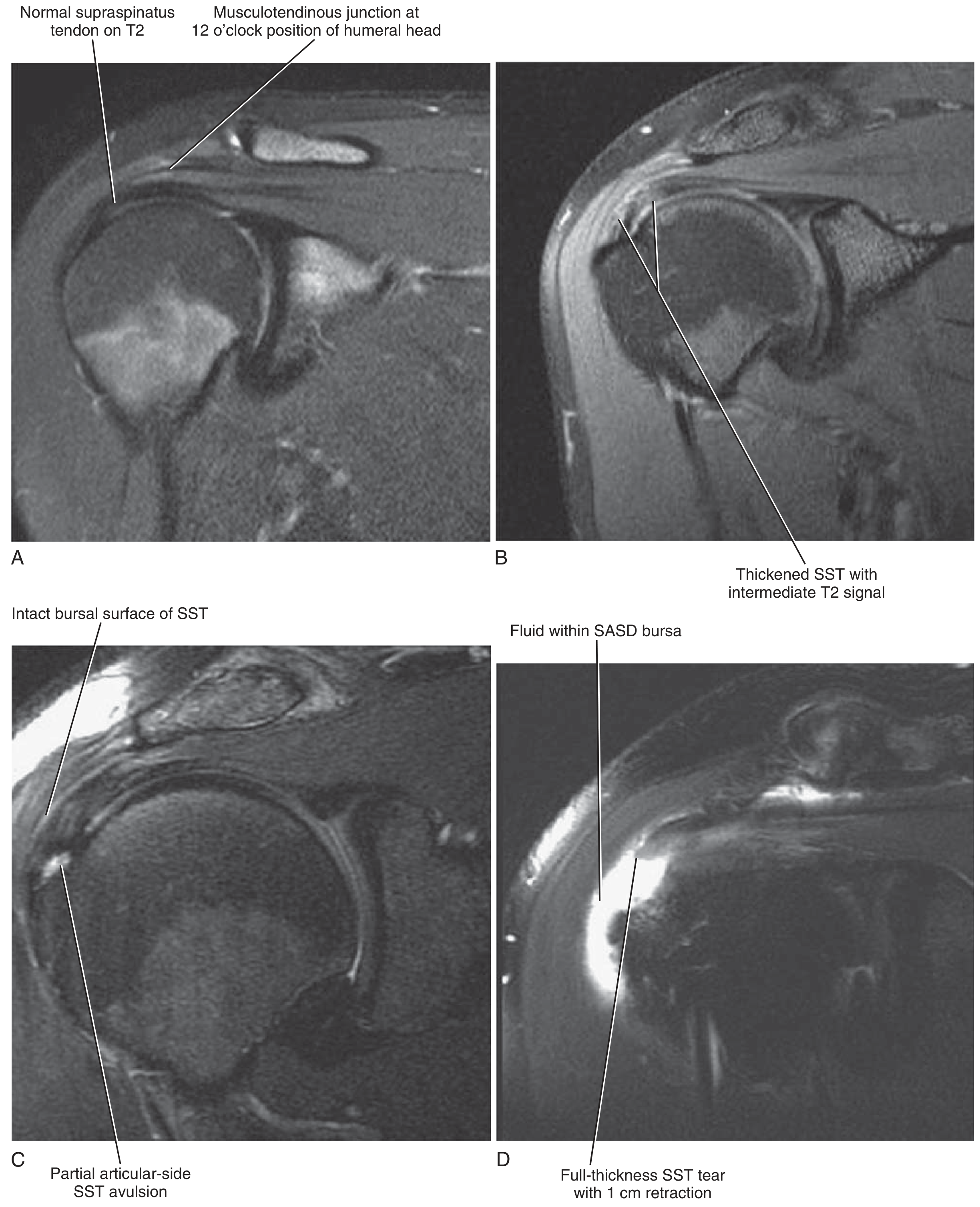
FIG. 4.52 - MRI appearances: (A) Normal supraspinatus tendon; (B) Thickened SST with intermediate T2 signal (tendinopathy); (C) Partial articular-side SST avulsion with intact bursal surface; (D) Full-thickness SST tear with fluid in the subacromial-subdeltoid (SASD) bursa. - Miller's Review of Orthopaedics 9th Ed.
Epidemiology
- 28% of patients >60 years have full-thickness tears
- 65% of patients >70 years have full-thickness tears
- A patient >60 with a unilateral rotator cuff tear has a 50% risk of bilateral tears
- A patient with a painful full-thickness tear has a 56% chance of an asymptomatic contralateral full/partial thickness tear
- Of those with asymptomatic tears: 50% become symptomatic within 3 years, and 40% of those will show tear progression
Clinical Presentation
History
- Insidious onset of pain exacerbated by overhead activities
- Night pain - a classic feature (often wakes patients)
- Pain in the deltoid region (referred)
- Muscular weakness, especially with abduction and external rotation
- Difficulty with ADLs: combing hair, reaching back pocket, hooking a bra strap, putting on a coat
- Acute-onset pain and weakness after trauma (fall on outstretched arm, lifting heavy object) suggests acute tear
In younger patients, onset requires relatively major trauma; in older adults, a simple fall or even spontaneous onset is possible.
Physical Examination
Key tests by tendon:
| Test | Tendon Tested | Positive Finding |
|---|---|---|
| Empty Can (Jobe's) | Supraspinatus | Weakness/pain with resisted abduction at 90°, 30° forward flexion, IR |
| Drop Arm Test | Supraspinatus (full-thickness) | Inability to lower arm smoothly |
| External Rotation Lag Sign | Infraspinatus | Cannot maintain passive ER |
| Hornblower's Sign | Teres minor | Cannot ER with shoulder abducted |
| Belly Press / Lift-off (Gerber's) | Subscapularis | Cannot press abdomen or lift hand off back |
| Bear Hug Test | Subscapularis | Weakness of IR against resistance |
| Neer Impingement Sign | Subacromial space | Pain with passive forward flexion (arm internally rotated) |
| Hawkins-Kennedy | Subacromial impingement | Pain with internal rotation at 90° forward flexion |
Key examination principle: If pain is removed with a subacromial local anaesthetic injection, persistent weakness confirms a structural tear rather than pain inhibition.
