Easy simple Notes with images
python3 -c " import pdfplumber pdf_path = '/home/daytona/workspace/attachments/b…
python3 -c " import pdfplumber pdf_path = '/home/daytona/workspace/attachments/b…
~/endo-notes/Endometriosis_Adenomyosis_Notes.html
<!DOCTYPE html>
<html lang="en">
<head>
<meta charset="UTF-8">
<meta name="viewport" content="width=device-width, initial-scale=1.0">
<title>Endometriosis & Adenomyosis – Easy Notes</title>
<style>
@import url('https://fonts.googleapis.com/css2?family=Inter:wght@400;500;600;700;800&display=swap');
* { box-sizing: border-box; margin: 0; padding: 0; }
body {
font-family: 'Inter', sans-serif;
background: #f0f4f8;
color: #1a202c;
line-height: 1.6;
padding: 20px;
}
/* ── COVER ── */
.cover {
background: linear-gradient(135deg, #c0392b 0%, #8e44ad 50%, #2c3e50 100%);
color: white;
border-radius: 20px;
padding: 50px 40px;
text-align: center;
margin-bottom: 30px;
box-shadow: 0 10px 40px rgba(0,0,0,0.25);
}
.cover h1 { font-size: 2.8rem; font-weight: 800; margin-bottom: 8px; }
.cover h2 { font-size: 1.3rem; font-weight: 400; opacity: 0.9; }
.cover .badge {
display: inline-block;
background: rgba(255,255,255,0.2);
border-radius: 50px;
padding: 6px 20px;
font-size: 0.85rem;
margin-top: 16px;
}
/* ── SECTION HEADERS ── */
.section-header {
display: flex;
align-items: center;
gap: 14px;
padding: 18px 24px;
border-radius: 14px;
margin: 30px 0 16px 0;
color: white;
font-size: 1.5rem;
font-weight: 700;
}
.section-header .icon { font-size: 2rem; }
.endo-header { background: linear-gradient(135deg, #c0392b, #e74c3c); }
.adeno-header { background: linear-gradient(135deg, #6c3483, #8e44ad); }
/* ── CARDS ── */
.card {
background: white;
border-radius: 14px;
padding: 22px 26px;
margin-bottom: 16px;
box-shadow: 0 2px 12px rgba(0,0,0,0.07);
border-left: 5px solid #e74c3c;
}
.card.purple { border-left-color: #8e44ad; }
.card.blue { border-left-color: #2980b9; }
.card.green { border-left-color: #27ae60; }
.card.orange { border-left-color: #e67e22; }
.card.teal { border-left-color: #16a085; }
.card.pink { border-left-color: #e84393; }
.card h3 {
font-size: 1.05rem;
font-weight: 700;
margin-bottom: 12px;
display: flex;
align-items: center;
gap: 8px;
}
/* ── GRID ── */
.grid-2 { display: grid; grid-template-columns: 1fr 1fr; gap: 16px; margin-bottom: 16px; }
.grid-3 { display: grid; grid-template-columns: 1fr 1fr 1fr; gap: 16px; margin-bottom: 16px; }
@media(max-width: 700px) {
.grid-2, .grid-3 { grid-template-columns: 1fr; }
}
/* ── LISTS ── */
ul.dotlist { list-style: none; padding: 0; }
ul.dotlist li { padding: 4px 0; padding-left: 22px; position: relative; font-size: 0.92rem; }
ul.dotlist li::before { content: '●'; color: #e74c3c; position: absolute; left: 0; font-size: 0.7rem; top: 7px; }
.card.purple ul.dotlist li::before { color: #8e44ad; }
.card.blue ul.dotlist li::before { color: #2980b9; }
.card.green ul.dotlist li::before { color: #27ae60; }
.card.orange ul.dotlist li::before { color: #e67e22; }
.card.teal ul.dotlist li::before { color: #16a085; }
.card.pink ul.dotlist li::before { color: #e84393; }
/* ── FLOW DIAGRAM ── */
.flow {
display: flex;
flex-direction: column;
align-items: center;
gap: 0;
padding: 10px 0;
}
.flow-box {
background: #fdf2f2;
border: 2px solid #e74c3c;
border-radius: 10px;
padding: 10px 24px;
font-size: 0.88rem;
font-weight: 600;
color: #c0392b;
text-align: center;
min-width: 220px;
}
.flow-box.purple-box {
background: #f5eef8;
border-color: #8e44ad;
color: #6c3483;
}
.flow-arrow {
font-size: 1.4rem;
color: #999;
line-height: 1;
}
/* ── ALERT BOXES ── */
.alert {
border-radius: 10px;
padding: 14px 18px;
margin: 10px 0;
font-size: 0.88rem;
font-weight: 600;
display: flex;
align-items: flex-start;
gap: 10px;
}
.alert-red { background: #fdecea; color: #c0392b; border: 1.5px solid #e74c3c; }
.alert-purple { background: #f5eef8; color: #6c3483; border: 1.5px solid #8e44ad; }
.alert-blue { background: #eaf4fc; color: #1a5276; border: 1.5px solid #2980b9; }
.alert-green { background: #eafaf1; color: #1e8449; border: 1.5px solid #27ae60; }
.alert-orange { background: #fef9e7; color: #935116; border: 1.5px solid #e67e22; }
.alert .alert-icon { font-size: 1.3rem; flex-shrink: 0; }
/* ── TRIAD BOX ── */
.triad {
display: flex;
gap: 10px;
justify-content: center;
margin: 12px 0;
flex-wrap: wrap;
}
.triad-item {
background: linear-gradient(135deg, #c0392b, #e74c3c);
color: white;
border-radius: 50px;
padding: 10px 22px;
font-weight: 700;
font-size: 0.9rem;
text-align: center;
}
.triad-item.purple-triad {
background: linear-gradient(135deg, #6c3483, #8e44ad);
}
/* ── STAGE TABLE ── */
table.stage-table {
width: 100%;
border-collapse: collapse;
font-size: 0.88rem;
margin-top: 10px;
}
table.stage-table th {
background: #e74c3c;
color: white;
padding: 8px 12px;
text-align: left;
font-weight: 700;
}
table.stage-table td {
padding: 8px 12px;
border-bottom: 1px solid #f0f0f0;
}
table.stage-table tr:nth-child(even) td { background: #fdf5f5; }
table.stage-table.purple-table th { background: #8e44ad; }
table.stage-table.purple-table tr:nth-child(even) td { background: #f9f4fc; }
/* ── COMPARE BOX ── */
.compare {
display: grid;
grid-template-columns: 1fr 1fr;
gap: 16px;
margin-bottom: 16px;
}
.compare-col {
border-radius: 14px;
padding: 20px;
background: white;
box-shadow: 0 2px 12px rgba(0,0,0,0.07);
}
.compare-col.red-col { border-top: 5px solid #e74c3c; }
.compare-col.purple-col { border-top: 5px solid #8e44ad; }
.compare-col h3 { font-size: 1rem; font-weight: 700; margin-bottom: 12px; }
.compare-col.red-col h3 { color: #c0392b; }
.compare-col.purple-col h3 { color: #6c3483; }
@media(max-width: 600px) { .compare { grid-template-columns: 1fr; } }
/* ── TREATMENT PILL ── */
.pill-group { display: flex; flex-wrap: wrap; gap: 8px; margin-top: 8px; }
.pill {
border-radius: 50px;
padding: 5px 14px;
font-size: 0.82rem;
font-weight: 600;
border: 2px solid;
}
.pill-red { background: #fdecea; color: #c0392b; border-color: #e74c3c; }
.pill-purple { background: #f5eef8; color: #6c3483; border-color: #8e44ad; }
.pill-blue { background: #eaf4fc; color: #1a5276; border-color: #2980b9; }
.pill-green { background: #eafaf1; color: #1e8449; border-color: #27ae60; }
.pill-orange { background: #fef9e7; color: #935116; border-color: #e67e22; }
.pill-teal { background: #e8f8f5; color: #0e6655; border-color: #16a085; }
/* ── SITE DIAGRAM ── */
.site-diagram {
background: #fdf2f2;
border-radius: 14px;
padding: 20px;
text-align: center;
position: relative;
}
.site-diagram svg { max-width: 100%; height: auto; }
/* ── DIVIDER ── */
.divider {
height: 3px;
background: linear-gradient(90deg, #e74c3c, #8e44ad);
border-radius: 10px;
margin: 30px 0;
}
/* ── KEY DIFF ── */
.keydiff {
background: linear-gradient(135deg, #fdecea, #f5eef8);
border-radius: 14px;
padding: 22px 26px;
margin: 20px 0;
border: 2px dashed #c39bd3;
}
.keydiff h3 { font-size: 1.1rem; font-weight: 700; color: #4a235a; margin-bottom: 14px; text-align: center; }
/* ── FOOTER ── */
.footer {
text-align: center;
color: #999;
font-size: 0.82rem;
margin-top: 30px;
padding: 16px;
}
</style>
</head>
<body>
<!-- ═══════════ COVER ═══════════ -->
<div class="cover">
<div style="font-size:4rem; margin-bottom:12px;">🩺</div>
<h1>Endometriosis & Adenomyosis</h1>
<h2>Easy Study Notes — Batch 2022-23 | Dr Vivek Jog</h2>
<div class="badge">📚 Gynaecology | OBG</div>
</div>
<!-- ═══════════ ENDOMETRIOSIS ═══════════ -->
<div class="section-header endo-header">
<span class="icon">🔴</span>
<span>ENDOMETRIOSIS</span>
</div>
<!-- Definition + Importance -->
<div class="grid-2">
<div class="card">
<h3>📖 Definition</h3>
<p style="font-size:0.93rem; background:#fdecea; border-radius:8px; padding:12px; color:#7b241c;">
Presence of <strong>functional endometrial glands and stroma</strong> <em>outside</em> the uterine cavity → chronic inflammatory reaction.
