Pulmonary embolism
Reading File
Finding Sources
Searching PubMed
"pulmonary embolism"[MeSH Terms] AND "diagnosis"[MeSH Terms]
Searching Images
pulmonary embolism CT angiography diagnosis
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Excellent — I now have very rich content. Let me compile a comprehensive response covering all key aspects of PE.
Pulmonary Embolism (PE)
Definition & Epidemiology
Pulmonary embolism is the occlusion of one or more pulmonary arteries by thrombus, most commonly originating from deep vein thrombosis (DVT) of the lower extremities. It is part of the venous thromboembolism (VTE) spectrum. PE accounts for approximately 25% of sudden cardiac deaths and is a leading cause of maternal mortality (15% of maternal deaths in the US, 2003–2011).
Pathophysiology
The classic Virchow's Triad drives thrombus formation:
- Venous stasis — prolonged immobility, uterine compression of IVC
- Hypercoagulability — inherited (Factor V Leiden, protein C/S deficiency, antithrombin deficiency, prothrombin G20210A) or acquired (malignancy, antiphospholipid syndrome, OCP use, pregnancy)
- Endothelial injury — surgery, trauma, catheter placement
When a clot occludes the pulmonary vasculature:
- Right ventricular (RV) afterload increases acutely
- RV dilation → interventricular septal deviation → compresses the left ventricle
- LV filling decreases → reduced cardiac output → systemic hypotension
- Coronary perfusion falls → RV ischemia → spiral of cardiac failure
- Respiratory consequences: dead-space ventilation, hypoxemia, reflex bronchoconstriction
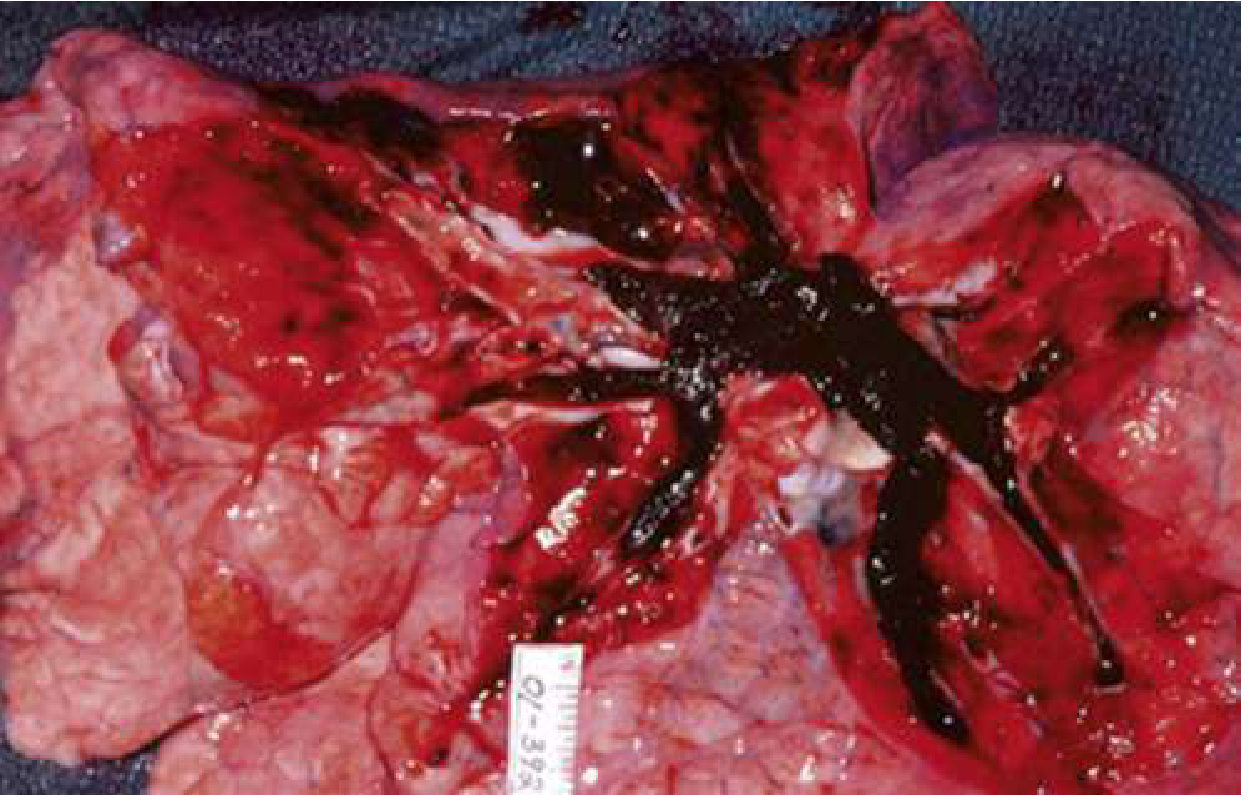
In its most extreme form, the clot can completely obstruct the RV outflow system:
Risk Factors
| Category | Examples |
|---|---|
| Provoked | Surgery (especially orthopedic), trauma, hospitalization, immobilization, pregnancy/postpartum |
| Hypercoagulable states | Cancer, Factor V Leiden, protein C/S/antithrombin deficiency, antiphospholipid syndrome |
| Other | Prior VTE, obesity, smoking, OCP/HRT, age >35 y, central venous catheter |
Clinical Presentation
Symptoms
PE presentation ranges from asymptomatic to sudden cardiovascular collapse.
| Symptom | Frequency |
|---|---|
| Dyspnea | 75–80% |
| Chest pain (pleuritic or dull) | ~67% |
| Pleuritic chest pain specifically | ~20% |
