Meningitis
Reading File
Finding Sources
Searching PubMed
"meningitis" AND "management"
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Reading File
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
I have comprehensive information from multiple authoritative textbooks. Let me now compile the full response.
Meningitis - Comprehensive Overview
Definition
Meningitis is an inflammatory process involving the arachnoid membrane, pia mater, and the intervening cerebrospinal fluid (CSF) within the subarachnoid space. The inflammatory process extends throughout the subarachnoid space around the brain and spinal cord and involves the ventricles. When the infection spreads into the underlying brain parenchyma, it is termed meningoencephalitis.
- Goldman-Cecil Medicine, p. 3997
- Robbins & Kumar Basic Pathology, p. 833
Classification
| Type | Onset | CSF Pattern | Common Causes |
|---|---|---|---|
| Acute Pyogenic (Bacterial) | Hours to days | PMN pleocytosis | S. pneumoniae, N. meningitidis, Group B Strep, L. monocytogenes |
| Aseptic (Viral) | Days | Lymphocytic pleocytosis | Enteroviruses, HSV, EBV |
| Chronic | Weeks to months | Lymphocytic ± elevated protein | M. tuberculosis, fungi (Cryptococcus), Treponema, Brucella |
- Robbins & Kumar Basic Pathology
Epidemiology
-
Global incidence: ~1.2 million cases per year
-
In the US, the leading causes of bacterial meningitis are: S. pneumoniae (58%), Group B Streptococcus (18.1%), N. meningitidis (13.9%), H. influenzae (6.7%), and L. monocytogenes (3.4%)
-
Mortality is ~15% in developed countries, with rates unchanged despite antibiotic advances
-
Vaccines against Hib, S. pneumoniae, and N. meningitidis have dramatically reduced incidence (now 0.5-1.5 cases/100,000 adults in developed countries)
-
S. pneumoniae is now the most common cause, predominating in older adults
-
Goldman-Cecil Medicine; Tintinalli's Emergency Medicine
Pathogens by Age Group
| Age Group | Predominant Organisms |
|---|---|
| Neonates (<1 month) | Group B Streptococcus, E. coli, L. monocytogenes |
| Infants / Children | N. meningitidis, S. pneumoniae |
| Adolescents / Young adults | N. meningitidis (especially in dormitories, military barracks) |
| Adults | S. pneumoniae, N. meningitidis |
| Adults >50 / Immunocompromised | S. pneumoniae, L. monocytogenes |
| Post-neurosurgery / Trauma | Coagulase-negative staphylococci, S. aureus, Cutibacterium acnes, Pseudomonas |
- Bradley and Daroff's Neurology in Clinical Practice; Rosen's Emergency Medicine
Pathophysiology
Bacterial meningitis begins primarily with nasopharyngeal colonization (S. pneumoniae, N. meningitidis):
- Bacteria invade bloodstream → cross the blood-brain barrier into the CSF
- CSF lacks effective host defenses → rapid bacterial proliferation
- Cytokine release triggers leukocyte infiltration into CSF
- Inflammatory cascade → increased BBB permeability, cerebral vasculitis
- Three types of cerebral edema develop:
- Vasogenic (increased BBB permeability, protein/water entry)
- Interstitial (hydrocephalus - reduced arachnoid granule absorption)
- Cytotoxic (disrupted cell membrane homeostasis)
- Elevated ICP → decreased cerebral blood flow → ischemia/thrombosis
- Neurons injured by free radicals from granulocytes and endothelial cells
Direct contiguous spread also occurs from sinusitis, otitis media, brain abscess, penetrating trauma, or neurosurgical procedures.