</p>
</div>
<div class="card green">
<h3>📊 Importance / Epidemiology</h3>
<ul class="dotlist">
<li>Affects <strong>6–10%</strong> of reproductive-age women</li>
<li>Present in <strong>30–50%</strong> of infertile women</li>
<li>Commonest cause of <strong>chronic pelvic pain</strong></li>
<li>Peak age: <strong>25–40 years</strong></li>
<li>Estrogen-dependent; rare before menarche / after menopause</li>
</ul>
</div>
</div>
<!-- Risk / Protective -->
<div class="grid-2">
<div class="card orange">
<h3>⚠️ Risk Factors</h3>
<ul class="dotlist">
<li>Early menarche</li>
<li>Short menstrual cycles (<27 days)</li>
<li>Heavy menstrual bleeding</li>
<li>Nulliparity</li>
<li>Family history</li>
<li>Delayed childbearing</li>
</ul>
</div>
<div class="card teal">
<h3>🛡️ Protective Factors</h3>
<ul class="dotlist">
<li>Multiparity</li>
<li>Lactation</li>
<li>Regular exercise</li>
</ul>
</div>
</div>
<!-- Pathogenesis -->
<div class="card blue">
<h3>🔬 Pathogenesis</h3>
<div class="grid-2" style="margin-top:10px;">
<div>
<div style="font-weight:700; color:#1a5276; margin-bottom:8px;">Sampson's Theory (Most Accepted)</div>
<div class="flow">
<div class="flow-box">Retrograde menstruation</div>
<div class="flow-arrow">▼</div>
<div class="flow-box">Endometrial cells → peritoneal cavity</div>
<div class="flow-arrow">▼</div>
<div class="flow-box">Implantation</div>
<div class="flow-arrow">▼</div>
<div class="flow-box">Inflammation</div>
<div class="flow-arrow">▼</div>
<div class="flow-box">Fibrosis & Adhesions</div>
</div>
</div>
<div>
<div style="font-weight:700; color:#1a5276; margin-bottom:8px;">Other Theories</div>
<ul class="dotlist">
<li>Coelomic metaplasia</li>
<li>Lymphatic/vascular dissemination (Halban)</li>
<li>Stem cell theory</li>
<li>Altered immunity</li>
<li>Genetic predisposition</li>
</ul>
<div class="alert alert-blue" style="margin-top:12px;">
<span class="alert-icon">📝</span>
<span>Retrograde menstruation <em>alone</em> is insufficient — immune dysfunction also contributes.</span>
</div>
</div>
</div>
</div>
<!-- Sites + Types -->
<div class="grid-2">
<div class="card">
<h3>📍 Common Sites</h3>
<div style="font-weight:600; color:#c0392b; margin-bottom:6px;">Pelvic (more common)</div>
<ul class="dotlist">
<li><strong>Ovaries</strong> (most common) ★</li>
<li>Pouch of Douglas</li>
<li>Uterosacral ligaments</li>
<li>Pelvic peritoneum</li>
<li>Rectovaginal septum</li>
<li>Fallopian tubes</li>
</ul>
<div style="font-weight:600; color:#c0392b; margin-top:10px; margin-bottom:6px;">Extra-pelvic (rare)</div>
<ul class="dotlist">
<li>Intestine, Urinary bladder</li>
<li>Caesarean scar, Umbilicus</li>
<li>Diaphragm, Pleura</li>
</ul>
</div>
<div class="card purple">
<h3>📋 ASRM Classification</h3>
<table class="stage-table">
<tr><th>Stage</th><th>Severity</th></tr>
<tr><td><strong>I</strong></td><td>Minimal</td></tr>
<tr><td><strong>II</strong></td><td>Mild</td></tr>
<tr><td><strong>III</strong></td><td>Moderate</td></tr>
<tr><td><strong>IV</strong></td><td>Severe</td></tr>
</table>
<p style="font-size:0.82rem; margin-top:10px; color:#555;">Based on: number of lesions, size, adhesions, ovarian involvement</p>
<div class="alert alert-red" style="margin-top:10px;">
<span class="alert-icon">⚠️</span>
<span>Stage <strong>does NOT</strong> always correlate with symptom severity!</span>
</div>
<div style="font-weight:600; margin-top:12px; margin-bottom:6px;">Types</div>
<div class="pill-group">
<span class="pill pill-red">Superficial peritoneal</span>
<span class="pill pill-red">Ovarian endometrioma</span>
<span class="pill pill-red">DIE (Deep infiltrating)</span>
</div>
</div>
</div>
<!-- Clinical Triad -->
<div class="card" style="text-align:center;">
<h3 style="justify-content:center; color:#c0392b;">🎯 Classical Triad of Endometriosis</h3>
<div class="triad">
<div class="triad-item">😣 Dysmenorrhoea<br><small style="font-weight:400;">Progressive</small></div>
<div class="triad-item">💔 Dyspareunia<br><small style="font-weight:400;">Deep</small></div>
<div class="triad-item">🤰 Infertility<br><small style="font-weight:400;">Sub/infertility</small></div>
</div>
<div style="font-size:0.85rem; color:#777; margin-top:6px;">Also: Chronic pelvic pain • Dyschezia • Dysuria • Menorrhagia</div>
</div>
<!-- Signs -->
<div class="card green">
<h3>🩺 Clinical Signs</h3>
<div class="pill-group">
<span class="pill pill-green">Fixed retroverted uterus</span>
<span class="pill pill-green">Restricted uterine mobility</span>
<span class="pill pill-green">Tender uterosacral nodules</span>
<span class="pill pill-green">Adnexal mass (endometrioma)</span>
<span class="pill pill-green">Cervical motion tenderness</span>
</div>
</div>
<!-- Diagnosis flowchart -->
<div class="card blue">
<h3>🔍 Diagnostic Approach</h3>
<div class="flow">
<div class="flow-box">Woman: Progressive dysmenorrhoea / Chronic pelvic pain / Dyspareunia / Infertility</div>
<div class="flow-arrow">▼</div>
<div class="flow-box">Clinical examination</div>
<div class="flow-arrow">▼</div>
<div class="flow-box">Transvaginal USG (TVS) — First-line imaging</div>
<div class="flow-arrow">▼</div>
<div class="flow-box">MRI — if Deep Infiltrating Endometriosis suspected</div>
<div class="flow-arrow">▼</div>
<div class="flow-box">🏆 Laparoscopy + Biopsy = GOLD STANDARD</div>
</div>
</div>
<!-- Investigations -->
<div class="grid-2">
<div class="card orange">
<h3>🧪 Investigations</h3>
<div style="font-weight:600; margin-bottom:6px;">Labs</div>
<ul class="dotlist">
<li>No test is diagnostic</li>
<li>CA-125: mildly elevated; NOT for screening — only to monitor response</li>
<li>CBC (if heavy bleeding), Urine (if urinary symptoms)</li>
</ul>
</div>
<div class="card">
<h3>🖥️ Imaging Findings</h3>
<div style="font-weight:600; margin-bottom:4px; color:#c0392b;">TVS — Endometrioma</div>
<ul class="dotlist">
<li>Unilocular cyst</li>
<li><strong>"Ground-glass"</strong> low-level internal echoes</li>
<li>Thick wall, minimal vascularity</li>
</ul>
<div style="font-weight:600; margin-top:10px; margin-bottom:4px; color:#c0392b;">Laparoscopy</div>
<ul class="dotlist">
<li>🔵 Powder-burn / blue-black lesions</li>
<li>🍫 Chocolate cyst (endometrioma)</li>
<li>Dense adhesions / Frozen pelvis</li>
</ul>
</div>
</div>
<!-- Infertility -->
<div class="card pink">
<h3>🤰 Endometriosis & Infertility</h3>
<div class="grid-2">
<div>
<div style="font-weight:600; margin-bottom:6px;">Mechanisms:</div>
<ul class="dotlist">
<li>Distorted pelvic anatomy</li>
<li>Tubal dysfunction & adhesions</li>
<li>Impaired ovulation</li>
<li>Altered peritoneal environment</li>
<li>Reduced implantation</li>
</ul>
</div>
<div>
<div style="font-weight:600; margin-bottom:6px;">Fertility Treatment:</div>
<ul class="dotlist">
<li><strong>Minimal–mild:</strong> Laparoscopy ± IUI</li>
<li><strong>Moderate–severe:</strong> IVF preferred</li>
</ul>
</div>
</div>
</div>
<!-- Management Medical -->
<div class="card">
<h3>💊 Medical Management</h3>
<div class="alert alert-orange" style="margin-bottom:12px;">
<span class="alert-icon">⚠️</span>
<span>Medical therapy <strong>relieves symptoms but does NOT improve fertility.</strong></span>
</div>
<div class="grid-2">
<div>
<div style="font-weight:600; margin-bottom:6px;">Indications:</div>
<ul class="dotlist">
<li>Mild–moderate symptoms</li>
<li>No large endometrioma</li>
<li>No immediate desire for pregnancy</li>
<li>Adjunct after conservative surgery</li>
</ul>
</div>
<div>
<div style="font-weight:600; margin-bottom:6px;">Drug Options:</div>
<div class="pill-group">
<span class="pill pill-blue">NSAIDs (1st line pain)</span>
<span class="pill pill-blue">COCPs (1st line hormonal)</span>
<span class="pill pill-blue">Progestins (Dienogest, MPA, NETA)</span>
<span class="pill pill-blue">LNG-IUS</span>
<span class="pill pill-blue">GnRH Agonists (+ add-back >6mo)</span>
<span class="pill pill-blue">GnRH Antagonists (Elagolix)</span>
<span class="pill pill-orange">Danazol (2nd line, androgenic SE)</span>
<span class="pill pill-orange">Aromatase inhibitors (refractory)</span>
</div>
</div>
</div>
</div>
<!-- Management Surgical -->
<div class="card green">
<h3>🔪 Surgical Management</h3>
<div class="grid-2">
<div>
<div style="font-weight:600; margin-bottom:6px;">Indications:</div>
<ul class="dotlist">
<li>Severe pain not responding to medical Rx</li>
<li>Endometrioma >4 cm</li>
<li>Deep infiltrating endometriosis</li>
<li>Infertility with correctable disease</li>
<li>Suspicion of malignancy</li>
</ul>
</div>
<div>
<div style="font-weight:600; margin-bottom:6px; color:#1e8449;">Conservative (Laparoscopy):</div>
<ul class="dotlist">
<li>Excision / ablation of implants</li>
<li>Adhesiolysis</li>
<li>Ovarian cystectomy</li>
<li>Restore pelvic anatomy</li>
</ul>
<div style="font-weight:600; margin: 8px 0 6px; color:#c0392b;">Definitive:</div>
<ul class="dotlist">
<li>Total hysterectomy + BSO</li>
<li>For completed family / recurrent disease</li>
</ul>
</div>
</div>
</div>
<!-- ═══════════ DIVIDER ═══════════ -->
<div class="divider"></div>
<!-- ═══════════ ADENOMYOSIS ═══════════ -->
<div class="section-header adeno-header">
<span class="icon">🟣</span>
<span>ADENOMYOSIS</span>
</div>
<!-- Definition + Importance -->
<div class="grid-2">
<div class="card purple">
<h3>📖 Definition</h3>
<p style="font-size:0.93rem; background:#f5eef8; border-radius:8px; padding:12px; color:#4a235a;">
Presence of <strong>endometrial glands and stroma within the myometrium</strong>, with hypertrophy & hyperplasia of surrounding smooth muscle.