| Cough / hemoptysis | Less common |
| Unilateral leg swelling | <30% |
| Syncope | <5% of syncope presentations |
- Dyspnea is the most common symptom but absent in ~25% of patients — do not rule out PE based on its absence
- Pleuritic pain suggests peripheral PE causing pulmonary infarction
- Fever from PE is low-grade; temperature >38.6°C (101.5°F) suggests infection
- Syncope alone, especially with risk factors, can be a PE presentation
Vital Signs
| Finding | Notes |
|---|---|
| Tachycardia (HR >100) | ~50%; shock index (HR > SBP) suggests severe PE |
| Tachypnea (RR >20) | ~50% |
| Hypotension (SBP <90) | ~10%; 4-fold increase in mortality |
| Hypoxemia (SpO₂ <95%) | ~50% of PE patients have normal SpO₂ |
⚠ Normal O₂ saturation cannot rule out PE. Normalization of vital signs does not reduce PE probability.
Physical Examination
- Usually unremarkable
- DVT signs (unilateral edema, leg asymmetry, vein tenderness) are the only findings that reliably increase PE probability
- Wheezing → favors bronchospasm over PE; bilateral rales → favors LV failure
Cardiac Arrest from PE
- PEA (pulseless electrical activity) is the most common ECG finding in PE-related arrest
- Survival rate from PE cardiac arrest ≈ 20% even with witnessed arrest and thrombolytics
Diagnosis
Clinical Pre-test Probability
Wells PE Score (most widely validated):
| Criterion | Points |
|---|---|
| Clinical signs/symptoms of DVT | +3 |
| PE more likely than alternative diagnosis | +3 |
| HR >100 | +1.5 |
| Immobilization ≥3 days or surgery in past 4 weeks | +1.5 |
| Previous DVT/PE | +1.5 |
| Hemoptysis | +1 |
| Malignancy (treatment within 6 months or palliative) | +1 |
- Low: ≤1 | Moderate: 2–6 | High: ≥7
- Two-level version: ≤4 = PE unlikely; >4 = PE likely
PERC Rule (Pulmonary Embolism Rule-out Criteria) — can exclude PE without further workup if ALL 8 criteria are met and pre-test probability is low:
- Age <50, HR <100, SpO₂ ≥95%, no unilateral leg swelling, no hemoptysis, no recent trauma/surgery, no prior DVT/PE, no exogenous estrogen use
Laboratory Tests
- D-dimer: High sensitivity (~98%), low specificity. A negative D-dimer (<500 ng/mL) with low pre-test probability effectively rules out PE. Not useful if probability is high. In the elderly, age-adjusted cutoff = age × 10 ng/mL (e.g., age 70 → cutoff 700 ng/mL).
