Latest guidelines for management of hypertension in pregnancy
Reading File
Finding Sources
Searching PubMed
"hypertension" AND "pregnancy" AND "management"
Searching the Web
hypertension in pregnancy guidelines 2024 2025 ACOG ISSHP management
Reading File
Reading File
Searching PubMed
"hypertensive disorders of pregnancy" AND "guidelines" AND "treatment"
Reading File
Finding Sources
Searching the Web
ACOG practice bulletin hypertension pregnancy 2024 2025 treatment thresholds antihypertensive drugs
Reading File
Finding Sources
Searching PubMed
"chronic hypertension" AND "pregnancy" AND "antihypertensive treatment" AND "outcomes"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
I now have comprehensive data from multiple authoritative sources. Let me compile the complete answer.
Management of Hypertension in Pregnancy - Current Guidelines
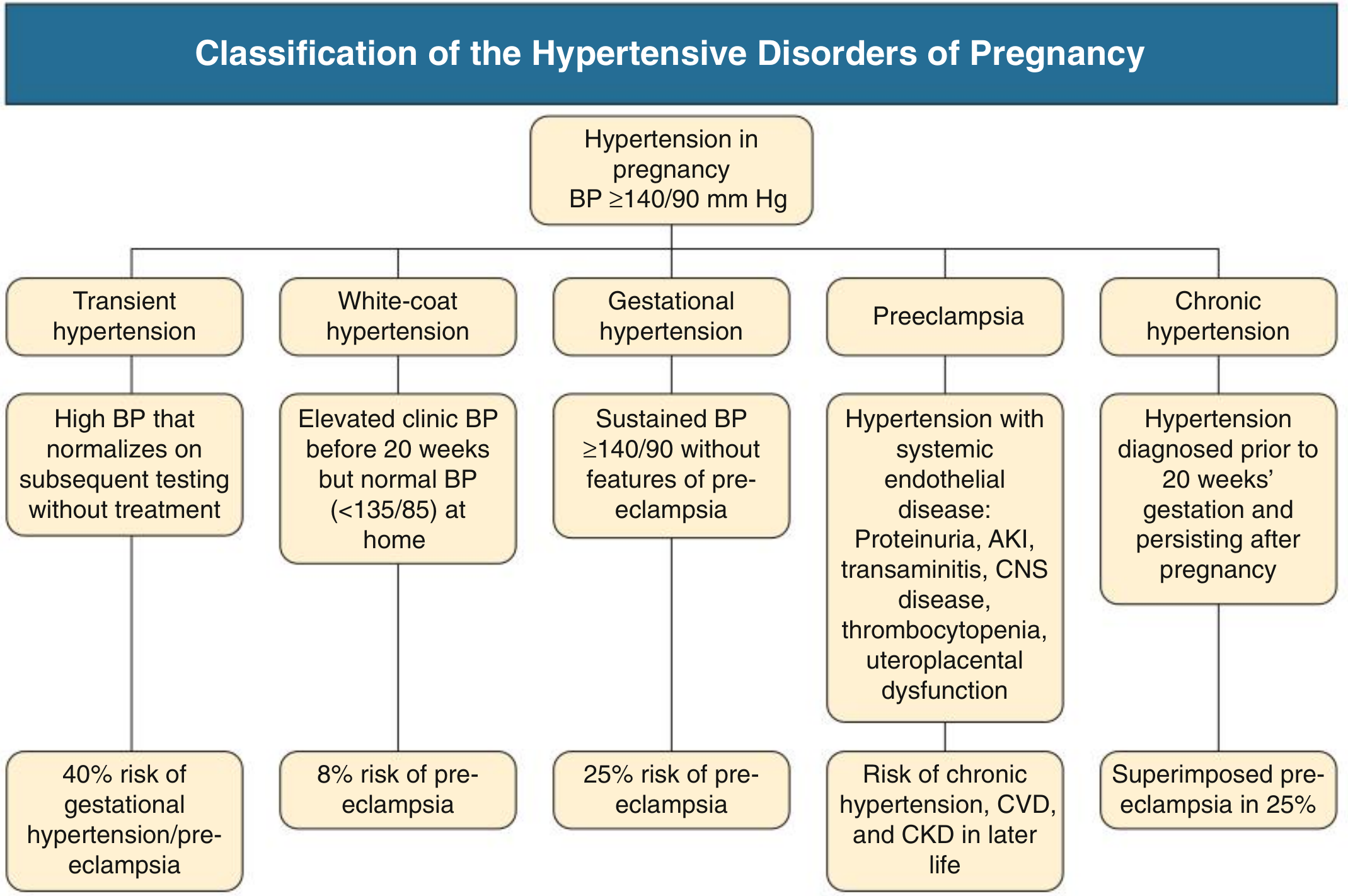
1. Classification
Hypertension in pregnancy is defined as BP ≥140/90 mmHg. The five disorders are:
| Disorder | Definition | Risk |
|---|---|---|
| Transient hypertension | BP elevation that normalizes without treatment | 40% risk of gestational HTN/preeclampsia |
| White-coat hypertension | Office BP ≥140/90, home BP <135/85 mmHg | ~8% risk of preeclampsia |
| Gestational hypertension | New-onset BP ≥140/90 after 20 weeks, no end-organ features | 25% progress to preeclampsia |
| Preeclampsia | New BP ≥140/90 after 20 weeks + proteinuria OR end-organ dysfunction | Risk of chronic HTN, CVD, CKD in later life |
| Chronic hypertension | BP ≥140/90 before 20 weeks or pre-existing; persists >12 weeks postpartum | 17-25% develop superimposed preeclampsia |
Eclampsia = preeclampsia + seizures; <0.1% incidence.
Source: Comprehensive Clinical Nephrology 7th Ed.; Fuster and Hurst's The Heart 15th Ed.
2. Preeclampsia Diagnosis (Updated Criteria)
Proteinuria is no longer required for diagnosis. Preeclampsia can be diagnosed with new hypertension after 20 weeks PLUS any one of:
- Proteinuria (uPCR >30 mg/mmol or ≥300 mg/24 h)
- AKI (creatinine ≥1 mg/dL above baseline, or ≥2x baseline)