</p>
</div>
<div class="card teal">
<h3>📊 Importance / Epidemiology</h3>
<ul class="dotlist">
<li>Affects <strong>35–50 year</strong> women</li>
<li>Incidence <strong>20–35%</strong></li>
<li>Common in <strong>multiparous</strong> women</li>
<li>Important cause of AUB, secondary dysmenorrhoea, chronic pelvic pain</li>
<li>Frequently coexists with fibroids & endometriosis</li>
</ul>
</div>
</div>
<!-- Risk Factors Adenomyosis -->
<div class="card orange">
<h3>⚠️ Risk Factors</h3>
<div class="pill-group">
<span class="pill pill-orange">Multiparity</span>
<span class="pill pill-orange">Increasing age</span>
<span class="pill pill-orange">Previous uterine surgery (C/S, D&C, myomectomy)</span>
<span class="pill pill-orange">Early menarche</span>
<span class="pill pill-orange">Short menstrual cycles</span>
<span class="pill pill-orange">Hyperestrogenic states</span>
</div>
</div>
<!-- Pathogenesis Adenomyosis -->
<div class="card purple">
<h3>🔬 Pathogenesis</h3>
<div class="grid-2">
<div>
<div style="font-weight:700; color:#6c3483; margin-bottom:8px;">Most Accepted Theory</div>
<div class="flow">
<div class="flow-box purple-box">Basal endometrium</div>
<div class="flow-arrow" style="color:#8e44ad;">▼</div>
<div class="flow-box purple-box">Break in junctional zone</div>
<div class="flow-arrow" style="color:#8e44ad;">▼</div>
<div class="flow-box purple-box">Invagination into myometrium</div>
<div class="flow-arrow" style="color:#8e44ad;">▼</div>
<div class="flow-box purple-box">Cyclic bleeding → Inflammation</div>
<div class="flow-arrow" style="color:#8e44ad;">▼</div>
<div class="flow-box purple-box">Smooth muscle hypertrophy</div>
<div class="flow-arrow" style="color:#8e44ad;">▼</div>
<div class="flow-box purple-box">Diffuse uterine enlargement</div>
</div>
</div>
<div>
<div style="font-weight:700; color:#6c3483; margin-bottom:8px;">Other Theories</div>
<ul class="dotlist">
<li>Metaplasia of Müllerian remnants</li>
<li>TIAR (Tissue Injury & Repair) mechanism</li>
<li>Stem cell theory</li>
</ul>
<div class="alert alert-purple" style="margin-top:12px;">
<span class="alert-icon">🔑</span>
<span>Adenomyosis is <strong>estrogen-dependent</strong> (like endometriosis).</span>
</div>
</div>
</div>
</div>
<!-- Pathology -->
<div class="grid-2">
<div class="card">
<h3>🔬 Pathology</h3>
<div style="font-weight:600; margin-bottom:6px; color:#c0392b;">Types</div>
<ul class="dotlist">
<li><strong>Diffuse</strong> — most common; endometrial tissue diffusely infiltrates myometrium</li>
<li><strong>Focal (Adenomyoma)</strong> — localized nodule; mimics fibroid</li>
</ul>
<div style="font-weight:600; margin-top:10px; margin-bottom:6px; color:#c0392b;">Gross Pathology</div>
<ul class="dotlist">
<li>Uniformly enlarged <strong>"globular uterus"</strong></li>
<li>Thickened, trabeculated myometrium</li>
<li>Small hemorrhagic cysts</li>
</ul>
</div>
<div class="card purple">
<h3>🔬 Histopathology</h3>
<div class="alert alert-purple">
<span class="alert-icon">📐</span>
<span>Endometrial glands & stroma <strong>≥2.5 mm below the endometrial-myometrial junction</strong> (or 1 low-power field beneath basalis) + surrounding smooth muscle hyperplasia</span>
</div>
<div style="font-weight:600; margin-top:12px; margin-bottom:6px;">Associated Conditions</div>
<ul class="dotlist">
<li>Leiomyoma (fibroid)</li>
<li>Endometriosis</li>
<li>Endometrial hyperplasia</li>
</ul>
</div>
</div>
<!-- Clinical features Adenomyosis -->
<div class="card purple" style="text-align:center; margin-bottom:16px;">
<h3 style="justify-content:center; color:#6c3483;">🎯 Classic Presentation</h3>
<div class="triad">
<div class="triad-item purple-triad">🩸 Menorrhagia<br><small style="font-weight:400;">Most common</small></div>
<div class="triad-item purple-triad">😣 Dysmenorrhoea<br><small style="font-weight:400;">Progressive, secondary</small></div>
<div class="triad-item purple-triad">🫃 Globular Uterus<br><small style="font-weight:400;">Boggy, tender</small></div>
</div>
</div>
<div class="card">
<h3>🩺 Signs on Examination</h3>
<div class="pill-group">
<span class="pill pill-teal">Uniformly enlarged uterus</span>
<span class="pill pill-teal">Globular shape</span>
<span class="pill pill-teal">Soft / "boggy" consistency</span>
<span class="pill pill-teal">Tender uterus</span>
<span class="pill pill-teal">Reduced mobility (if coexisting endo)</span>
</div>
<div class="alert alert-purple" style="margin-top:12px;">
<span class="alert-icon">💡</span>
<span><strong>Clinical Clue:</strong> Severe dysmenorrhoea + uniformly enlarged, tender, boggy uterus = strongly suspect adenomyosis</span>
</div>
</div>
<!-- Investigations Adenomyosis -->
<div class="grid-2">
<div class="card blue">
<h3>🖥️ TVS Findings</h3>
<ul class="dotlist">
<li>Globular uterus</li>
<li>Asymmetrical myometrial thickening</li>
<li>Heterogeneous myometrium</li>
<li>Myometrial cysts</li>
<li>Fan-shaped shadowing</li>
<li>Indistinct endo-myometrial junction</li>
</ul>
</div>
<div class="card purple">
<h3>🧲 MRI (Best Imaging)</h3>
<ul class="dotlist">
<li>Thickened junctional zone (<strong>>12 mm</strong>)</li>
<li>Myometrial cysts</li>
<li>Diffuse or focal pattern</li>
</ul>
<div style="font-weight:600; margin-top:10px; margin-bottom:4px;">MRI preferred when:</div>
<ul class="dotlist">
<li>Diagnosis uncertain</li>
<li>Differentiating from fibroid</li>
<li>Planning conservative surgery</li>
</ul>
<div class="alert alert-purple" style="margin-top:10px;">
<span class="alert-icon">🏆</span>
<span>Gold standard = <strong>Histopathology</strong> of hysterectomy specimen</span>
</div>
</div>
</div>
<!-- Management Adenomyosis -->
<div class="card purple">
<h3>💊 Medical Management</h3>
<div class="grid-2">
<div>
<div style="font-weight:600; margin-bottom:6px;">Indications:</div>
<ul class="dotlist">
<li>Mild–moderate symptoms</li>
<li>Desire to preserve fertility</li>
<li>Perimenopausal women</li>
<li>Unsuitable for surgery</li>
</ul>
</div>
<div>
<div style="font-weight:600; margin-bottom:6px;">Options:</div>
<div class="pill-group">
<span class="pill pill-purple">NSAIDs (dysmenorrhoea)</span>
<span class="pill pill-purple">Tranexamic acid (blood loss)</span>
<span class="pill pill-purple">COCPs</span>
<span class="pill pill-purple">Progestins (Dienogest, MPA, NETA)</span>
<span class="pill pill-purple">LNG-IUS ⭐ Most effective long-term</span>
<span class="pill pill-purple">GnRH Agonists (max 3–6 months)</span>
</div>
</div>
</div>
</div>
<!-- Surgical Adenomyosis + Algorithm -->
<div class="grid-2">
<div class="card green">
<h3>🔪 Surgical Management</h3>
<div style="font-weight:600; margin-bottom:6px; color:#1e8449;">Conservative (fertility preserving):</div>
<ul class="dotlist">
<li>Adenomyomectomy (focal disease)</li>
<li>Endometrial ablation (no future pregnancy)</li>
<li>Uterine artery embolization</li>
<li>MRI-guided focused ultrasound</li>
</ul>
<div style="font-weight:600; margin-top:10px; margin-bottom:6px; color:#c0392b;">Definitive: Total Hysterectomy</div>
<ul class="dotlist">
<li>Completed family</li>
<li>Severe / refractory symptoms</li>
<li>Diffuse adenomyosis</li>
</ul>
<div class="alert alert-green" style="margin-top:10px;">
<span class="alert-icon">ℹ️</span>
<span>Ovaries are preserved unless another indication exists.</span>
</div>
</div>
<div class="card blue">
<h3>🗺️ Treatment Algorithm</h3>
<div class="flow">
<div class="flow-box" style="background:#f5eef8; border-color:#8e44ad; color:#6c3483;">Symptomatic adenomyosis</div>
<div class="flow-arrow">▼</div>
<div class="flow-box" style="background:#f5eef8; border-color:#8e44ad; color:#6c3483;">Desires fertility?</div>
<div style="display:flex; gap:16px; margin:8px 0;">
<div style="text-align:center;">
<div style="font-weight:700; color:#27ae60;">YES</div>
<div class="flow-box" style="background:#eafaf1; border-color:#27ae60; color:#1e8449; min-width:140px;">Medical therapy ± Conservative surgery</div>
</div>
<div style="text-align:center;">
<div style="font-weight:700; color:#c0392b;">NO</div>
<div class="flow-box" style="background:#fdecea; border-color:#e74c3c; color:#c0392b; min-width:140px;">Medical therapy</div>
</div>
</div>
<div class="flow-arrow">▼</div>
<div class="flow-box" style="background:#f5eef8; border-color:#8e44ad; color:#6c3483;">Persistent symptoms?</div>
<div class="flow-arrow">▼</div>
<div class="flow-box" style="background:#fdecea; border-color:#e74c3c; color:#c0392b;"><strong>Total Hysterectomy</strong></div>
</div>
</div>
</div>
<!-- Prognosis -->
<div class="card teal">
<h3>📈 Prognosis — Adenomyosis</h3>
<ul class="dotlist">