- Troponin I/T and BNP/NT-proBNP: Markers of RV strain — useful for risk stratification, not diagnosis. Elevated troponin indicates RV myocardial injury and portends worse prognosis.
- ABG: May show hypoxemia, hypocapnia (respiratory alkalosis), increased A-a gradient — nonspecific
ECG
- Sinus tachycardia (most common)
- S1Q3T3 pattern (S wave in lead I, Q wave and T-wave inversion in lead III) — classic but insensitive (~20%)
- Right bundle branch block (complete or incomplete)
- T-wave inversions in V1–V4 (RV strain pattern)
- New right axis deviation
Chest X-Ray
Usually normal, but can show:
- Westermark sign: Focal oligemia (hypovascular zone distal to obstructed vessel)
- Hampton's hump: Peripheral wedge-shaped opacity (pulmonary infarction)
- Palla sign: Enlarged right descending pulmonary artery
- Elevated hemidiaphragm, atelectasis, small pleural effusion
Imaging
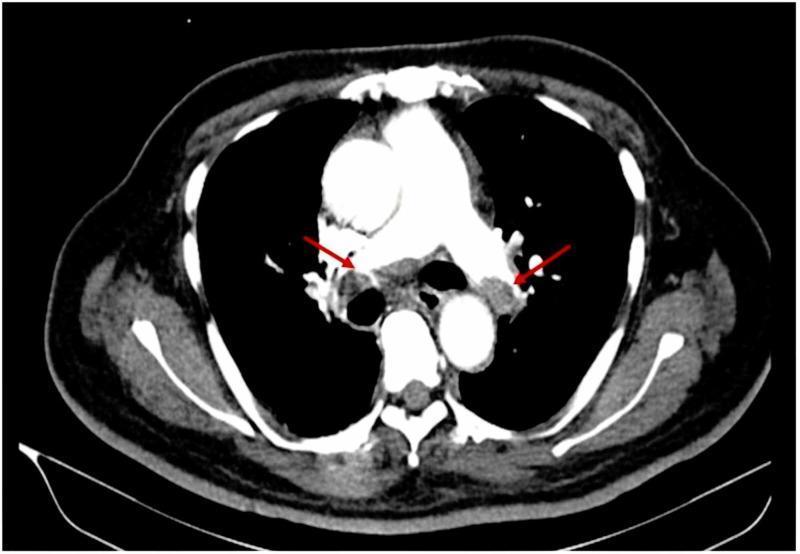
CT Pulmonary Angiography (CTPA) — gold standard for most patients:
- Sensitivity ~96%, specificity ~98% for segmental/larger PE
- Shows hypodense intraluminal filling defects within pulmonary arteries
V/Q Scan (Ventilation-Perfusion):
- Preferred when CTPA is contraindicated (renal failure, contrast allergy, pregnancy)
- In pregnancy: halving the perfusion dose is standard practice; fetal radiation exposure ≈ 0.011–0.022 cGy
- Results: Normal (rules out PE), High probability, Indeterminate
Compression Ultrasound of lower extremities: If DVT found, anticoagulation is indicated even without CTPA
Echocardiography: Useful in hemodynamically unstable patients (bedside for RV dilation, RV hypokinesis, McConnell sign, clot-in-transit)
MRI Pulmonary Angiography: Emerging option; a 2025 meta-analysis (PMID 40114100) confirms MRI has good diagnostic accuracy but remains limited by availability.