- Thrombocytopenia (platelets ≤100,000/µL)
- Liver dysfunction (transaminases ≥2x ULN)
- Pulmonary edema
- Neurological features (severe headache, visual scotomata, seizures)
- Uteroplacental dysfunction (fetal growth restriction, abnormal umbilical artery Doppler)
Source: Comprehensive Clinical Nephrology 7th Ed., p.625-626
3. BP Treatment Thresholds - Where Guidelines Diverge
| Guideline Body | Initiation Threshold | Target |
|---|---|---|
| ACOG (US) | Gestational HTN/preeclampsia: ≥160/110 mmHg; Chronic HTN: ≥140/90 mmHg (updated 2024 recommendation per CHAP trial) | SBP 120-160, DBP 80-105 |
| NICE (UK) | >150/100 mmHg; >140/90 if target organ damage | <150/80-100 |
| ISSHP (International) | ≥140/90 mmHg for all hypertensive disorders | DBP 85 mmHg |
| Canadian (SOGC) | ≥140/90 mmHg | DBP 85 mmHg (tight control) |
Key evidence - CHIPS trial: "Tight" BP control (DBP target 85 mmHg) vs. "less-tight" (DBP 100 mmHg) found no difference in fetal harm, but tight control significantly reduced severe hypertension episodes (27.5% vs 40.6%, OR 1.80) without increasing small-for-gestational-age neonates.
CHAP trial (2022, driving 2024 ACOG update): Treating chronic hypertension at ≥140/90 mmHg reduced adverse perinatal outcomes vs. waiting for severe range BP.
Source: Brenner & Rector's The Kidney, p.2460; Comprehensive Clinical Nephrology 7th Ed., p.631; ACOG 2024
4. Antihypertensive Drug Selection
4A. Drugs Safe in Pregnancy (Oral - Chronic/Non-urgent)
| Drug | Starting Dose | Max Daily Dose | Notes |
|---|---|---|---|
| Methyldopa | 250 mg twice daily | 2000 mg | Longest safety record; sedation, rarely hemolytic anemia |
| Labetalol | 200 mg twice daily | 1200-2400 mg | Avoid in asthma, heart failure, CHF |
| Nifedipine (long-acting) | 30 mg once daily | 120 mg | Edema, headache; do NOT use sublingual form |
| Hydralazine (oral) | 50 mg three times daily | 300 mg | Tachycardia; mainly used IV for acute control |
A 2024 multicenter RCT (Sanusi et al., PMID 38949541) found no significant difference in outcomes between nifedipine and labetalol for mild chronic hypertension management.