<li>Symptoms usually <strong>resolve after menopause</strong></li>
<li>Excellent prognosis after <strong>hysterectomy</strong></li>
<li>Medical treatment controls symptoms but <strong>recurrence common</strong> after discontinuation</li>
</ul>
</div>
<!-- ═══════════ COMPARISON TABLE ═══════════ -->
<div class="divider"></div>
<div class="keydiff">
<h3>⚡ Endometriosis vs Adenomyosis — Quick Comparison</h3>
<table style="width:100%; border-collapse:collapse; font-size:0.88rem;">
<thead>
<tr style="background:linear-gradient(90deg,#c0392b,#8e44ad); color:white;">
<th style="padding:10px 14px; text-align:left;">Feature</th>
<th style="padding:10px 14px; text-align:left;">🔴 Endometriosis</th>
<th style="padding:10px 14px; text-align:left;">🟣 Adenomyosis</th>
</tr>
</thead>
<tbody>
<tr style="background:white;">
<td style="padding:8px 14px; font-weight:600; border-bottom:1px solid #eee;">Location</td>
<td style="padding:8px 14px; border-bottom:1px solid #eee;">Outside uterus</td>
<td style="padding:8px 14px; border-bottom:1px solid #eee;">Within myometrium</td>
</tr>
<tr style="background:#fdf5f5;">
<td style="padding:8px 14px; font-weight:600; border-bottom:1px solid #eee;">Age group</td>
<td style="padding:8px 14px; border-bottom:1px solid #eee;">25–40 years</td>
<td style="padding:8px 14px; border-bottom:1px solid #eee;">35–50 years</td>
</tr>
<tr style="background:white;">
<td style="padding:8px 14px; font-weight:600; border-bottom:1px solid #eee;">Parity</td>
<td style="padding:8px 14px; border-bottom:1px solid #eee;">Nulliparous</td>
<td style="padding:8px 14px; border-bottom:1px solid #eee;">Multiparous</td>
</tr>
<tr style="background:#fdf5f5;">
<td style="padding:8px 14px; font-weight:600; border-bottom:1px solid #eee;">Main symptom</td>
<td style="padding:8px 14px; border-bottom:1px solid #eee;">Pelvic pain + infertility</td>
<td style="padding:8px 14px; border-bottom:1px solid #eee;">Menorrhagia + dysmenorrhoea</td>
</tr>
<tr style="background:white;">
<td style="padding:8px 14px; font-weight:600; border-bottom:1px solid #eee;">Uterus</td>
<td style="padding:8px 14px; border-bottom:1px solid #eee;">Fixed, retroverted</td>
<td style="padding:8px 14px; border-bottom:1px solid #eee;">Uniformly enlarged, boggy</td>
</tr>
<tr style="background:#fdf5f5;">
<td style="padding:8px 14px; font-weight:600; border-bottom:1px solid #eee;">Gold standard Dx</td>
<td style="padding:8px 14px; border-bottom:1px solid #eee;">Laparoscopy + biopsy</td>
<td style="padding:8px 14px; border-bottom:1px solid #eee;">Histopathology of hysterectomy specimen</td>
</tr>
<tr style="background:white;">
<td style="padding:8px 14px; font-weight:600; border-bottom:1px solid #eee;">Best imaging</td>
<td style="padding:8px 14px; border-bottom:1px solid #eee;">TVS (1st line), MRI (DIE)</td>
<td style="padding:8px 14px; border-bottom:1px solid #eee;">TVS (1st line), MRI (best)</td>
</tr>
<tr style="background:#fdf5f5;">
<td style="padding:8px 14px; font-weight:600; border-bottom:1px solid #eee;">Hormone</td>
<td style="padding:8px 14px; border-bottom:1px solid #eee;">Estrogen-dependent</td>
<td style="padding:8px 14px; border-bottom:1px solid #eee;">Estrogen-dependent</td>
</tr>
<tr style="background:white;">
<td style="padding:8px 14px; font-weight:600;">Definitive Rx</td>
<td style="padding:8px 14px;">Laparoscopy / Hysterectomy + BSO</td>
<td style="padding:8px 14px;">Total hysterectomy (ovaries preserved)</td>
</tr>
</tbody>
</table>
</div>
<!-- ═══════════ EXAM PEARLS ═══════════ -->
<div class="divider"></div>
<div class="card orange" style="margin-top:0;">
<h3>💎 High-Yield Exam Pearls</h3>
<div class="grid-2" style="margin-top:8px;">
<ul class="dotlist">
<li>Most common site of endometriosis → <strong>Ovary</strong></li>
<li>Most accepted theory → <strong>Sampson's (retrograde menstruation)</strong></li>
<li>Chocolate cyst = <strong>ovarian endometrioma</strong></li>
<li>Ground-glass appearance on USG = endometrioma</li>
<li>Gold standard for endometriosis = <strong>Laparoscopy + biopsy</strong></li>
<li>ASRM staging: I-Minimal, II-Mild, III-Moderate, IV-Severe</li>
<li>Stage ≠ symptom severity!</li>
<li>Medical Rx does NOT improve fertility</li>
</ul>
<ul class="dotlist">
<li>Adenomyosis = endometrium in myometrium</li>
<li>Histo criterion: glands <strong>≥2.5 mm below EMJ</strong></li>
<li>Globular, boggy, tender uterus = adenomyosis</li>
<li>MRI junctional zone <strong>>12 mm</strong> → adenomyosis</li>
<li>LNG-IUS = most effective long-term medical Rx (adenomyosis)</li>
<li>Gold standard for adenomyosis = <strong>histopathology of hysterectomy</strong></li>
<li>Both are <strong>estrogen-dependent</strong></li>
<li>Both can coexist!</li>
</ul>
</div>
</div>
<div class="footer">
📚 Dr Vivek Jog | Batch 2022–23 | Endometriosis & Adenomyosis Study Notes
</div>
</body>
</html>
ls -lh /home/daytona/workspace/endo-notes/
Endometriosis Adenomyosis Notes
HTML File · HTML
🔴 ENDOMETRIOSIS
| Topic | Key Point |
|---|---|
| Definition | Endometrial glands/stroma outside uterus |
| Peak age | 25–40 years, estrogen-dependent |
| Epidemiology | 6–10% reproductive women; 30–50% infertile women |
| Pathogenesis | Sampson's Theory (retrograde menstruation) ⭐ |
| Most common site | Ovaries |
| Classical Triad | Dysmenorrhoea + Dyspareunia + Infertility |
| USG finding | "Ground-glass" appearance = endometrioma |
| Gold standard Dx | Laparoscopy + histopathological confirmation |
| Medical Rx | NSAIDs → COCPs → Progestins → GnRH agonists |
| Key rule | Medical Rx relieves pain but does NOT improve fertility |
🟣 ADENOMYOSIS
| Topic | Key Point |
|---|---|
| Definition | Endometrial glands/stroma within myometrium |
| Peak age | 35–50 years, multiparous |
| Classic presentation | Menorrhagia + boggy/globular uterus + secondary dysmenorrhoea |
| Histology criterion | Glands ≥2.5 mm below endo-myometrial junction |
| MRI finding | Junctional zone >12 mm |
| Best long-term medical Rx | LNG-IUS ⭐ |
| Gold standard Dx | Histopathology of hysterectomy specimen |
| Definitive Rx | Total hysterectomy (ovaries preserved) |
💎 Notes features include:
- Color-coded cards (red = Endometriosis, purple = Adenomyosis)
- Flowcharts for pathogenesis and diagnostic algorithms
- Side-by-side comparison table
- Exam pearl boxes
- Treatment pill tags
- Mnemonic highlights
Is me kuch all terminology he vo simply samjao
🔴 ENDOMETRIOSIS — Terminology Simply
📖 Basic Words
| Medical Word | Simple Matlab |
|---|---|
| Endometrium | Uterus (bachi dani) ki andar ki lining — jab period aata hai toh yahi girti hai |
| Endometriosis | Yeh lining bahar nikal ke galat jagah chipak jaaye |
| Stroma | Lining ka supporting tissue (cells ke beech ka material) |
| Glands | Lining mein chhoti chhoti liquid banane wali structures |
| Myometrium | Uterus ki muscular wall (muscle layer) |
🩸 Period / Hormones Related
| Word | Simple Matlab |
|---|---|
| Menarche | Pehli baar period aana (usually 11–13 saal mein) |
| Menopause | Period hamesha ke liye band hona (usually ~50 saal mein) |
| Menorrhagia | Bahut zyada bleeding hona period mein |
| Dysmenorrhoea | Period ke time dard hona |
| Premenstrual spotting | Period se pehle thodi si bleeding aana |
| Estrogen-dependent | Yeh disease estrogen hormone ki wajah se badhti hai |
| Retrograde menstruation | Period ka khoon neeche baahir jaane ki jagah upar fallopian tube mein chala jaata hai |
😣 Pain Related Symptoms
| Word | Simple Matlab |
|---|---|
| Dyspareunia | Sex ke time dard hona |
| Deep dyspareunia | Sex ke time andar gehri jagah dard hona |
| Dyschezia | Potty (stool) pass karte waqt dard hona |
| Dysuria | Peshab karte waqt dard/jalan hona |
| Chronic pelvic pain | Pet ke neeche (pelvic area) mein lambe samay se dard rehna |
🏥 Signs (Doctor Examine Kare Toh)
| Word | Simple Matlab |
|---|---|
| Fixed retroverted uterus | Uterus peeche ki taraf muda hua ho aur hilta na ho (chipka hua) |
| Restricted uterine mobility | Uterus uski jagah se hil nahi sakta — adhesions ki wajah se |
| Adnexal mass | Ovary ya fallopian tube ke paas koi gilthi/cyst |
| Cervical motion tenderness | Cervix (uterus ka munh) hilane par dard |
| Uterosacral ligaments | Uterus ko peeche rakhne wale ligaments — jab tender ho toh endometriosis suspect karo |
🔬 Pathogenesis Words
| Word | Simple Matlab |
|---|---|
| Peritoneal cavity | Pet ke andar ka khali space (abdominal cavity) |
| Implantation | Cells ka kisi jagah chipak jaana |
| Fibrosis | Tissue ka sख्त (hard) ho jaana — scarring jaisa |
| Adhesions | Organs ka ek doosre se chipak jaana (jaise glue lagana) |