- Tintinalli's Emergency Medicine; Rosen's Emergency Medicine
Gross Pathology
The image below (from Robbins & Kumar Basic Pathology) shows the characteristic appearance of bacterial meningitis in brain cross-section:
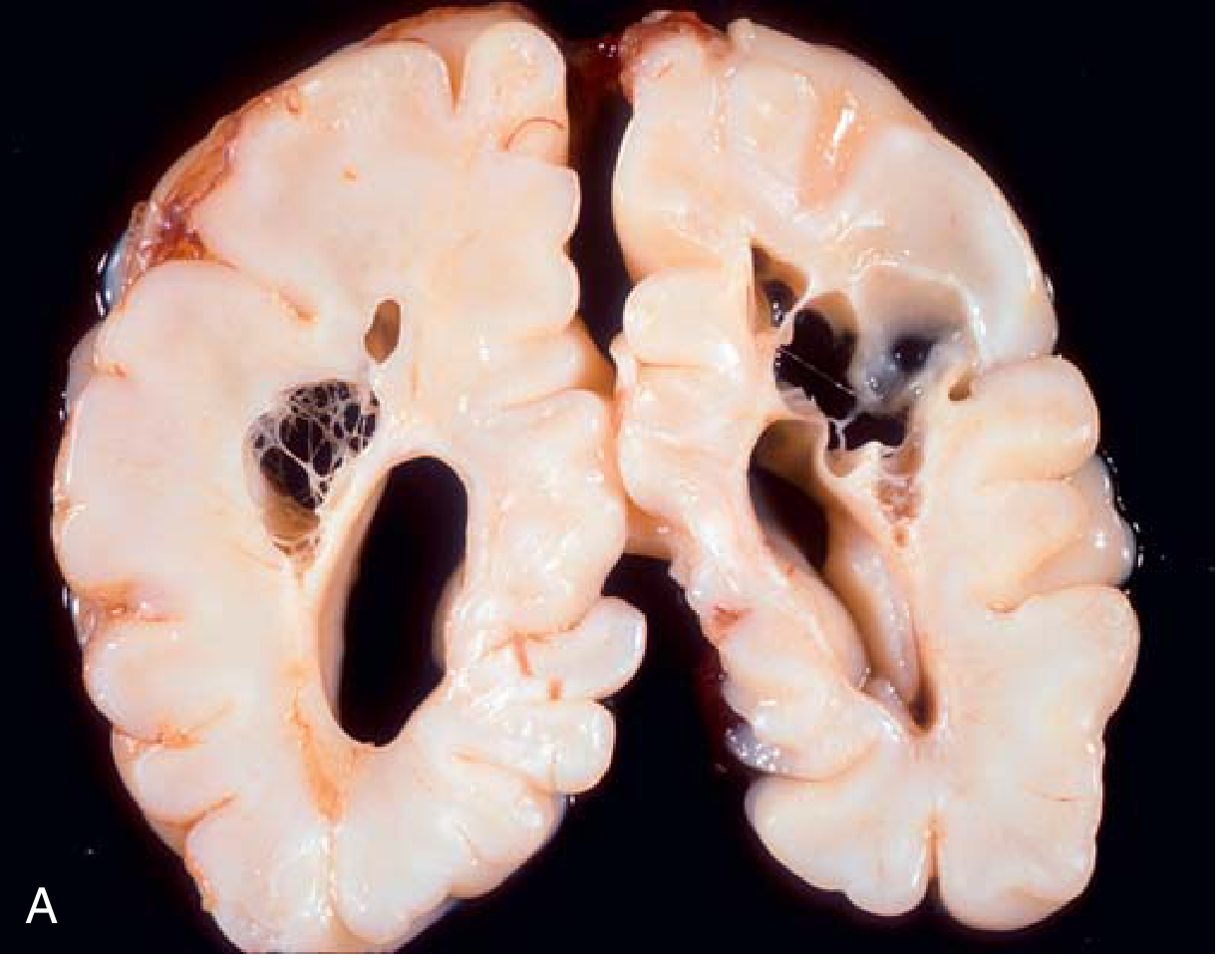
FIG: Bacterial meningitis - cross-section showing dark purulent exudate filling the subarachnoid spaces
Grossly, the meninges appear cloudy or frankly purulent. There is a neutrophil-rich exudate in the subarachnoid space, and the brain may appear congested. In severe cases, exudate may organize to cause obstructive hydrocephalus.
Risk Factors
-
Acute or chronic otitis media / sinusitis
-
Immunosuppression / splenectomy
-
Alcoholism
-
Diabetes mellitus
-
CSF leak (basal skull fracture)
-
Endocarditis
-
Neurosurgical procedures / head injury
-
Close living quarters (N. meningitidis)
-
Tintinalli's Emergency Medicine
Clinical Features
Classic Triad (and Tetrad)
- Fever
- Severe headache (most common; >85% of patients)
- Nuchal rigidity (neck stiffness)
- Altered mental status (tetrad)
Most patients have at least two of four of these symptoms. Seizures and focal neurologic deficits occur in 25-30%.
Meningeal Signs
| Sign | Test | Sensitivity | Specificity |
|---|---|---|---|
| Kernig's sign | Inability to extend knee when hip flexed to 90° (supine) | <12% | High |
| Brudzinski's sign | Passive neck flexion causes hip/knee flexion | <12% | High |
Both signs are highly specific but insensitive - their presence strongly suggests meningitis; their absence does NOT rule it out.
