Explain me about FUE hair transplant in detail
Reading File
Finding Sources
Searching the Web
FUE hair transplant procedure technique outcomes 2025
Searching PubMed
follicular unit extraction hair transplantation
Finding Sources
Reading Article
PMID: 40354670
Reading Web Page
https://jdcronline.org/article/innovations-in-follicular-uni…
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Here is a detailed, evidence-based breakdown of FUE hair transplantation.
Follicular Unit Extraction (FUE) - Complete Guide
What Is FUE?
FUE is a minimally invasive surgical hair restoration technique in which individual follicular units (natural groupings of 1-4 terminal hairs with their surrounding sebaceous glands, connective tissue, and erector pili muscle) are extracted one by one from the donor scalp using small circular punch devices (0.75-1.2 mm in diameter) and transplanted into recipient sites in the balding area.
It was developed primarily to avoid the linear scar left by the older Follicular Unit Transplantation (FUT/strip) method, and is now the globally dominant technique in hair restoration.
The entire procedure rests on the principle of donor dominance: transplanted hair retains the genetic characteristics of its donor site. Hair from the permanent occipital (back of scalp) zone does not respond to DHT-driven miniaturization, so it continues to grow permanently at the new location.
Anatomy of a Follicular Unit
Each follicular unit contains:
- 1-4 terminal hairs
- Sebaceous glands
- Erector pili muscle
- Perifollicular vascular plexus
- Surrounding connective tissue sheath
These microanatomic units are the building blocks of modern hair transplantation. Recipient site density is typically designed at 35-40 follicular units/cm², though lower density may be used in areas with pre-existing hair.
Biological Basis: Why FUE Works
The scalp contains approximately 100,000 hairs cycling through four phases:
- Anagen (growth phase): ~90% of follicles, lasts 3-4 years
- Catagen (involution): ~1% of follicles, lasts ~2 weeks
- Telogen (rest): ~10% of follicles, lasts 3-4 months
- Exogen (shedding): leads to normal daily loss of 50-100 hairs
Androgenetic alopecia (AGA), the most common indication for FUE, is driven by DHT (dihydrotestosterone) causing progressive miniaturization of genetically susceptible follicles in the frontotemporal and vertex regions. The mid-occipital and parieto-occipital zones are DHT-resistant and serve as the permanent donor pool.
Indications
- Androgenetic alopecia (AGA) - the primary indication in men and women
- Patients who want to keep their hair closely cropped (FUT leaves a linear scar; FUE leaves only diffuse small circular dots)
- Patients with reduced scalp laxity from prior strip surgery
- Eyebrow, beard, and eyelash restoration
- Scar camouflage (surgical scars, burn scars, traction alopecia)
- End-stage cicatricial alopecia (only after 2-5 years of disease stability, no active inflammation)
- Gender-affirmation hairline surgery
Patient Selection and Candidacy
Good candidacy depends on:
- Donor density: A minimum of 40 follicular units/cm² in the occipital scalp is required. The average is 65-85 FU/cm². Below 40 FU/cm² = poor candidate.
- Stable hair loss: Surgery should not be performed on actively progressing, unstable hair loss. Young patients especially must be counseled that transplanted hair will grow, but surrounding native hair will continue thinning.
- Realistic expectations: Hair transplantation rearranges existing hair; it does not create new hair. Net density = grafts transplanted minus ongoing loss.
- Medical fitness: Pre-operative labs for females with alopecia should include thyroid function, CBC, and iron studies. In cases with signs of androgen excess, total testosterone, DHEA, and prolactin levels are checked.
- Exclusions: Active cicatricial or inflammatory alopecias require biopsy and disease stabilization before considering surgery. A positive hair pull test (>5 telogen hairs from a 30-40 hair cluster) should prompt postponement until the etiology is identified.
The law of MPB governs candidacy: the more advanced the baldness, the more grafts are needed - but the fewer grafts are available, due to the inverse relationship between donor and recipient areas.
The Procedure - Step by Step
1. Pre-operative Planning
- Hairline design is mapped to create a natural, lifelong-appropriate anterior hairline. The frontal scalp is prioritized over the vertex since vertex transplants consume many grafts and can develop a peripheral bald rim over time as AGA progresses in a 360° pattern.
- Donor hair in the mid-occipital scalp between the upper and lower occipital protuberances is assessed for density and quality.
- Harvesting too superiorly may later expose surgical sites as AGA advances.
2. Anesthesia
- Local anesthesia using 1% lidocaine with epinephrine is infiltrated into both donor and recipient areas.
- Tumescence (injection of bacteriostatic normal saline) is added to create dermal turgor, which reduces follicular transection and minimizes bleeding.