| Coelomic metaplasia | Pet ke andar ki normal cells khud badal ke endometrial cells ban jaayein |
| Lymphatic dissemination | Endometrial cells lymph vessels ke through door nikal jaayein |
| Immune dysfunction | Body ka defense system sahi kaam na kare — isiliye cells bahar bhi survive karte hain |
🖼️ Imaging Words
| Word | Simple Matlab |
|---|---|
| TVS (Transvaginal USG) | Vagina ke andar se kiya jaane wala ultrasound — zyada clear picture aata hai |
| Ground-glass appearance | USG mein cyst ke andar "dhundla/kaacha sheeshe jaisa" dikhna — endometrioma ki pehchaan |
| Endometrioma | Ovary mein endometriosis se bani cyst |
| Chocolate cyst | Endometrioma ka doosra naam — kyunki andar dark brown blood hota hai, chocolate jaisa dikhta hai 🍫 |
| DIE (Deep Infiltrating Endometriosis) | Endometriosis jo bahut gehri andar tak ghus gayi ho |
| Powder-burn lesions | Laparoscopy mein blue-black chhote dabbe dikhte hain — endometriosis ke spots |
| Frozen pelvis | Pelvic organs sab chipke hue hain — severe case |
💊 Treatment Words
| Word | Simple Matlab |
|---|---|
| NSAIDs | Dard ki common dawa (jaise ibuprofen) |
| COCPs | Combined oral contraceptive pills — period regulate karne wali goli |
| Progestins | Progesterone hormone wali dawaiyan |
| GnRH Agonists | Injection jo ovaries ko temporarily "off" kar de — period band, endometriosis shrink |
| Add-back therapy | GnRH agonist ke side effects (haddiyan kamzor hona) rokne ke liye thoda hormone wapas dena |
| Danazol | Purani dawa — male hormone jaisi, isliye side effects zyada (acne, voice change) |
| Aromatase inhibitors | Estrogen banana band karne wali dawaiyan (letrozole, anastrozole) |
| LNG-IUS | Uterus ke andar daali jaane wali device (Mirena) — progesterone release karta hai |
| IUI | Sperm directly uterus mein daalna — light infertility mein |
| IVF | Baahir lab mein fertilization karke embryo uterus mein dalna |
| Laparoscopy | Naabhi ke paas chhota sa cut karke camera andar daalke dekhna/treat karna — "keyhole surgery" |
| Adhesiolysis | Surgery mein chipke hue organs ko alag karna |
| Cystectomy | Cyst ko nikaalna |
| BSO (Bilateral Salpingo-Oophorectomy) | Dono ovaries + dono fallopian tubes nikaalna |
🟣 ADENOMYOSIS — Terminology Simply
| Word | Simple Matlab |
|---|---|
| Adenomyosis | Endometrial tissue (lining) muscle ke andar ghus gayi |
| Junctional zone | Endometrium aur myometrium ke beech ki border line |
| Globular uterus | Uterus gol aur bada ho jaana — uniformly (chaaro taraf se) |
| Boggy uterus | Uterus geela/spongy/naram feel ho touch karne par |
| Trabeculated myometrium | Muscle mein lines/bands dikhna — cut karne par pattern dikhta hai |
| Adenomyoma | Focal adenomyosis — ek jagah localized — fibroid jaisa lagta hai |
| TIAR | Tissue Injury and Repair — bar bar chot lagne se repair hote hote endometrium andar ghus jaata hai |
| Hypertrophy | Size mein bada ho jaana |
| Hyperplasia | Cells ki ginti badh jaana |
| Histopathology | Microscope se tissue examine karna |
| Basalis | Endometrium ki sabse neeche ki layer (jo period mein nahi girti) |
⚡ Ek Line Summary
Endometriosis = Uterus ki lining bahar nikal gayi → dard + infertilityAdenomyosis = Uterus ki lining andar muscle mein ghus gayi → bleeding + bada uterus
Sampson's Theory (retrograde menstruation) ⭐,Ground-glass" appearance = endometrioma,NSAIDs → COCPs → Progestins → GnRH agonists ,Menorrhagia + boggy/globular uterus + secondary dysmenorrhoea ,MRI finding Junctional zone >12 mm ,Best long-term medical Rx LNG-IUS ⭐ ,Definitive Rx Total hysterectomy (ovaries preserved) ye sab samaj nai aya
1️⃣ Sampson's Theory (Retrograde Menstruation) ⭐
🩸 Normal Period kya hota hai?
Period mein uterus ki lining neeche ki taraf — vagina se bahar nikalti hai.
😮 Retrograde = Ulta!
Kuch aurat mein thodi si lining upar ki taraf — Fallopian tube se hote hue pet ke andar (peritoneal cavity) mein chali jaati hai.
Normal: Uterus → Vagina → Baahir ✅
Retrograde: Uterus → Fallopian Tube → Pet ke andar ❌
🦠 Phir kya hota hai?
Lining ke cells pet mein girte hain
↓
Wahan chipak jaate hain (implantation)
↓
Har period pe wahan bhi bleeding hoti hai
↓
Soojan (inflammation) hoti hai
↓
Dheere dheere sख्त ho jaata hai (fibrosis + adhesions)
↓
= ENDOMETRIOSIS 😰
❓ Toh phir sabko endometriosis kyun nahi hota?
Kyunki normal immune system in cells ko maar deta hai. Jis aurat ki immunity kamzor ho — cells survive kar lete hain = Endometriosis!
2️⃣ "Ground-Glass" Appearance = Endometrioma
🍫 Pehle samjho — Chocolate Cyst kya hai?
Ovary mein endometriosis ki wajah se ek cyst (thaili) banti hai. Isme har month thodi bleeding hoti hai. Yeh blood bahar nahi nikal sakta — andar hi jamta rehta hai. Purana jamaa hua blood → dark brown, thick liquid banta hai — exactly chocolate jaisa 🍫
🖥️ Ultrasound mein kya dikhta hai?
Jab USG machine se dekhte hain toh cyst ke andar ka liquid hota hai:
- Clear liquid hota toh kala (anechoic) dikhta
- Yahan thick, gaadhaa, dark brown liquid hai
- Toh screen par dhundhla, kaacha sheeshe jaisa dikhta hai
🪟 Ground-Glass ka matlab:
Socho ek frosted/kaacha sheeshe ki khidki — Us par light padti hai toh na bilkul saaf, na bilkul kala — beech ka dhundhlaahat! Exactly waisa hi USG screen par dikhta hai → "Ground-Glass Appearance" ✅
Saaf paani wali cyst = Kali dikhti hai (anechoic)
Chocolate cyst = Dhundhli dikhti hai = GROUND GLASS ⭐
3️⃣ NSAIDs → COCPs → Progestins → GnRH Agonists
Yeh ek ladder (seedhi) hai — pehle simple dawa, phir strong 💊
Jaise Ibuprofen, Mefenamic acid Sirf dard kam karna — soojan kam karna Sabse safe, sabse asan 👉 "Dard hai toh pehle yeh lo"
Goli jisme estrogen + progesterone dono hote hain Yeh period ko control karti hai Endometriosis estrogen se badhta hai → goli se estrogen control = bimari control 👉 "Dard relief nahi? Ab hormone goli shuru karo"
Jaise Dienogest, Norethisterone Yeh endometriosis ke spots ko sukhate hain COCPs se zyada targeted 👉 "COCPs se relief nahi mila? Toh sirf progesterone wali dawa do"
Jaise Leuprolide injection Yeh brain ko signal deta hai → "Ovary band karo!" Ovary band → Estrogen zero → Endometriosis shrink ho jaata hai Basically artificial menopause create karta hai temporarily ⚠️ Side effect: Haddiyan kamzor, hot flushes Isliye 6 mahine se zyada nahi dete 👉 "Sabse badi gun — serious cases mein"
Dard sirf → NSAIDs
Hormone help → COCPs
Progesterone → Progestins
Sabse strong → GnRH Agonists
4️⃣ Menorrhagia + Boggy/Globular Uterus + Secondary Dysmenorrhoea
Yeh teen cheezein milke Adenomyosis ki pehchaan hain 🟣
Normal period mein 3–5 din, normal amount Adenomyosis mein uterus ki muscle ke andar endometrial tissue hoti hai Har period pe bahar bhi + andar muscle mein bhi bleeding hoti hai Result = Bahut zyada khoon = Menorrhagia
Globular = Uterus gol aur bada ho gaya — chaaro taraf se equally (fibroid mein ek taraf zyada bada hota — adenomyosis mein uniform) Boggy = Touch karo toh spongy/naram/geela lagta hai (normal uterus firm hota hai — yeh soft feel hota hai) 👉 Socho ek bheega sponge — dabaane par squish karta hai = Boggy!
Primary dysmenorrhoea = Pehle se hi period mein dard — koi bimari nahi, normal Secondary dysmenorrhoea = Pehle dard nahi tha, baad mein shuru hua — koi disease ki wajah se Adenomyosis mein muscle ke andar tissue hai → bleeding → muscle mein pressure → dard Aur yeh dard time ke saath badta jaata hai (progressive)
5️⃣ MRI Mein Junctional Zone > 12 mm
🧱 Junctional Zone kya hai?
[Endometrium - andar ki lining ]
━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━━ ← Yeh hai JUNCTIONAL ZONE (border)
[Myometrium - muscle layer ]
Endometrium aur Muscle ke beech ek border/dividing line hoti hai. MRI par yeh dark line ki tarah dikhti hai.
📏 Normal vs Adenomyosis
Normal = Yeh border ki thickness 8 mm se kam hoti hai Adenomyosis = Endometrial tissue muscle mein ghus jaata hai → border moti aur irregular ho jaati hai > 12 mm = Adenomyosis confirm ✅
🤔 Simple Example:
Socho ek wall aur floor ke beech grout line (cement line) hoti hai. Normal = Patli, clean line Adenomyosis = Grout phail gaya, mota ho gaya, irregular — matlab dono mein mixing ho gayi!
6️⃣ LNG-IUS = Best Long-Term Medical Treatment ⭐
LNG-IUS kya hai?
Levonorgestrel Intrauterine System Popular name = Mirena Ek chhota T-shaped plastic device jo uterus ke andar daala jaata hai
|
_|_
| | ← Yeh T-shape hai
|___|
Yeh kaam kaise karta hai?
Iske andar Levonorgestrel (progesterone type hormone) bhara hota hai Dheere dheere 5 saal tak hormone release karta rehta hai Direct uterus mein → Lining patli ho jaati hai → Bleeding kam → Dard kam
Adenomyosis mein kyun best hai?