Special Populations
- Immunocompromised / elderly: Altered mental status may be the ONLY finding
- Neonates: Bulging fontanelle, behavioral changes, decreased tone (subtle)
- Lower threshold for LP evaluation in these groups
Additional Findings
-
Petechiae/purpura: Characteristic of meningococcemia (extremities, but anywhere) - indicates endotoxic shock risk
-
Waterhouse-Friderichsen syndrome: Bilateral adrenal hemorrhage from meningococcemia + DIC + purpura
-
Cerebral venous thrombosis: ~1% of meningitis cases - manifests as new seizures, focal deficits
-
Signs of source infection (otitis media, sinusitis, endocarditis skin lesions)
-
Rosen's Emergency Medicine; Bradley and Daroff's Neurology in Clinical Practice
CSF Findings - Lumbar Puncture
Harrison's Principles of Internal Medicine (2025, Table 143-2):
| Parameter | Bacterial Meningitis | Viral Meningitis | Normal |
|---|---|---|---|
| Opening pressure | >180 mmH₂O (200-500 mmH₂O) | Normal / mildly elevated | 70-180 mmH₂O |
| WBC | 10-10,000/μL; PMN predominance | 10-100; lymphocytic | <10/mm³ |
| Protein | >45 mg/dL (often >100) | 60-100 mg/dL | <45 mg/dL |
| Glucose | <40 mg/dL (or CSF:serum ratio <0.4) | Normal (40-80 mg/dL) | 40-80 mg/dL |
| Gram stain | Positive in >60% | Negative | - |
| Culture | Positive in >80% | Negative | - |
-
Hypoglycorrhachia (CSF glucose <40 mg/dL) is the hallmark of bacterial meningitis
-
PMN count >1,180 cells/μL has 99% predictive value for bacterial meningitis
-
Viral meningitis: lymphocytic pleocytosis, normal glucose - viral neutrophilia shifts to lymphocytic within 2-3 days
-
Harrison's Principles of Internal Medicine 22E; Harriet Lane Handbook; Henry's Clinical Diagnosis
Gram Stain Findings by Organism
| Organism | Gram Stain |
|---|---|
| S. pneumoniae | Gram-positive diplococci in pairs |
| N. meningitidis | Gram-negative diplococcus |
| L. monocytogenes | Gram-positive rods |
| H. influenzae | Gram-negative coccobacillus |
- Bradley and Daroff's Neurology
Diagnostic Approach
Blood Tests
- Blood cultures (ideally before antibiotics - but do NOT delay antibiotics)
- CBC with differential, CMP (serum glucose to interpret CSF glucose)
- Procalcitonin: sensitivity ~90%, specificity ~98% for bacterial vs. viral (useful adjunct, not definitive)
- ESR, CRP: elevated but non-diagnostic
- Coagulation studies if anticoagulated
When to CT First (Before LP)?
CT should be obtained BEFORE LP if any of these are present:
- Papilledema or absent venous pulsations
- New-onset seizures
- Abnormal level of consciousness
- Focal neurologic deficits
If no focal findings, proceed directly to LP without CT.
Key principle: Neuroimaging and LP must NOT delay antibiotic administration. Start empiric antibiotics immediately if meningitis is strongly suspected.
MRI
-
More sensitive than CT for complications
-
Meningeal enhancement with gadolinium (non-specific - indicates increased BBB permeability)
-
HSV encephalitis: T2/FLAIR high-signal in temporal lobes within 48h (not seen in bacterial meningitis)
-
Rosen's Emergency Medicine
Treatment
Empiric Antibiotic Therapy
Tintinalli's Emergency Medicine (Table 174-4):
| Patient | First-Line Empiric Regimen | Target Organisms |
|---|---|---|
| Immunocompetent adult | Ceftriaxone 2g IV q12h + Vancomycin 15-20 mg/kg IV | S. pneumoniae, N. meningitidis |
| Age >50 / immunocompromised | Ceftriaxone 2g IV + Vancomycin + Ampicillin 2g IV | Add L. monocytogenes coverage |
| Penicillin allergy (severe) | Meropenem 2g IV or Moxifloxacin 400mg IV (replace ceftriaxone) | - |
| Post-neurosurgery / trauma | Vancomycin + Cefepime or Meropenem | Staph, Pseudomonas coverage |
| Neonates (<1 month) | Ampicillin + Cefotaxime (or ceftazidime) | GBS, E. coli, Listeria |
CNS dosing (Bradley-Daroff):
- Vancomycin: 40-60 mg/kg/day q8-12h
- Ceftriaxone: 2g q12h
- Ampicillin: 2g q4h
Dexamethasone (Adjunctive Corticosteroid)
-
Give 10 mg IV q6h x 4 days (adults)
-
Administer before or with the first dose of antibiotics
-
Benefits: reduces mortality and morbidity (especially in S. pneumoniae meningitis), reduces hearing loss and neurologic sequelae in children
-
Landmark 2002 RCT (de Gans et al.): dexamethasone significantly improved outcomes; all mortality/morbidity benefits in pneumococcal subgroup
-
Can be given up to 4 hours after antibiotic start if not given initially
-
Note: Concurrent dexamethasone does NOT significantly reduce CSF vancomycin concentration - serum levels remain proportional to CSF levels
-
Bradley and Daroff's Neurology; Tintinalli's Emergency Medicine
Narrowing Therapy
Once organism and sensitivities are known, narrow to targeted antibiotic based on culture and sensitivity results.
