Pyogenic meningitis microbiology
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Finding Sources
Loading Image
Reading File
Reading File
I now have comprehensive information from multiple authoritative sources. Let me compile the full answer.
Pyogenic Meningitis - Microbiology
Pyogenic (acute bacterial) meningitis is inflammation of the arachnoid membrane, pia mater, and the CSF within the subarachnoid space, caused by bacteria that evoke a polymorphonuclear (neutrophilic) response in the CSF.
Gross Pathology
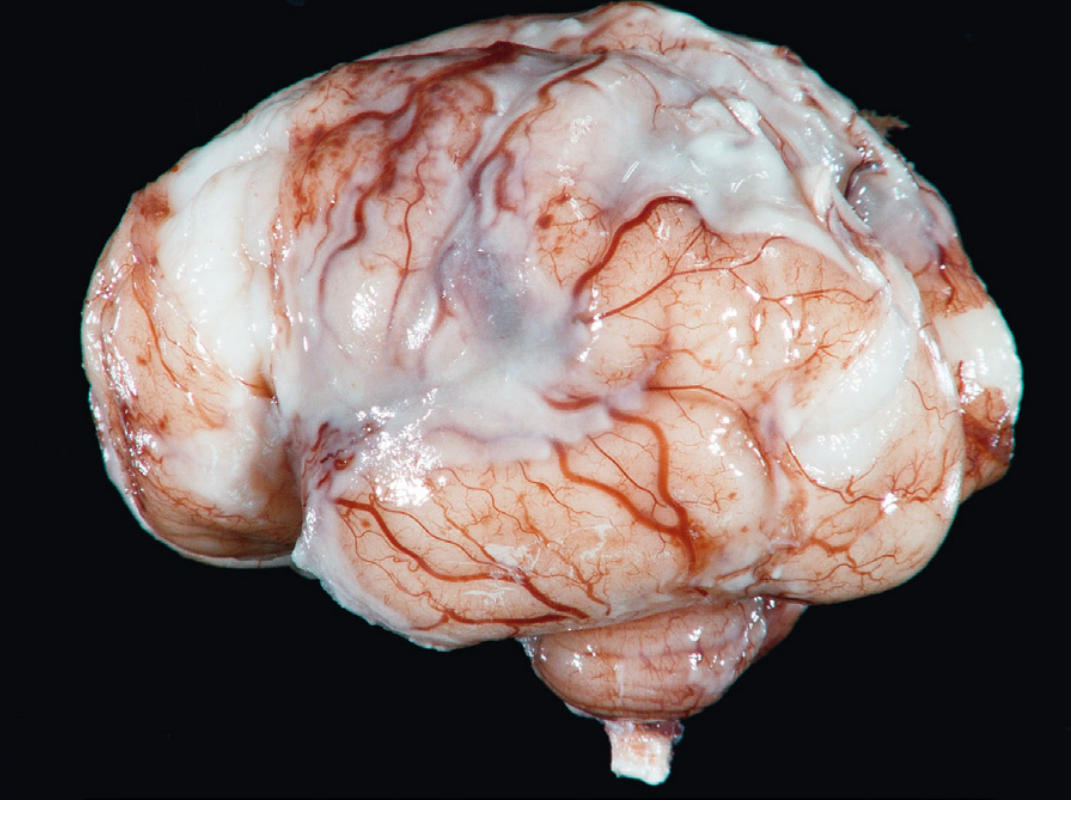
Fig. Pyogenic meningitis: A thick layer of suppurative (purulent) exudate covers the brain surface and thickens the leptomeninges. The meningeal vessels are engorged and prominent. - Robbins & Cotran Pathologic Basis of Disease, p. 1164
Causative Organisms by Age Group
The most likely pathogen is strongly determined by the patient's age:
| Age Group | Predominant Organisms |
|---|---|
| Neonates (< 1 month) | Escherichia coli, Group B Streptococcus (GBS, S. agalactiae) |
| Infants / Children | Neisseria meningitidis, Haemophilus influenzae type b (Hib) |
| Adolescents / Young adults | Neisseria meningitidis |
| Adults (18-50 yrs) | Streptococcus pneumoniae, N. meningitidis |
| Older adults (>50 yrs) | Streptococcus pneumoniae, Listeria monocytogenes |
| Immunocompromised | Klebsiella, anaerobes, Listeria |
| Post-neurosurgery / trauma | Coagulase-negative staphylococci, Staphylococcus aureus, Cutibacterium acnes, Pseudomonas aeruginosa |
- Robbins & Kumar Basic Pathology, p. 833; Robbins & Cotran, p. 1164; Rosen's Emergency Medicine, p. 2268
Key Organisms - Details
1. Streptococcus pneumoniae (Pneumococcus)
- Most common overall cause in adults, accounting for ~70% of cases in developed countries following Hib vaccination
- Gram-positive, lancet-shaped diplococci
- Exudate is densest over cerebral convexities near the sagittal sinus
- Large amounts of capsular polysaccharide can produce gelatinous exudate and subsequent chronic adhesive arachnoiditis with hydrocephalus
- Highest rates of residual neurologic deficits among survivors
2. Neisseria meningitidis (Meningococcus)
- Gram-negative diplococci
- Predominant pathogen in children and young adults; often causes outbreaks (military barracks, college dormitories)
- Major serogroups: A, B, C, W-135, Y
- Group B: prevalent in Europe
- Group C: common in the United States
- Feared complication: Waterhouse-Friderichsen syndrome - meningococcal (and pneumococcal) septicemia causing bilateral hemorrhagic adrenal infarction
- Conjugate vaccine covers serogroups A, C, Y, W-135; separate vaccine for serogroup B
3. Haemophilus influenzae type b (Hib)
- Gram-negative coccobacillus; requires factors X (hemin) and V (NAD) - grown on chocolate agar
- Exudate is typically basal in distribution
- Incidence has dropped sharply since introduction of the Hib vaccine
- Now affects primarily unvaccinated children and older adults (as illustrated by the nursing-home case above with gram-negative rods in CSF - Medical Microbiology 9e, p. 293)
4. Listeria monocytogenes
- Gram-positive short rod, motile
- Affects neonates and adults >60 years; emerging as one of the most common causes in developed countries
- Highest mortality rate of all causes (up to 27%)
- Requires ampicillin for coverage (cephalosporins are not effective)