3. Donor Harvest (FUE Technique)
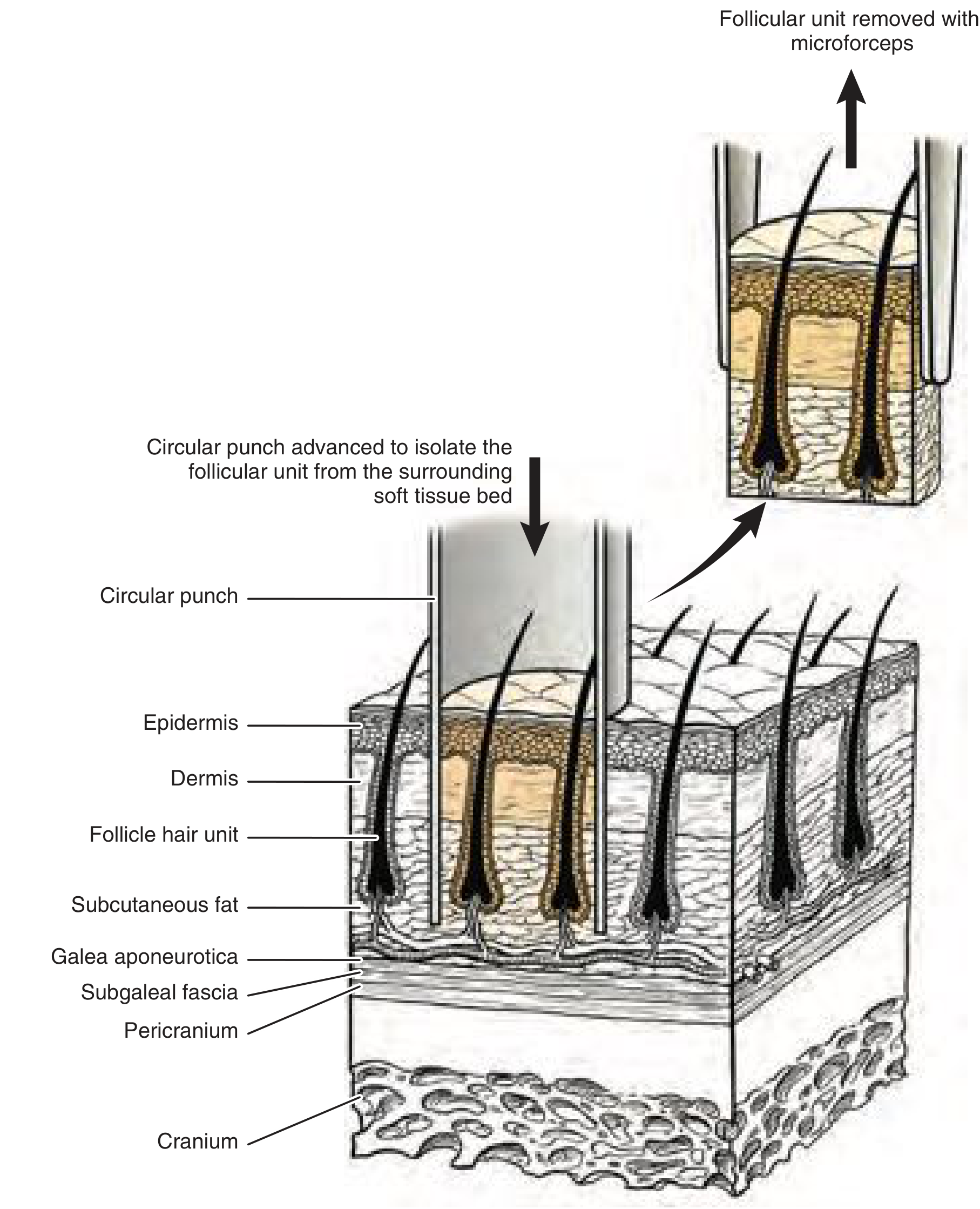
- Hair is trimmed to ~1 mm to accurately identify the true angle of follicular emergence. Trimming too long makes the apparent angle more acute than the real angle; too short conceals it.
- A small circular punch (0.75-1.2 mm) is positioned centered over each individual follicular unit. The incision must follow the hair shaft angle precisely, since follicles curve with the concavity on the acute-angle side.
- The technique involves:
- First, a shallow incision perpendicular to the skin to score the epidermis
- Then, a deeper angled incision following the follicular path into perifollicular fat
- The follicle is then gently grasped with microforceps and lifted free
- Grafts are immediately placed into chilled saline or holding solution to prevent desiccation.
- Because of follicular splay within groupings, a punch diameter of 0.8-0.9 mm yields an average of 2.10-2.25 follicles/graft.
Technical key points to avoid transection:
- The inferior side of the punch contacts skin first (hair grows at an acute angle)
- Applying excessive axial force displaces and amputates the follicular bulb; rotational or oscillatory force is preferred
- Skin tension from tumescence or manual traction helps prevent graft torsion
- Sharp, thin-walled instruments minimize frictional forces
4. Graft Storage
- Grafts are kept moist in saline-filled Petri dishes throughout the procedure
- Chilled conditions slow metabolism and preserve viability
- Grafts must be replanted with minimal out-of-body time
5. Recipient Site Creation
- The physician creates small recipient sites (incisions) in the bald/thinning area at the planned density and appropriate hair direction/angle.