✅ Local action — sirf uterus pe, body mein side effects kam ✅ 5 saal tak kaam karta hai — bar bar dawa nahi ✅ Bleeding 80–90% tak kam kar deta hai ✅ Dard bhi kam karta hai ✅ Fertility preserve hoti hai
7️⃣ Definitive Rx = Total Hysterectomy (Ovaries Preserved)
Matlab seedha seedha:
| Word | Matlab |
|---|---|
| Definitive Rx | Permanent/final treatment — bimari dobara nahi aayegi |
| Total Hysterectomy | Poora uterus nikaalna (cervix sameto) |
| Ovaries preserved | Ovaries nahi nikalte — woh wahi rehti hain |
❓ Ovaries kyun nahi nikalte?
Adenomyosis uterus ki bimari hai — ovaries theek hain Ovaries nikalte toh = surgical menopause (sudden) → Hot flushes, haddi kamzor (osteoporosis), heart problems Isliye → Sirf uterus nikalo, ovaries rehne do ✅
Compare karo Endometriosis se:
| Adenomyosis | Endometriosis (severe) | |
|---|---|---|
| Uterus | Nikalta hai | Nikalta hai |
| Ovaries | Rehti hain ✅ | BSO (nikal bhi sakte hain) |
| Kyun? | Bimari sirf uterus mein | Ovaries pe bhi endometriosis ho sakta |
🎯 Ek Line Mein Yaad Karo
🔴 Sampson = Period ulta gaya → Pet mein chipka → Endometriosis 🍫 Ground glass = Chocolate cyst ka USG look = dhundhlaahat 💊 NSAIDs→COCPs→Progestins→GnRH = Dawa ki seedhi (simple se strong) 🟣 Menorrhagia + Boggy uterus + Secondary dysmenorrhoea = Adenomyosis ki pehchaan 📏 JZ > 12mm = MRI mein adenomyosis 🏆 LNG-IUS = Adenomyosis ka best lambi chalne wali dawa 🔪 Hysterectomy = Uterus nikalo, Ovaries rehne do (Adenomyosis mein)
Find latest clinical images showing chocolate cysts and junctional zone changes
chocolate cyst endometrioma ultrasound ground glass appearance clinical image
adenomyosis junctional zone thickening MRI clinical image radiology
endometrioma chocolate cyst gross pathology surgical laparoscopy image
🍫 IMAGE 1 — Chocolate Cyst (Endometrioma) on Ultrasound
"Ground-Glass" Appearance — USG
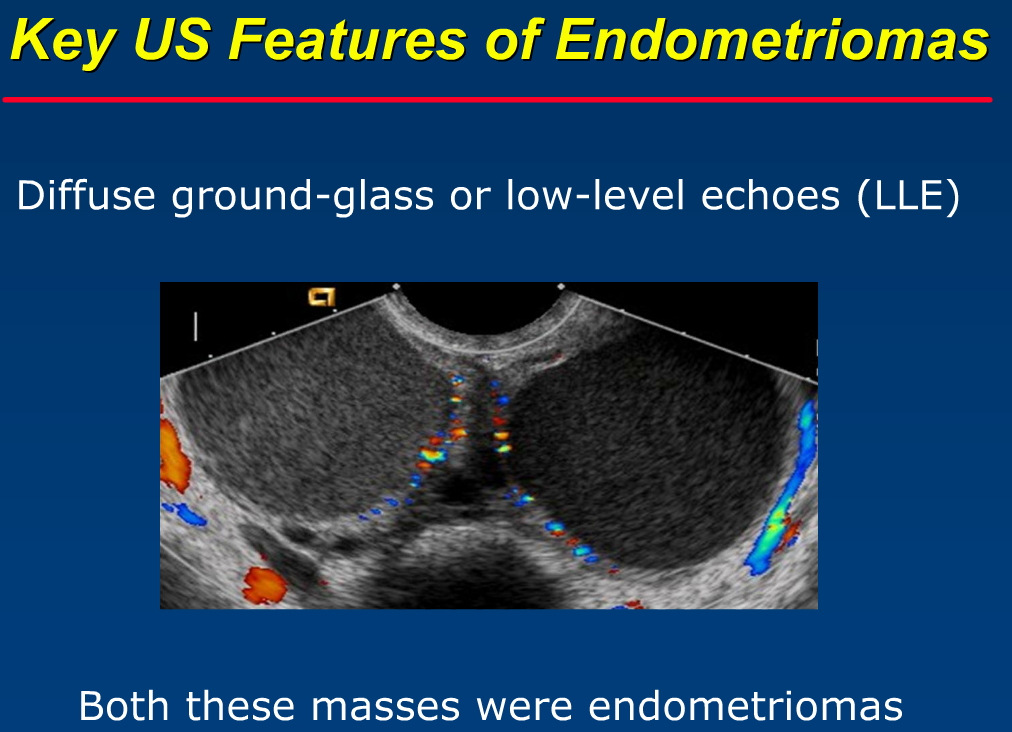
- Screen par dono taraf gol, dhundhli cysts hain — yeh dono endometriomas hain
- Andar ka content na bilkul kala, na bilkul saaf — yeh "ground-glass / low-level echoes" hai
- Thick wall clearly visible hai
- Yahi classic chocolate cyst ka ultrasound look hai ✅
🔬 IMAGE 2 — Laparoscopy mein Chocolate Cyst (Actual surgical view)
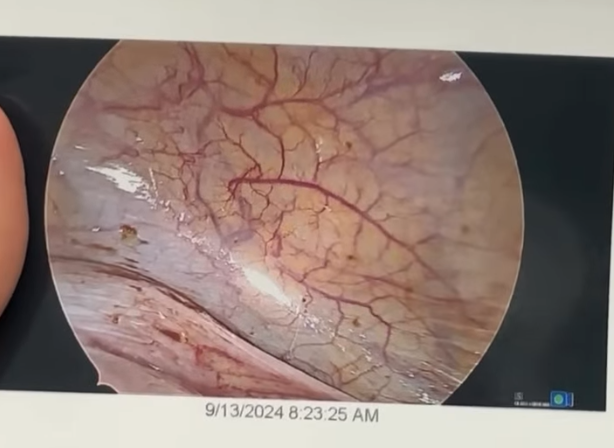
- Yeh laparoscopy camera se andar ka actual view hai (September 2024 ka real case)
- Ovary par ek badi chocolate-brown/dark cyst clearly dikh rahi hai
- Surface par blood vessels visible hain
- Yahi woh cyst hai jiske andar dark brown thick fluid (purana khoon) hota hai
- Surgeon yahi dekhkar confirm karta hai = Endometrioma ✅
🧲 IMAGE 3 — Junctional Zone Thickening on MRI (Adenomyosis)
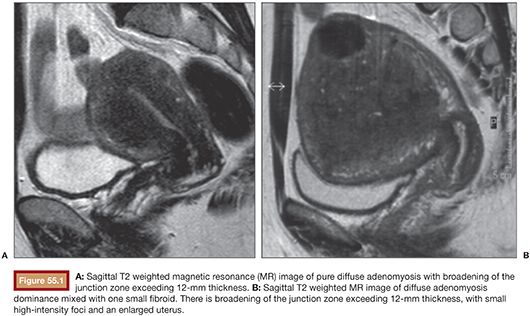
- A (baayaan image): Sagittal T2 MRI — Uterus ki muscle mein dark, ill-defined thickening clearly visible — yeh hai Junctional Zone > 12mm = Adenomyosis confirmed
- B (daayaan image): Dono images mein uterus bada aur globular ho gaya hai
- Dark area = muscle mein endometrial tissue ghus gayi hai (smooth muscle hyperplasia)
- Bright foci = andar chhoti chhoti bleeding ke spots
📊 IMAGE 4 — Normal vs Adenomyosis JZ (Side by side comparison)

| Image | Matlab |
|---|---|
| a & b | Normal JZ — thin, clean, well-defined dark line around endometrium |
| c | Adenomyosis — JZ moti, irregular, ill-defined ho gayi (red arrow = ectopic endometrial tissue) |
| d | Normal uterine zonal anatomy for reference |
🔑 Key point: JZ 8-12mm = "gray zone" (recheck needed) | JZ >12mm = Adenomyosis confirmed ✅
🏥 IMAGE 5 — Diffuse Adenomyosis on MRI (Confirmed Cases)

- A: Sagittal MRI — bada uterus, JZ thickening with ill-defined mass (black arrow) = focal adenomyosis
- B: Coronal view — uterus deformed, anterior wall hypertrophied = diffuse adenomyosis
- Star (★) = vagina for orientation
🎯 Summary — Images se kya seekha
| Finding | Image Type | Kya dikhta hai |
|---|---|---|
| 🍫 Chocolate cyst | USG | Dhundhli (ground-glass), thick-walled cyst |
| 🔪 Chocolate cyst | Laparoscopy | Dark brown cyst on ovary (actual view) |
| 🧲 JZ thickening | MRI T2 | Dark thick band around endometrium |
| 📏 JZ > 12mm | MRI | Ill-defined dark zone = Adenomyosis |
| 🔴 Ectopic tissue | MRI | Bright spots (red arrow) in muscle |
Generate visual diagnostic flowchart for endometriosis vs adenomyosis
A detailed medical diagnostic flowchart comparing Endometriosis vs Adenomyosis. The flowchart starts at the top with "Woman with Chronic Pelvic Pain / Menstrual Symptoms" in a central box, then splits into two parallel diagnostic pathways side by side. Left pathway in red theme for Endometriosis, right pathway in purple theme for Adenomyosis. Each pathway shows: key symptoms (dysmenorrhea, dyspareunia, infertility for endometriosis; menorrhagia, boggy uterus, secondary dysmenorrhea for adenomyosis), clinical signs, investigations (TVS ultrasound findings, MRI findings), gold standard diagnosis, and treatment options (medical and surgical). Include labeled boxes with icons, arrows connecting steps, color-coded sections, clear typography. At the bottom a comparison summary table. Clean clinical infographic style on white background.