5. Group B Streptococcus (S. agalactiae)
- Gram-positive cocci in chains
- Major neonatal pathogen along with E. coli
- Acquired during passage through the birth canal
6. Escherichia coli
- Gram-negative rod
- Key neonatal pathogen; K1 capsular antigen is a major virulence factor
Pathogenesis
- Nasopharyngeal colonization - most organisms (especially N. meningitidis, S. pneumoniae, Hib) colonize the nasopharyngeal mucosa first
- Mucosal invasion - bacteria cross epithelial barriers; polysaccharide capsules protect against phagocytosis
- Bacteremia - organisms seed the bloodstream
- Blood-brain barrier (BBB) crossing - bacteria enter the CSF; host defense mechanisms within CSF are largely ineffective (low immunoglobulin, low complement levels)
- Bacterial proliferation in CSF - triggers leukocyte recruitment
- Inflammatory cascade - cytokines (TNF-α, IL-1, IL-6) released; increased BBB permeability, cerebral vasculitis, edema, raised intracranial pressure
- Decreased cerebral blood flow - can cause cerebral hypoxia and infarction
- Rosen's Emergency Medicine, p. 2268
Morphology / Pathology
Gross:
- Leptomeninges over the brain surface are covered with suppurative exudate
- Meningeal vessels engorged and prominent
- Distribution varies: basal (Hib meningitis) vs. over cerebral convexities (pneumococcal)
- In fulminant cases: inflammation extends to ventricles (ventriculitis)
Microscopic:
- Neutrophils fill the subarachnoid space; concentrated around leptomeningeal blood vessels
- Gram stain shows variable numbers of bacteria
- In severe cases: neutrophil infiltration of leptomeningeal vein walls, focal cerebritis
- Secondary vasculitis and venous thrombosis can cause hemorrhagic cerebral infarction
Sequelae:
-
Leptomeningeal fibrosis → hydrocephalus
-
Pneumococcal-specific: gelatinous polysaccharide exudate → chronic adhesive arachnoiditis
-
Robbins & Cotran, p. 1165
CSF Findings in Bacterial (Pyogenic) Meningitis
| Parameter | Normal | Bacterial Meningitis | Viral | Tuberculous | Cryptococcal |
|---|---|---|---|---|---|
| Opening pressure | <180 mm H₂O | ↑ | ↑ | ↑ | ↑↑ |
| White cells /μL | 0-5 | 100-5000 (neutrophils) | 10-1000 (lymphocytes) | 50-300 (lymphocytes) | 20-500 (lymphocytes) |
| Glucose (mg/dL) | 50-75 | <40 | Normal | <45 | <40 |
| Protein (mg/dL) | 15-40 | 100-500 | 50-100 | 50-300 | >45 |
| Diagnosis | - | Gram stain + culture | Virus-specific PCR | AFB smear/culture/PCR | CrAg, India ink, fungal culture |
- Washington Manual of Medical Therapeutics, p. 520
Gram stain sensitivity: 70-80% in bacterial meningitis. Blood and CSF cultures remain the gold standard. - Quick Compendium of Clinical Pathology 5e, p. 8307
Summary of Epidemiological Impact of Vaccination
-
Hib vaccine: dramatically reduced H. influenzae meningitis in children
-
Pneumococcal conjugate vaccine (PCV): reduced pneumococcal meningitis but S. pneumoniae remains the most common cause in adults (~70%)
-
Meningococcal conjugate vaccine (serogroups A, C, Y, W-135) + separate serogroup B vaccine: highly effective, but not yet broadly distributed in developing countries
-
Net effect: incidence down to 0.5-1.5 per 100,000 adults in developed countries; mortality (~15%) largely unchanged
-
Goldman-Cecil Medicine, p. 3997-3999
This is a shared conversation. Sign in to Orris to start your own chat.