Complications
| Complication | Notes |
|---|---|
| Hearing loss | Can appear within 1 day of onset; resolves in ~50% of acute cases |
| Hydrocephalus | Uncommon; from exudate organization blocking CSF flow |
| Cerebral venous sinus thrombosis | ~1% of cases; new seizures/focal deficits |
| Waterhouse-Friderichsen syndrome | Bilateral adrenal hemorrhage (meningococcal); DIC, purpura, shock |
| Residual neurologic deficits | Highest in pneumococcal meningitis |
| Death | Overall ~15%; Listeria highest (up to 27%) |
- Rosen's Emergency Medicine; Adams and Victor's Neurology
Viral Meningitis (Aseptic Meningitis)
- Now the most common type of meningitis (vaccines reduced bacterial incidence)
- Causes: Enteroviruses and Herpesviruses (most common); also mumps, HIV
- Clinical: similar symptoms but generally milder
- CSF: lymphocytic pleocytosis, normal glucose, mildly elevated protein
- Prognosis: excellent for the majority
- Treatment: supportive (antivirals for HSV/VZV)
Tuberculous Meningitis (Chronic Meningitis)
- Subacute/chronic presentation (symptoms developing over weeks/months)
- Symptoms: fever, weight loss, night sweats, malaise ± headache
- Leading cause of chronic meningitis globally due to worldwide endemicity
- CSF: initially modest PMN pleocytosis → rapidly evolves to lymphocytic predominance
- Diagnosis: 20-30 mL CSF for AFB stain and culture; PCR
- 2026 Lancet Infectious Diseases [PMID: 40840485] published a new clinical practice guideline for tuberculous meningitis (Feb 2026)
Fungal Meningitis
- Often subtle presentation even in healthy adults
- Common in immunocompromised (HIV/AIDS): Cryptococcus neoformans
- Symptoms: headache, low-grade fever, malaise, weight loss
- Diagnosis: India ink, cryptococcal antigen, CSF fungal culture
- Treatment: Amphotericin B + flucytosine (induction), then fluconazole (maintenance)
Prevention / Vaccination
| Vaccine | Target Organisms | Notes |
|---|---|---|
| Hib vaccine | H. influenzae type b | Dramatically reduced meningitis in children |
| Pneumococcal vaccines (PCV/PPSV) | S. pneumoniae | Reduced meningitis + otitis media |
| Meningococcal conjugate (MenACWY) | N. meningitidis A, C, W-135, Y | Recommended for adolescents, college freshmen |
| MenB vaccine | N. meningitidis serogroup B | Now required at most US universities; given separately |
- Bradley and Daroff's Neurology in Clinical Practice
Recent Evidence (2024-2026)
- A new clinical practice guideline for tuberculous meningitis was published in Lancet Infectious Diseases (Feb 2026) - [PMID: 40840485] - providing updated recommendations for a disease that remains a major global challenge.
- A systematic review on IgG4-related pachymeningitis (JAMA Neurology, Feb 2025, [PMID: 39556369]) characterized the clinical presentation, investigation findings, and outcomes of this rare autoimmune form.
Sources: Goldman-Cecil Medicine | Harrison's Principles of Internal Medicine 22E | Bradley and Daroff's Neurology in Clinical Practice | Rosen's Emergency Medicine | Tintinalli's Emergency Medicine | Robbins & Kumar Basic Pathology | Harriet Lane Handbook 23e | Henry's Clinical Diagnosis and Management | Adams and Victor's Neurology 12e
This is a shared conversation. Sign in to Orris to start your own chat.