All about sepsis eli5
Reading File
Finding Sources
Searching the Web
sepsis definition pathophysiology treatment explained simply 2024
Searching PubMed
"sepsis"[MeSH Terms] AND "management"[MeSH Terms]
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
I have excellent data from Harrison's 2025. Now I have everything I need to write a thorough ELI5 explanation of sepsis. Let me compile the full answer.
Sepsis - Explained Like You're 5 (and then some 🧫)
The Simple Version First
Imagine your body as a house. An infection (bacteria, virus, fungus) is like a fire that breaks out in one room - say the kitchen (lungs, bladder, gut). Normally, your immune system - the fire brigade - rushes to that one room, puts out the fire, and everything goes back to normal.
Sepsis happens when the fire brigade goes completely crazy. Instead of putting out the fire in the kitchen, it starts spraying water everywhere - the living room, the bedroom, the electrical wiring. Now you have water damage throughout the whole house. The original fire might even be out, but your house is collapsing anyway.
That "water damage everywhere" is your body attacking its own organs. That's sepsis.
What Is Sepsis? (Official Definition)
The current definition (called Sepsis-3, updated in 2016) says:
Sepsis = life-threatening organ dysfunction caused by a dysregulated host response to infection
- Harrison's Principles of Internal Medicine 22e (2025)
Key point: it's not just an infection. It's what happens when your body's response to the infection goes out of control and starts damaging your own tissues. As Sir William Osler said back in the 1800s: "the patient appears to die from the body's response to infection rather than from it."
Where Does it Come From?
Sepsis can start from almost any infection, but the most common sources are:
| Source | % of cases |
|---|---|
| Urinary tract (UTI gone wrong) | ~49% |
| Lungs (pneumonia) | ~33% |
| Abdomen (appendix, bowel) | ~14% |
| Skin/soft tissue | ~10% |
The most common bugs are:
- Gram-positive bacteria: Staph aureus (including MRSA), Streptococcus, Enterococcus
- Gram-negative bacteria: E. coli, Klebsiella, Pseudomonas
- Can also be caused by fungi or viruses, but bacteria dominate
About 88% of cases start outside the hospital (community-onset) - so most people arrive to the ER already sick.
- Harrison's Principles of Internal Medicine 22e (2025), p. 2360
How Does It Actually Happen? (Pathophysiology)
Here's the chain of events, step by step:
Step 1 - The Alarm Goes Off
When bacteria (or their toxic parts) enter the bloodstream or overwhelm a local infection, your immune cells - especially macrophages and neutrophils - detect them using pattern-recognition receptors (like smoke detectors).
Step 2 - The Cytokine Storm
These immune cells release a flood of chemical messengers called cytokines (TNF-alpha, IL-1, IL-6, and many others). In a normal infection, this is a controlled, local response. In sepsis, it becomes a body-wide storm. Both pro-inflammatory AND anti-inflammatory signals go haywire simultaneously.
Step 3 - The Blood Vessels Go Wrong
All those cytokines and inflammatory chemicals hit the blood vessel walls (endothelium). The vessels:
- Dilate (get wider) - blood pressure drops
- Leak - fluid escapes into tissues (causing swelling and reducing blood volume)
- Become prothrombotic - tiny clots start forming in small vessels throughout the body (this is called DIC - disseminated intravascular coagulation)
Step 4 - Organs Start Failing
With dropping blood pressure, leaking vessels, and micro-clots blocking blood flow, organs start starving of oxygen:
- Kidneys: make less urine, creatinine rises (acute kidney injury)
- Lungs: fill with fluid (ARDS - acute respiratory distress syndrome)
- Brain: confusion, altered mental status
- Liver: bilirubin rises, clotting factors drop
- Heart: pump function deteriorates
- Blood: platelets fall, clotting goes out of control
Step 5 - Septic Shock
When all this progresses far enough, blood pressure crashes and the heart can't compensate even with IV fluids. This is septic shock - the most severe form, with mortality over 40%.
- Harrison's Principles of Internal Medicine 22e (2025); Schwartz's Principles of Surgery 11e
Severity Scale
Think of it as a ladder of how bad things get:
Infection (just the bug, no big problem)
↓
Sepsis (bug + organ dysfunction)
↓
Septic Shock (sepsis + blood pressure crash + elevated lactate despite IV fluids)
Under modern Sepsis-3 definitions, "severe sepsis" is no longer a separate term - if you have organ dysfunction, you already have sepsis by definition.
