How to improve grip in physiology
Reading File
Finding Sources
Finding Sources
Searching the Web
grip strength physiology improvement mechanisms training
Searching PubMed
grip strength training physiology
Finding Sources
Finding Sources
Reading Web Page
grip strength physiology improvement training mechanisms
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have everything needed for a thorough, well-sourced answer. Here it is:
Improving Grip Strength: The Physiology
Grip strength depends on force generated by the finger flexors and intrinsic hand muscles, stabilized by the wrist extensors of the forearm. Improving it requires understanding both the neural and structural adaptations that happen during training.
1. The Core Physiological Principle: Load is Non-Negotiable
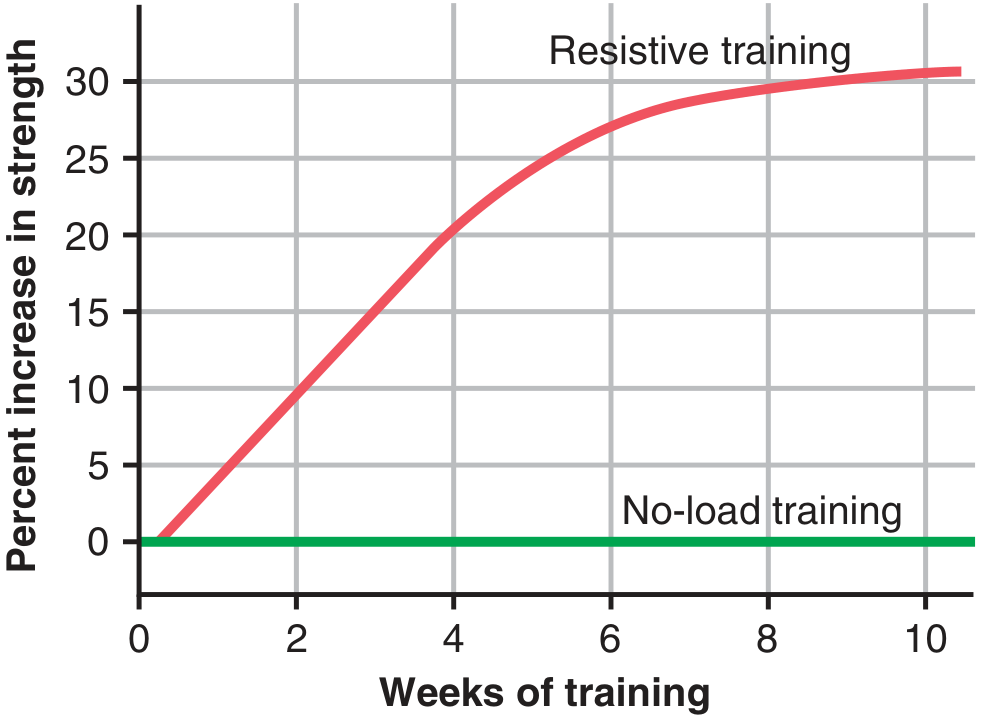
"Muscles that function under no load, even if they are exercised for hours on end, increase little in strength. At the other extreme, muscles that contract at more than 50% maximal force of contraction will develop strength rapidly even if the contractions are performed only a few times each day."
- Guyton and Hall Textbook of Medical Physiology
The practical takeaway: six near-maximal contractions performed in 3 sets, 3 days per week provides approximately optimal strength gains. Expect ~30% increase in strength over the first 6-8 weeks, after which gains plateau.
2. Physiological Adaptations That Drive Strength Gains
A. Muscle Hypertrophy
- Resistance training causes hypertrophy primarily by increasing muscle fiber diameter (not fiber number), resulting in up to 30-60% increase in muscle cross-sectional area.
- Muscle fibers develop a maximum force of 3-4 kg/cm² of muscle area - so increasing cross-sectional area directly scales force output.
- Inside the hypertrophied fiber: increased myofibrils, up to 120% more mitochondrial enzymes, 60-80% more ATP/phosphocreatine, 50% more glycogen stores.
- (Basic Medical Biochemistry - A Clinical Approach, 6e)
B. Neural Adaptations
Early gains (first 2-4 weeks) are primarily neural, not structural:
- Improved motor unit recruitment - the CNS learns to activate more motor units simultaneously
- Better neural synchronization - motor units fire more synchronously, producing higher peak force
- Reduced autogenic inhibition (Golgi tendon organ inhibition) over time
- (Miller's Review of Orthopaedics, 9th ed.)
C. Fiber Type and Specificity
- Grip strength training (high tension, low reps) preferentially hypertrophies Type II (fast-twitch) fibers
- Type II fibers are ~twice the diameter of Type I and produce 2-3× greater power output
- Training can shift fiber composition by up to 10%, but baseline proportions are largely genetic
- (Guyton & Hall, Textbook of Medical Physiology)
D. Metabolic Adaptations
- Increased phosphocreatine (PCr) stores for short burst grip force
- Improved glycogen utilization for sustained grip endurance
- Training increases the capacity of both anaerobic and aerobic metabolic systems by up to 45%
- (Guyton & Hall)
3. Practical Training Strategies (Evidence-Based)
| Method | Mechanism | Implementation |
|---|---|---|
| Crushing grip exercises | Directly loads finger flexors | Grippers, towel wraps on barbells/dumbbells |
| Supporting/static holds | Trains grip endurance via isometric contraction | Deadlift holds, bar hangs, farmer's carries |
| Thick bar training | Greater circumference forces higher muscular force to grip | Wrap a towel around a barbell to increase diameter |
| Wrist curls + extensions | Strengthens flexors while stabilizing extensors | Dumbbell wrist curls; extensors stabilize the wrist during gripping |
| Weighted carries | Integrates grip with full-body stabilization | Farmer's walks, suitcase carries |
Optimal dosing (meta-analysis): At least 9 weeks of task-specific training, intensity at ~75% of 1-rep max, perceived exertion rated "hard," with a multimodal approach (strength + endurance + flexibility) produces the largest effects. - Physiopedia, citing meta-analysis
4. Important Nuances
- Detraining is rapid: a significant decline in strength begins after only 2 weeks without training.
- Specificity matters: exercises that mimic the grip action (crushing, pinching, hooking) transfer better than generic upper-limb training.
- Older adults / sarcopenia: grip strength is a validated marker of overall muscle mass and nutritional status. Resistance training significantly improves handgrip even in sarcopenic patients, and whey protein supplementation during resistance training can augment gains. - PMID 37571361
- Testosterone influences baseline muscle mass and therefore grip ceiling - men have larger absolute values due to this hormonal effect.
5. Clinical Significance of Grip Strength
Grip strength is used as a proxy for:
- Overall nutritional status and muscle mass (marker of sarcopenia)
- Postoperative risk and functional recovery
- Cardiovascular health (poor grip associated with cardiac remodeling)
- Neurological or myopathic disease assessment (e.g., myotonia, CKD-related muscle wasting)
Sources:
- Guyton and Hall Textbook of Medical Physiology - Effect of Athletic Training on Muscles and Muscle Performance
- Basic Medical Biochemistry - A Clinical Approach, 6e - Metabolic Effects of Training
- Miller's Review of Orthopaedics, 9th ed. - Athletic Training, Injury, and Adaptation
- NSCA - Effective Methods of Grip Strength Development
This is a shared conversation. Sign in to Orris to start your own chat.