~/endo-notes/Diagnostic_Flowchart.html
<!DOCTYPE html>
<html lang="en">
<head>
<meta charset="UTF-8">
<meta name="viewport" content="width=device-width, initial-scale=1.0">
<title>Diagnostic Flowchart — Endometriosis vs Adenomyosis</title>
<style>
@import url('https://fonts.googleapis.com/css2?family=Inter:wght@400;600;700;800&display=swap');
* { box-sizing: border-box; margin: 0; padding: 0; }
body { font-family: 'Inter', sans-serif; background: #f0f4f8; padding: 20px; color: #1a202c; }
.page-title {
text-align: center;
background: linear-gradient(135deg, #c0392b, #6c3483);
color: white;
border-radius: 16px;
padding: 28px 20px;
margin-bottom: 28px;
box-shadow: 0 8px 30px rgba(0,0,0,0.2);
}
.page-title h1 { font-size: 2rem; font-weight: 800; }
.page-title p { font-size: 0.95rem; opacity: 0.85; margin-top: 6px; }
/* START BOX */
.start-box {
background: linear-gradient(135deg, #2c3e50, #34495e);
color: white;
border-radius: 50px;
padding: 16px 32px;
text-align: center;
font-size: 1.1rem;
font-weight: 700;
max-width: 600px;
margin: 0 auto 10px;
box-shadow: 0 4px 16px rgba(0,0,0,0.2);
}
/* ARROW */
.arrow-down {
text-align: center;
font-size: 2rem;
color: #7f8c8d;
line-height: 1;
margin: 4px 0;
}
/* QUESTION BOX */
.question-box {
background: white;
border: 3px solid #3498db;
border-radius: 14px;
padding: 14px 20px;
text-align: center;
font-size: 1rem;
font-weight: 700;
color: #1a5276;
max-width: 500px;
margin: 0 auto 6px;
box-shadow: 0 2px 10px rgba(0,0,0,0.08);
}
/* TWO COLUMN SPLIT */
.split {
display: grid;
grid-template-columns: 1fr 40px 1fr;
gap: 0;
align-items: start;
margin: 10px 0;
}
.split-divider {
display: flex;
flex-direction: column;
align-items: center;
justify-content: flex-start;
padding-top: 30px;
color: #bbb;
font-size: 1.8rem;
font-weight: 700;
}
/* PATHWAY HEADER */
.path-header {
border-radius: 14px 14px 0 0;
padding: 14px 18px;
text-align: center;
font-size: 1.15rem;
font-weight: 800;
color: white;
}
.endo-hdr { background: linear-gradient(135deg, #c0392b, #e74c3c); }
.adeno-hdr { background: linear-gradient(135deg, #6c3483, #8e44ad); }
/* STEP BOX */
.step {
border-radius: 10px;
padding: 12px 16px;
margin-bottom: 4px;
font-size: 0.87rem;
}
.step-label {
font-size: 0.75rem;
font-weight: 700;
text-transform: uppercase;
letter-spacing: 0.05em;
margin-bottom: 6px;
display: block;
}
.step ul { padding-left: 16px; }
.step ul li { margin-bottom: 3px; }
.step strong { font-weight: 700; }
/* ENDO steps */
.e-symptoms { background: #fdecea; border-left: 4px solid #e74c3c; }
.e-signs { background: #fef9e7; border-left: 4px solid #f39c12; }
.e-usg { background: #eaf4fc; border-left: 4px solid #2980b9; }
.e-mri { background: #eaf4fc; border-left: 4px solid #1a5276; }
.e-gold { background: #e8f8f5; border-left: 4px solid #16a085; }
.e-medical { background: #fef5e7; border-left: 4px solid #e67e22; }
.e-surgical { background: #f9ebea; border-left: 4px solid #c0392b; }
/* ADENO steps */
.a-symptoms { background: #f5eef8; border-left: 4px solid #8e44ad; }
.a-signs { background: #fef9e7; border-left: 4px solid #d4ac0d; }
.a-usg { background: #eaf4fc; border-left: 4px solid #2e86c1; }
.a-mri { background: #eaf4fc; border-left: 4px solid #1b4f72; }
.a-gold { background: #e8f8f5; border-left: 4px solid #0e6655; }
.a-medical { background: #f4ecf7; border-left: 4px solid #7d3c98; }
.a-surgical { background: #f5eef8; border-left: 4px solid #6c3483; }
.step-label.red { color: #c0392b; }
.step-label.orange { color: #d35400; }
.step-label.blue { color: #1a5276; }
.step-label.teal { color: #0e6655; }
.step-label.purple { color: #6c3483; }
.step-label.gold { color: #9a7d0a; }
/* COLUMN WRAPPER */
.col-wrap {
border-radius: 14px;
overflow: hidden;
box-shadow: 0 4px 16px rgba(0,0,0,0.1);
}
.col-body { background: white; padding: 10px; display: flex; flex-direction: column; gap: 5px; }
/* BADGE */
.badge {
display: inline-block;
border-radius: 50px;
padding: 3px 10px;
font-size: 0.75rem;
font-weight: 700;
margin-right: 4px;
margin-bottom: 2px;
}
.b-red { background: #fdecea; color: #c0392b; border: 1.5px solid #e74c3c; }
.b-purple { background: #f5eef8; color: #6c3483; border: 1.5px solid #8e44ad; }
.b-green { background: #e8f8f5; color: #0e6655; border: 1.5px solid #16a085; }
.b-blue { background: #eaf4fc; color: #1a5276; border: 1.5px solid #2980b9; }
.b-orange { background: #fef5e7; color: #935116; border: 1.5px solid #e67e22; }
/* ARROW between steps inside column */
.step-arrow { text-align: center; color: #bbb; font-size: 1.2rem; margin: 1px 0; }
/* COMPARISON TABLE */
.compare-section {
margin-top: 24px;
background: white;
border-radius: 16px;
overflow: hidden;
box-shadow: 0 4px 16px rgba(0,0,0,0.1);
}
.compare-section .cmp-header {
background: linear-gradient(90deg, #c0392b, #6c3483);
color: white;
text-align: center;
padding: 14px;
font-size: 1.1rem;
font-weight: 800;
}
table.cmp-table { width: 100%; border-collapse: collapse; }
table.cmp-table th { padding: 10px 14px; font-size: 0.85rem; }
table.cmp-table td { padding: 9px 14px; font-size: 0.84rem; border-bottom: 1px solid #f0f0f0; }
table.cmp-table .th-feat { background: #f0f4f8; color: #2c3e50; font-weight: 700; }
table.cmp-table .th-endo { background: #fdecea; color: #c0392b; font-weight: 700; }
table.cmp-table .th-adeno{ background: #f5eef8; color: #6c3483; font-weight: 700; }
table.cmp-table tr:nth-child(even) td { background: #fafafa; }
table.cmp-table .feat-cell { font-weight: 600; color: #555; }
/* EXAM PEARLS */
.pearls {
margin-top: 20px;
background: linear-gradient(135deg, #fef9e7, #fdecea);
border-radius: 14px;
padding: 20px 24px;
border: 2px dashed #e67e22;
}
.pearls h3 { font-size: 1.05rem; font-weight: 800; color: #935116; margin-bottom: 12px; }
.pearls-grid { display: grid; grid-template-columns: 1fr 1fr; gap: 8px; }
.pearl-item {
background: white;
border-radius: 8px;
padding: 8px 12px;
font-size: 0.83rem;
display: flex;
align-items: flex-start;
gap: 8px;
box-shadow: 0 1px 4px rgba(0,0,0,0.07);
}
.pearl-item .pi { font-size: 1.1rem; flex-shrink: 0; }
@media(max-width: 700px) {
.split { grid-template-columns: 1fr; }
.split-divider { display: none; }
.pearls-grid { grid-template-columns: 1fr; }
}
</style>
</head>
<body>
<!-- TITLE -->
<div class="page-title">
<h1>🩺 Diagnostic Flowchart</h1>
<p>Endometriosis 🔴 vs Adenomyosis 🟣 — Step-by-step Clinical Approach</p>
</div>
<!-- START -->
<div class="start-box">👩 Woman presenting with Pelvic Pain / Menstrual Complaints</div>
<div class="arrow-down">▼</div>
<!-- HISTORY QUESTION -->
<div class="question-box">🗣️ Take Detailed History — When did pain start? Menstrual pattern? Fertility issues?</div>
<div class="arrow-down">▼</div>
<!-- SPLIT into two pathways -->
<div class="split">
<!-- ═══ ENDOMETRIOSIS ═══ -->
<div class="col-wrap">
<div class="path-header endo-hdr">🔴 ENDOMETRIOSIS PATHWAY</div>
<div class="col-body">
<!-- Symptoms -->
<div class="step e-symptoms">
<span class="step-label red">🤒 Symptoms to look for</span>
<ul>
<li><strong>Progressive dysmenorrhoea</strong> (worsening over years)</li>
<li>Deep <strong>dyspareunia</strong> (sex mein dard)</li>
<li>Chronic <strong>pelvic pain</strong></li>
<li><strong>Infertility / subfertility</strong></li>
<li>Dyschezia (potty mein dard)</li>
<li>Dysuria (bladder involved)</li>
</ul>
<div style="margin-top:8px;">
<span class="badge b-red">Age: 25–40 yrs</span>
<span class="badge b-red">Nulliparous</span>
</div>
</div>
<div class="step-arrow">▼</div>
<!-- Signs -->
<div class="step e-signs">
<span class="step-label orange">🩺 Examination Signs</span>
<ul>
<li>Fixed <strong>retroverted uterus</strong></li>
<li>Restricted uterine mobility</li>
<li>Tender nodules in uterosacral ligaments</li>
<li><strong>Adnexal mass</strong> (endometrioma)</li>
<li>Cervical motion tenderness</li>
</ul>
</div>
<div class="step-arrow">▼</div>
<!-- TVS -->
<div class="step e-usg">
<span class="step-label blue">🖥️ TVS (First-line Imaging)</span>
<ul>
<li>Ovarian cyst: <strong>"Ground-glass"</strong> appearance</li>
<li>Unilocular, thick wall, ↓ vascularity</li>
<li>= <strong>Chocolate cyst / Endometrioma</strong> 🍫</li>
</ul>
</div>
<div class="step-arrow">▼</div>
<!-- MRI -->
<div class="step e-mri">
<span class="step-label blue">🧲 MRI (if DIE suspected)</span>
<ul>
<li>Deep infiltrating endometriosis mapping</li>
<li>Bowel / bladder / ureteric involvement</li>
<li>Pre-operative planning</li>
</ul>
</div>
<div class="step-arrow">▼</div>
<!-- Gold Standard -->
<div class="step e-gold">
<span class="step-label teal">🏆 Gold Standard Diagnosis</span>
<div style="font-size:0.92rem; font-weight:700; color:#0e6655;">
Laparoscopy + Histopathological Confirmation
</div>
<ul style="margin-top:6px;">
<li>Powder-burn (blue-black) lesions</li>
<li>Chocolate cyst</li>
<li>Dense adhesions / Frozen pelvis</li>
</ul>
</div>
<div class="step-arrow">▼</div>
<!-- Medical Rx -->
<div class="step e-medical">
<span class="step-label orange">💊 Medical Treatment</span>
<div style="display:flex; flex-wrap:wrap; gap:4px;">
<span class="badge b-orange">NSAIDs</span>
<span class="badge b-orange">COCPs</span>
<span class="badge b-orange">Progestins</span>
<span class="badge b-orange">LNG-IUS</span>
<span class="badge b-orange">GnRH Agonists</span>
<span class="badge b-blue">Danazol (2nd line)</span>
</div>
<div style="font-size:0.78rem; color:#c0392b; margin-top:6px; font-weight:600;">
⚠️ Does NOT improve fertility!