Imaging
Plain Radiograph (X-ray)
- First-line, establishes baseline
- May show: acromial spurring, calcification, cystic changes in greater tuberosity
- Acromiohumeral distance < 7 mm on AP view suggests massive tear / irreparable cuff (superior humeral head migration)
- With chronic disease: superior migration of humeral head + glenohumeral degenerative changes
Ultrasonography
- Increasing popularity for initial diagnosis and for guiding injections (subacromial or intraarticular)
- Dynamic assessment is an advantage
- Operator-dependent
MRI (Gold Standard for Surgical Planning)
- Defines: extent of tear, degree of retraction, presence of muscular atrophy, fatty infiltration
- Goutallier classification grades fatty infiltration (originally based on CT, now applied to MRI)
- Larger, more retracted tears (>40 mm) show fatty atrophy, supraspinatus width <5 mm at glenoid margin, high T2 signal in infraspinatus
- Tangent sign: failure of the supraspinatus muscle belly to reach a line tangent to the superior borders of scapular spine and coracoid - indicates advanced atrophy
Treatment
Conservative (Non-Surgical)
First-line for most patients:
- NSAIDs for pain and inflammation
- Subacromial corticosteroid injection (guided or landmark-based)
- Physiotherapy - structured in phases:
Phase 1: Restore range of motion - passive stretching, pendulum exercises, posterior capsular stretching (for posterior capsular contracture)
Phase 2: Strengthening - once motion is restored with minimal discomfort; rotator cuff strengthening out of the impingement arc (70-120° of shoulder flexion), deltoid and periscapular muscle strengthening (serratus anterior, trapezius), elastic resistance bands
Phase 3: Gradual return to overhead activities, work, and sport - individualized to patient needs
Conservative trial duration: 3-6 months before surgical consideration, especially in older, sedentary patients.
Surgical Indications
Primary drivers for surgery:
- Severity and duration of pain despite conservative management
- Significant weakness with functional disability (may warrant earlier surgery)
- Acute tear in a young/athletic patient - early surgical intervention is preferred
Other decision factors: shoulder dominance, activity level, physiologic (not chronologic) age, acuteness of tear, degree/size, retraction, fatty atrophy of remaining musculature.
Note: older chronologic age alone does not portend worse surgical outcomes. However, pending workers' compensation claims negatively affect treatment results.
Surgical Options
| Technique | Details |
|---|---|
| Arthroscopic repair | All-arthroscopic, now the dominant technique; minimally invasive |
| Mini-open (deltoid-sparing) | Transitional technique |
| Open repair | Classic approach, now reserved for complex/revision cases |
| Double-row / suture-bridge fixation | Improved biomechanical strength in vitro; clinical superiority remains debated |
Key surgical principles:
- Routine acromioplasty is no longer recommended during rotator cuff repair
- Biologic healing of tendon-to-bone requires a minimum of 8-12 weeks regardless of technique - this is the rate-limiting step
- Blood flow to the repair comes from peribursal tissue and bone anchor site; vascularity increases with exercise
Partial-thickness tears (articular-sided / PASTA lesion):
- Tear < 50% thickness: debridement + subacromial decompression
- Tear > 50% thickness (>7 mm bone lateral to articular margin exposed): repair recommended
Massive and Irreparable Tears:
- Failure rate for repair is higher
- Irreparable when: acromiohumeral distance <7 mm, large fatty atrophy, high retraction
- Options for irreparable combined supraspinatus + infraspinatus tears: latissimus dorsi transfer, superior capsular reconstruction, or reverse total shoulder arthroplasty (in older patients with rotator cuff tear arthropathy)
Post-repair rehabilitation:
- A 2025 systematic review (Hao et al., PMID 40082920) found that early exercise vs. immobilization after arthroscopic repair remains a nuanced decision - outcomes are comparable, but protocols should be individualized.
Complications and Natural History
- Untreated full-thickness tears progress in size over time (40% of symptomatic tears enlarge)
- Tear progression leads to muscle atrophy and irreversible fatty infiltration
- End-stage disease: rotator cuff tear arthropathy - superior humeral migration, glenohumeral and acromioclavicular articular destruction
- Post-repair retear rates are higher for larger tears; tissue failure (not anchor pullout) is the most common failure mode
Recent Evidence Updates (2024-2026)
- Bioinductive patches as augmentation (Warren et al., 2024, PMID 38942225): Systematic review/meta-analysis examining bioinductive patches as augmentation for rotator cuff repair - emerging technology showing promise for improving healing rates.
- PRP does not significantly improve outcomes (Xue et al., 2025, PMID 38609023): Arthroscopic surgery combined with PRP does not significantly improve pain, function, complication rates, or retear rates compared to arthroscopic surgery alone for full-thickness tears.
- Post-repair rehabilitation timing (Hao et al., 2025, PMID 40082920): Early exercise vs. immobilization after arthroscopic repair - outcomes are comparable; individualized protocols are recommended.
Sources:
- Miller's Review of Orthopaedics, 9th Edition
- Firestein & Kelley's Textbook of Rheumatology, 2-Volume Set
- Bailey and Love's Short Practice of Surgery, 28th Edition
- Schwartz's Principles of Surgery, 11th Edition
This is a shared conversation. Sign in to Orris to start your own chat.