How Do Doctors Spot It? (Diagnosis & Scoring)
Quick Screen - qSOFA (can do it at bedside in 30 seconds, no labs needed):
Score 1 point each for:
- Altered mental status (confused, disoriented)
- Respiratory rate ≥ 22 breaths/min
- Systolic blood pressure ≤ 100 mmHg
2 or more points = high suspicion for sepsis - needs urgent evaluation.
Full Score - SOFA (Sequential Organ Failure Assessment):
Doctors use this in hospital to track organ dysfunction across 6 systems:
- Breathing (PaO2/FiO2 ratio)
- Clotting (platelet count)
- Liver (bilirubin)
- Cardiovascular (blood pressure/vasopressors)
- Brain (Glasgow Coma Scale)
- Kidneys (creatinine/urine output)
An increase of ≥ 2 points from baseline = organ dysfunction = sepsis. A SOFA score rise of 2+ correlates with ~10% in-hospital mortality.
- Schwartz's Principles of Surgery 11e; Harrison's 22e
Who Is at Risk?
Risk is higher in:
-
Elderly (mortality rates skyrocket after age 65 - up to 1037 deaths/100,000 in men ≥85 years)
-
Diabetes, obesity, cancer
-
Kidney or liver disease
-
Immunocompromised patients (chemotherapy, HIV, steroids)
-
Recent hospitalization (3x increased risk in the 90 days after any hospital stay)
-
Men have higher mortality than women at all ages
-
Harrison's Principles of Internal Medicine 22e (2025)
Treatment: The "Hours Matter" Emergency
Sepsis is treated as a medical emergency. Every hour without antibiotics in septic shock increases mortality by 7-8%.
The Core Bundle (do these FAST):
1. Antibiotics - within 1 hour of shock recognition
- Broad-spectrum IV antibiotics to cover likely organisms
- Choice depends on: site of infection, hospital vs. community origin, local resistance patterns, immune status
- Common regimens:
- If no Pseudomonas risk: ceftriaxone or cefotaxime (3rd-gen cephalosporin)
- If Pseudomonas risk: piperacillin-tazobactam, cefepime, or a carbapenem
- If MRSA risk: add vancomycin or linezolid
2. Blood cultures BEFORE antibiotics (if it won't delay treatment)
3. IV Fluids
- 30 mL/kg crystalloid (normal saline or Ringer's lactate) given rapidly for low blood pressure or high lactate
- Goal: restore circulation
4. Vasopressors (if fluids aren't enough)
- Norepinephrine is first-line
- Goal: mean arterial pressure (MAP) ≥ 65 mmHg
5. Source Control
- Find and fix the source! Drain an abscess, remove an infected catheter, take a burst appendix to surgery