Risk Stratification
| Category | Definition | Mortality |
|---|---|---|
| Massive / High-risk | SBP <90 mmHg or hemodynamic instability | >15% |
| Submassive / Intermediate-risk | Normotensive + RV dysfunction (echo/CT) OR elevated troponin/BNP | 3–15% |
| Low-risk | Normotensive, no RV dysfunction, normal biomarkers | <2% |
Treatment
General Supportive Care
- Supplemental oxygen; mechanical ventilation if needed (use low tidal volumes to avoid worsening RV dilation from high intrathoracic pressures)
- IV fluids cautiously — excessive volume can worsen RV dilation
- Vasopressors (norepinephrine preferred) for hemodynamic instability
Anticoagulation (cornerstone of treatment)
All non-massive PE (hemodynamically stable):
| Drug | Route | Notes |
|---|---|---|
| Unfractionated heparin (UFH) | IV bolus + infusion | Preferred when thrombolysis/procedure may be needed; easily reversible |
| LMWH (enoxaparin, dalteparin) | SC | Preferred for cancer-associated PE; avoid if severe renal failure |
| Fondaparinux | SC | Alternative to LMWH |
| Direct oral anticoagulants (DOACs) | Oral | Rivaroxaban & apixaban: approved for PE, no need for initial parenteral therapy (acute-phase dosing) |
| Warfarin | Oral | Requires INR monitoring (target 2–3); bridge with parenteral anticoagulant |
Duration of anticoagulation:
- Provoked (reversible risk factor): 3 months
- Unprovoked or high-recurrence risk: ≥3–6 months, often indefinite
- Cancer-associated VTE: indefinite (LMWH or DOAC preferred)
Pregnancy: LMWH throughout pregnancy (DOACs and warfarin are contraindicated)
Thrombolysis (Systemic)
Indications: Massive PE (hemodynamic instability) without contraindications
- Alteplase 100 mg IV over 2 hours (or 0.6 mg/kg for cardiac arrest)
- Contraindications: recent surgery (<10 days), intracranial pathology, active bleeding, recent stroke
- Survival from PE arrest ≈ 20% even with witnessed arrest + thrombolytics
Catheter-Directed Therapy (CDT)
- Catheter-directed thrombolysis or mechanical thrombectomy
- Considered for submassive PE with high bleeding risk for systemic thrombolysis, or failed systemic lysis
- Effective at restoring patency (as seen in pre/post angiography images of bilateral PE treatment)
Surgical Embolectomy
- Reserved for massive PE with absolute contraindication to thrombolysis or failed thrombolysis
- High-risk procedure
IVC Filter
- Indicated when anticoagulation is absolutely contraindicated (e.g., active hemorrhage)
- Preferred: retrievable filters; permanent filters have long-term complications (IVC thrombosis)
Special Populations
Pregnancy
- VTE risk is 5× higher than non-pregnant age-matched controls
- Diagnosis complicated by: physiological dyspnea, elevated baseline D-dimer
- Left-sided DVT predominates (88% in one series) due to gravid uterus compressing left iliac vein
- A pregnancy-adapted YEARS algorithm has been studied but no strategy can fully safely exclude PE in pregnancy given catastrophic consequences of a missed diagnosis
- Treatment: LMWH throughout pregnancy and ≥6 weeks postpartum (warfarin and DOACs contraindicated)
Cancer
- Highest VTE risk; LMWH (dalteparin) or DOACs (edoxaban, rivaroxaban) preferred
- A 2024 meta-analysis found significant VTE risk in lung cancer (PMID 39183726)
Complications
- Pulmonary hypertension (chronic thromboembolic pulmonary hypertension, CTEPH) — ~4% of PE survivors
- Recurrent VTE — ~30% at 10 years if anticoagulation stopped
- Post-thrombotic syndrome (from underlying DVT)
- Right heart failure (acute cor pulmonale)
Key Mnemonics & Pearls
- "PERC all 8 criteria" — if ALL met with low clinical suspicion, no further workup needed
- Shock index >1 (HR > SBP) — suggests high-risk PE requiring urgent intervention
- Normal SpO₂ does not exclude PE (~50% of PE patients have normal oxygen saturation)
- Normal D-dimer in a low-probability patient effectively rules out PE
- Age-adjusted D-dimer (age × 10 ng/mL for age >50) improves specificity without sacrificing sensitivity
- PEA arrest in an undifferentiated patient → think PE, tension pneumothorax, cardiac tamponade
Sources: Rosen's Emergency Medicine: Concepts and Clinical Practice, 10e | Murray & Nadel's Textbook of Respiratory Medicine, 2-Vol | Miller's Anesthesia, 10e | PMID 40114100 (MRI for PE, 2025) | PMID 39183726 (VTE in lung cancer, 2024)
This is a shared conversation. Sign in to Orris to start your own chat.