- Site angle, direction, and depth determine the cosmetic naturalness of the result.
- Recipient density is typically 35-40 FU/cm².
6. Graft Placement (Implantation)
- Technicians carefully insert grafts into recipient sites using fine forceps or implanter pens.
- Single-hair grafts go at the hairline; 2-3 hair grafts provide density behind.
- The use of implanter pens (DHI method - Direct Hair Implantation) allows simultaneous creation of the recipient site and placement of the graft, offering fine control over depth, angle, and spacing.
FUE Variants and Technologies
| Method | Key Feature |
|---|---|
| Manual FUE | Surgeon uses hand-held punch; most time-consuming, highest transection risk |
| Motorized FUE | Powered rotation/oscillation punch; faster harvest, larger graft numbers per session |
| Robotic FUE (ARTAS) | AI-guided image analysis directs robotic punch extraction; highest patient satisfaction, lowest complication rate (10%), highest cost |
| DHI (Direct Hair Implantation) | Implanter-pen delivery; no separate recipient site creation step |
| Unshaven/Long-Hair FUE (U-FUE) | No full shave required; discreet recovery, preview of hair direction in real time |
| Sapphire FUE | Sapphire-bladed recipient site creation; smaller, more precise incisions |
Graft survival rates across all three major FUE types are statistically similar (~87-89%) based on 2025 data. Complication rates differ: robotic 10%, motorized 15%, manual FUE 20%.
FUE vs. FUT (Strip): Comparison
| Feature | FUT (Elliptical Strip) | FUE |
|---|---|---|
| Visible scar | Yes (linear) | No (diffuse white dots only) |
| Follicular transection | Minimal | Variable (higher) |
| Harvest time | 10-20 min | 30-90 min |
| Graft preparation time | Lengthy (lab dissection) | Minimal |
| Post-op pain | More | Less |
| Short hairstyle compatible | No | Yes |
| Body hair harvesting | No | Yes |
| Quality of transplant | Excellent | Excellent |
Post-operative Care and Recovery
- Small circular punch wounds heal spontaneously without sutures
- Swelling of the forehead and periorbital region is common in the first 3-5 days
- Crusting around transplanted grafts occurs over 1-2 weeks
- Shock loss (telogen effluvium): Transplanted hairs shed 2-6 weeks post-op. This is normal - the follicle remains alive and will re-enter anagen.
- New growth begins at 3-4 months, with significant density visible at 6-9 months, and full results at 12-18 months.
- Donor sites typically show only small diffuse "white dots" if closely cropped - this should be discussed with patients pre-operatively.
Adjuvant Therapies
- Platelet-Rich Plasma (PRP): Growth factors (PDGF, TGF-β, VEGF, EGF) may support wound healing and graft survival. Evidence is mixed; no optimal protocol is established yet, but it is increasingly used post-transplant.
- Minoxidil and finasteride: Concurrent medical management helps preserve remaining native hair and maintain long-term density. This is a key component of modern hair restoration planning.
Complications
| Complication | Notes |
|---|---|
| Folliculitis | Most common across all FUE types; treatable with antibiotics |
| Infection | More common with manual FUE |
| Swelling/edema | Common with motorized FUE |
| Follicular transection | Higher than in strip harvesting; directly impacts graft yield |
| Donor area thinning | Risk with repeated sessions; total lifetime follicle count is similar to FUT |
| Ingrown hairs / epidermal cysts | From buried graft fragments |
| Poor growth / low density | Graft desiccation, poor blood supply, or improper depth |
| Shock loss (telogen effluvium) | Expected; resolves with regrowth |
Future Directions
According to a 2025 state-of-the-art review (Queen & Avram, Dermatologic Surgery, PMID 40354670):
- AI-assisted and robotic systems are improving precision and consistency
- Hair follicle cloning (multiplication of follicular units in vitro) remains an active area of research
- Stem cell therapies are being explored for follicular regeneration
- Refined implanter instruments and smarter adjuvant medical management continue to improve long-term density and patient satisfaction
Summary
FUE is the current standard of care in hair transplantation, particularly favored for its lack of linear scarring, shorter recovery, lower post-op pain, and versatility. Its main limitations are longer operative time, variable follicular transection rates, and the finite donor supply that constrains how many grafts can be moved over a lifetime. Proper patient selection, conservative hairline design, concurrent medical therapy, and skilled technique are the foundations of excellent, long-lasting outcomes.
- Dermatology 2-Volume Set 5e, Elsevier
- Cummings Otolaryngology Head and Neck Surgery
- Queen D, Avram MR. Hair Transplantation: State of the Art. Dermatol Surg 2025. PMID 40354670
This is a shared conversation. Sign in to Orris to start your own chat.