- Should happen as fast as possible
6. Monitor Lactate
- Lactate > 2 mmol/L = poor oxygen delivery to tissues
- Serial measurements show whether treatment is working
7. Supportive Care
-
Oxygen/ventilation for lung failure
-
Dialysis for kidney failure
-
Blood glucose control
-
Stress ulcer and DVT prophylaxis
-
Consider hydrocortisone in refractory septic shock
-
Harrison's Principles of Internal Medicine 22e (2025), pp. 2364-2366
Epidemiology - How Common and How Deadly?
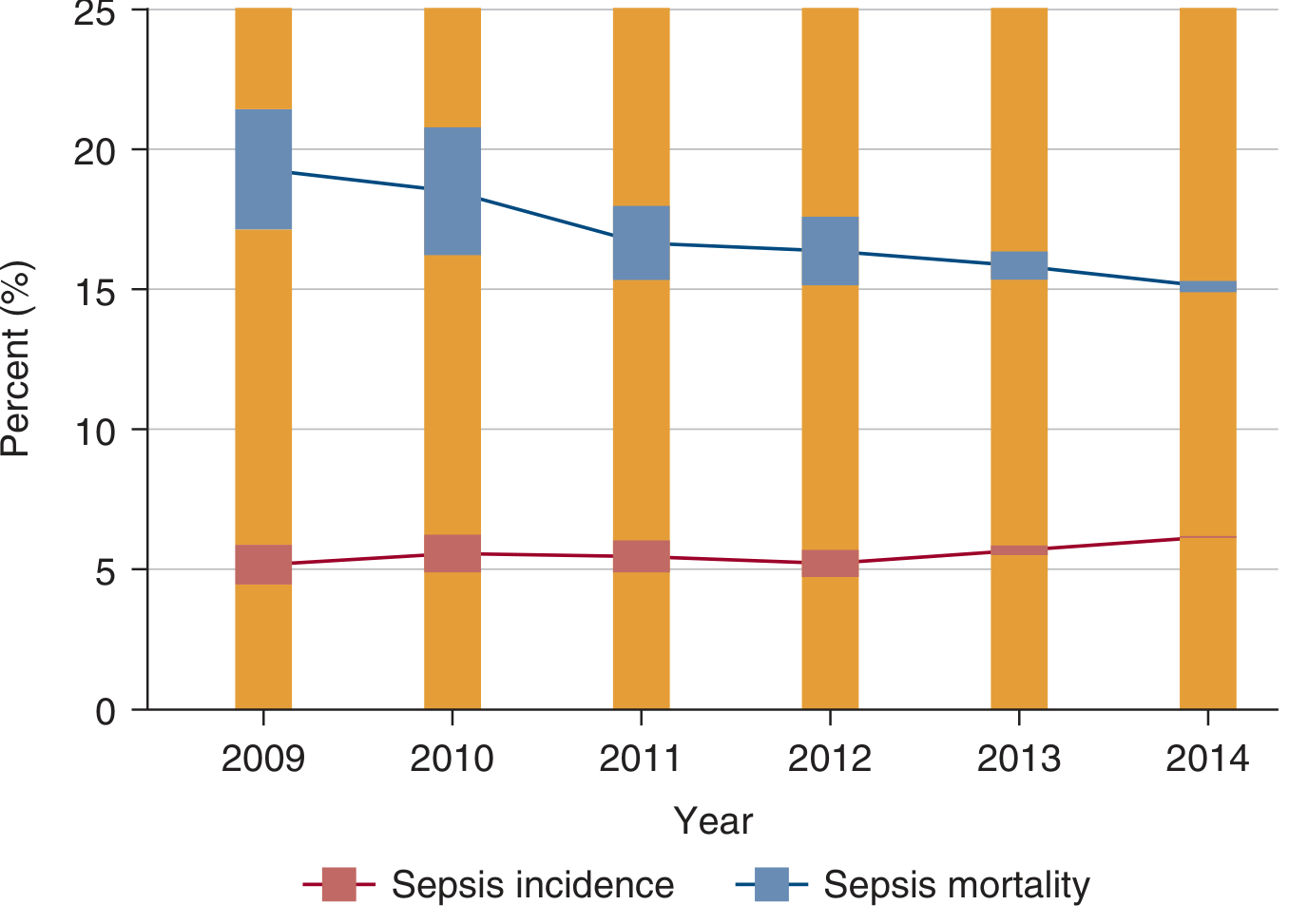
Sepsis incidence (~5-6% of hospitalizations) has remained relatively stable, while mortality has fallen from ~19% to ~15% over 2009-2014, reflecting better care bundles. - Harrison's 22e
Key numbers:
- Sepsis mortality: ~15-20% of cases
- Septic shock mortality: >40%
- Sepsis is the #1 cause of death in non-cardiac ICUs
- #11 overall cause of death in the US
- In the UK: ~200,000 adult episodes per year, ~48,000 deaths annually
- 53% of US cases are bacterial culture-positive
After Sepsis - The Long Tail
Surviving sepsis is not the end of the story. Many survivors develop post-sepsis syndrome:
- Cognitive impairment (memory, attention problems)
- Muscle weakness and fatigue
- Immune dysfunction (increased risk of future infections)
- PTSD, depression, anxiety
- 3x higher risk of developing sepsis again within 90 days
Quick Summary Table
| Feature | Details |
|---|---|
| Definition | Organ dysfunction from dysregulated immune response to infection |
| Most common cause | Bacteria (E. coli, Staph aureus, Klebsiella) |
| Most common sources | UTI, pneumonia, abdominal infection |
| Key mechanism | Cytokine storm → vascular dysfunction → organ failure |
| Screening tool | qSOFA (≥2 of: confusion, RR≥22, SBP≤100) |
| Severity score | SOFA (6 organ systems) |
| Worst form | Septic shock - >40% mortality |
| Core treatment | Antibiotics fast + fluids + vasopressors + source control |
| Time-critical | Every 1-hour delay in antibiotics = +7-8% mortality in shock |
Here's a great video that walks through everything visually, including pathophysiology, SOFA scoring, and the Sepsis 6 treatment bundle:
Sources: Harrison's Principles of Internal Medicine 22e (2025), Schwartz's Principles of Surgery 11e, Rosen's Emergency Medicine, Creasy & Resnik's Maternal-Fetal Medicine
This is a shared conversation. Sign in to Orris to start your own chat.