</div>
</div>
<div class="step-arrow">▼</div>
<!-- Surgical Rx -->
<div class="step e-surgical">
<span class="step-label red">🔪 Surgical Treatment</span>
<div style="font-weight:600; margin-bottom:4px;">Conservative (Laparoscopy):</div>
<ul>
<li>Excision of implants</li>
<li>Adhesiolysis</li>
<li>Ovarian cystectomy</li>
</ul>
<div style="font-weight:600; margin-top:6px; margin-bottom:4px;">Definitive:</div>
<ul>
<li>Hysterectomy + BSO</li>
<li>For completed family / recurrent disease</li>
</ul>
</div>
</div>
</div>
<!-- DIVIDER -->
<div class="split-divider">VS</div>
<!-- ═══ ADENOMYOSIS ═══ -->
<div class="col-wrap">
<div class="path-header adeno-hdr">🟣 ADENOMYOSIS PATHWAY</div>
<div class="col-body">
<!-- Symptoms -->
<div class="step a-symptoms">
<span class="step-label purple">🤒 Symptoms to look for</span>
<ul>
<li><strong>Menorrhagia</strong> — most common symptom</li>
<li>Progressive <strong>secondary dysmenorrhoea</strong></li>
<li>Chronic <strong>pelvic pain</strong></li>
<li>Dyspareunia</li>
<li>Subfertility (less common)</li>
</ul>
<div style="margin-top:8px;">
<span class="badge b-purple">Age: 35–50 yrs</span>
<span class="badge b-purple">Multiparous</span>
</div>
</div>
<div class="step-arrow">▼</div>
<!-- Signs -->
<div class="step a-signs">
<span class="step-label gold">🩺 Examination Signs</span>
<ul>
<li>Uniformly <strong>enlarged</strong> uterus</li>
<li><strong>Globular</strong> uterus shape</li>
<li><strong>Boggy</strong> (soft/spongy) consistency</li>
<li><strong>Tender</strong> uterus</li>
</ul>
<div style="font-size:0.78rem; color:#7d3c98; font-weight:600; margin-top:5px;">
💡 Boggy + Globular + Tender = Suspect Adenomyosis!
</div>
</div>
<div class="step-arrow">▼</div>
<!-- TVS -->
<div class="step a-usg">
<span class="step-label blue">🖥️ TVS (First-line Imaging)</span>
<ul>
<li>Globular uterus</li>
<li>Asymmetric myometrial thickening</li>
<li>Heterogeneous myometrium</li>
<li>Myometrial cysts</li>
<li>Fan-shaped shadowing</li>
<li>Indistinct endo-myometrial junction</li>
</ul>
</div>
<div class="step-arrow">▼</div>
<!-- MRI -->
<div class="step a-mri">
<span class="step-label blue">🧲 MRI (Best Imaging)</span>
<ul>
<li><strong>Junctional zone > 12 mm</strong> = diagnostic ✅</li>
<li>Myometrial cysts (bright foci on T2)</li>
<li>Diffuse or focal adenomyosis</li>
<li>JZ 8–12mm = "gray zone" (recheck needed)</li>
</ul>
</div>
<div class="step-arrow">▼</div>
<!-- Gold Standard -->
<div class="step a-gold">
<span class="step-label teal">🏆 Gold Standard Diagnosis</span>
<div style="font-size:0.92rem; font-weight:700; color:#0e6655;">
Histopathology of Hysterectomy Specimen
</div>
<ul style="margin-top:6px;">
<li>Glands ≥2.5 mm below endo-myometrial junction</li>
<li>Smooth muscle hyperplasia around glands</li>
</ul>
</div>
<div class="step-arrow">▼</div>
<!-- Medical Rx -->
<div class="step a-medical">
<span class="step-label purple">💊 Medical Treatment</span>
<div style="display:flex; flex-wrap:wrap; gap:4px;">
<span class="badge b-purple">NSAIDs</span>
<span class="badge b-purple">Tranexamic acid</span>
<span class="badge b-purple">COCPs</span>
<span class="badge b-purple">Progestins</span>
<span class="badge b-green">LNG-IUS ⭐ Best</span>
<span class="badge b-purple">GnRH Agonists (max 6mo)</span>
</div>
<div style="font-size:0.78rem; color:#6c3483; margin-top:6px; font-weight:600;">
⭐ LNG-IUS = Most effective long-term medical Rx
</div>
</div>
<div class="step-arrow">▼</div>
<!-- Surgical Rx -->
<div class="step a-surgical">
<span class="step-label purple">🔪 Surgical Treatment</span>
<div style="font-weight:600; margin-bottom:4px;">Conservative:</div>
<ul>
<li>Adenomyomectomy (focal)</li>
<li>Endometrial ablation</li>
<li>Uterine artery embolization</li>
</ul>
<div style="font-weight:600; margin-top:6px; margin-bottom:4px;">Definitive:</div>
<ul>
<li><strong>Total hysterectomy</strong></li>
<li>Ovaries <strong>preserved</strong> ✅</li>
<li>For completed family / failed medical Rx</li>
</ul>
</div>
</div>
</div>
</div>
<!-- COMPARISON TABLE -->
<div class="compare-section">
<div class="cmp-header">⚡ Side-by-Side Comparison</div>
<table class="cmp-table">
<thead>
<tr>
<th class="th-feat">Feature</th>
<th class="th-endo">🔴 Endometriosis</th>
<th class="th-adeno">🟣 Adenomyosis</th>
</tr>
</thead>
<tbody>
<tr><td class="feat-cell">📍 Location</td><td>Outside uterus</td><td>Within myometrium</td></tr>
<tr><td class="feat-cell">👩 Age</td><td>25–40 years</td><td>35–50 years</td></tr>
<tr><td class="feat-cell">🤱 Parity</td><td>Nulliparous</td><td>Multiparous</td></tr>
<tr><td class="feat-cell">🩸 Main symptom</td><td>Pain + Infertility</td><td>Menorrhagia + Pain</td></tr>
<tr><td class="feat-cell">🫃 Uterus</td><td>Fixed, retroverted</td><td>Globular, boggy, enlarged</td></tr>
<tr><td class="feat-cell">🖥️ TVS finding</td><td>Ground-glass cyst (endometrioma)</td><td>Heterogeneous myometrium, cysts</td></tr>
<tr><td class="feat-cell">🧲 MRI finding</td><td>Deep lesions mapping</td><td>JZ > 12 mm ⭐</td></tr>
<tr><td class="feat-cell">🏆 Gold standard</td><td>Laparoscopy + biopsy</td><td>Histopathology of hysterectomy</td></tr>
<tr><td class="feat-cell">💊 Best medical Rx</td><td>COCPs / GnRH agonists</td><td>LNG-IUS ⭐</td></tr>
<tr><td class="feat-cell">🔪 Definitive surgery</td><td>Hysterectomy + BSO</td><td>Total hysterectomy (ovaries preserved)</td></tr>
<tr><td class="feat-cell">🔬 Hormone dependence</td><td>Estrogen-dependent</td><td>Estrogen-dependent</td></tr>
</tbody>
</table>
</div>
<!-- EXAM PEARLS -->
<div class="pearls">
<h3>💎 High-Yield Exam Pearls</h3>
<div class="pearls-grid">
<div class="pearl-item"><span class="pi">⭐</span><span>Most common site of endometriosis = <strong>Ovary</strong></span></div>
<div class="pearl-item"><span class="pi">🍫</span><span>Chocolate cyst = Ovarian endometrioma (dark brown old blood)</span></div>
<div class="pearl-item"><span class="pi">🪟</span><span>Ground-glass USG = thick, old blood in cyst = endometrioma</span></div>
<div class="pearl-item"><span class="pi">📐</span><span>JZ > 12mm on MRI = Adenomyosis confirmed</span></div>
<div class="pearl-item"><span class="pi">🔪</span><span>Endo gold standard = Laparoscopy + biopsy</span></div>
<div class="pearl-item"><span class="pi">🏥</span><span>Adeno gold standard = Histopathology of hysterectomy</span></div>
<div class="pearl-item"><span class="pi">⚠️</span><span>Medical Rx in endometriosis does NOT improve fertility</span></div>
<div class="pearl-item"><span class="pi">💡</span><span>ASRM staging does NOT correlate with symptom severity</span></div>
<div class="pearl-item"><span class="pi">🔴🟣</span><span>Both are estrogen-dependent — can coexist!</span></div>
<div class="pearl-item"><span class="pi">🤱</span><span>Endo = nulliparous | Adeno = multiparous (opposite parity!)</span></div>
</div>
</div>
<div style="text-align:center; color:#aaa; font-size:0.8rem; margin-top:20px; padding:10px;">
📚 Dr Vivek Jog | Batch 2022–23 | Endometriosis & Adenomyosis Diagnostic Flowchart
</div>
</body>
</html>
📥 Download karo
Diagnostic Flowchart
HTML File · HTML
Flowchart mein kya hai — Summary
👩 Patient presents
▼
🗣️ History lena
▼
┌───────────┬───────────┐
🔴 ENDO VS 🟣 ADENO
│ │
🤒 Symptoms 🤒 Symptoms
(Pain+Infertility) (Bleeding+Pain)
│ │
🩺 Signs 🩺 Signs
(Fixed uterus) (Boggy uterus)
│ │
🖥️ TVS 🖥️ TVS
(Ground-glass cyst) (Heterogeneous)
│ │
🧲 MRI 🧲 MRI
(DIE mapping) (JZ > 12mm ⭐)
│ │
🏆 GOLD STD 🏆 GOLD STD
(Laparoscopy) (Histopathology)
│ │
💊 Medical 💊 Medical
(NSAIDs→GnRH) (LNG-IUS ⭐)
│ │
🔪 Surgical 🔪 Surgical
(Lap/Hysterectomy) (Hysterectomy,
Ovaries saved!)