4B. IV Drugs for Acute/Severe Hypertension (SBP ≥160 or DBP ≥110)
Goal: Treat within 30-60 minutes
| Drug | IV Dose | Notes |
|---|---|---|
| Labetalol | 20 mg IV; escalate to 40-80 mg every 10 min (max 300 mg total) | First-line; avoid in asthma, CHF |
| Hydralazine | 5-10 mg IV or IM; repeat every 20 min | Reflex tachycardia common |
| Nifedipine (oral) | 10-20 mg orally; can be used when IV access unavailable | No significant difference in efficacy vs. labetalol/hydralazine |
| Nicardipine (IV) | 5-15 mg/h infusion | Used in hypertensive crises |
| Nitroglycerin (IV) | ≤100 µg/min | Preferred when pulmonary edema coexists |
4C. Contraindicated Drugs
- ACE inhibitors - fetal renal dysplasia, oligohydramnios, pulmonary hypoplasia (especially 2nd/3rd trimester)
- Angiotensin receptor blockers (ARBs) - same as ACE inhibitors
- Atenolol - associated with fetal growth restriction
- Direct renin inhibitors - not recommended
- Spironolactone - theoretical risk of inadequate virilization of male fetuses
Source: Goodman & Gilman's Pharmacological Basis of Therapeutics; NKF Primer on Kidney Diseases 8th Ed., Table 47.1; Fuster and Hurst's The Heart 15th Ed.
5. Preeclampsia - Specific Management
5A. Severity Assessment
Severe features include: SBP ≥160, DBP ≥110 (on two readings 4 h apart), thrombocytopenia, severe headache, visual disturbances, epigastric pain, pulmonary edema, new renal/hepatic impairment.
5B. Magnesium Sulfate (Seizure Prophylaxis)
- Indicated in preeclampsia with severe features, particularly CNS involvement (clonus, severe headache, visual scotomata)
- Loading dose: 4-6 g IV over 15-20 min; maintenance 1-2 g/h infusion
- Monitor: respiratory rate, O2 saturation, reflexes, ECG
- Avoid routine serum Mg levels unless renal impairment present (dose reductions needed in CKD)
- Withholding Mg2SO4 in preeclampsia without severe features is associated with extremely low seizure risk and avoids drug toxicity (up to 25% experience toxicity)
- ~20% of eclampsia occurs >48 h postpartum - continue treatment
5C. Fluid Management
- Preeclampsia is a volume-contracted, not volume-depleted state with increased capillary permeability
- IV fluid restriction (~85 mL/h) in severe features reduces maternal morbidity and mortality
- Volume expansion is NOT warranted - high risk of pulmonary edema
- Invasive monitoring of central pressure is not indicated
5D. Platelet Transfusion (HELLP)
- Indicated for platelets <20-30 × 10⁹/L to facilitate delivery
- Avoid at higher counts - pathology is consumptive, not deficiency
- No evidence for plasma exchange or corticosteroids in HELLP syndrome
Source: Comprehensive Clinical Nephrology 7th Ed., p.631-632
6. Delivery Timing
| Situation | Recommendation |
|---|---|
| Preeclampsia ≥37 weeks | Deliver - HYPITAT trial confirmed significant maternal benefit without added perinatal risk |
| Severe features any gestational age | Deliver after maternal stabilization |
| Preeclampsia <34 weeks (without indications above) | Expectant management - balance fetal maturity vs. maternal risk |
| Preeclampsia 34-37 weeks | Individualized; delivery generally indicated |
| Mild preeclampsia ≥37 weeks | Deliver |
Indications for expedited delivery:
- Progressive end-organ dysfunction (kidney, liver, CNS, thrombocytopenia)
- Inability to control BP
- Failure of fetal growth or compromised fetal status
7. Prevention of Preeclampsia
Low-Dose Aspirin
- Recommended for all women at high risk (prior preeclampsia, chronic hypertension, diabetes types 1/2, renal disease, autoimmune conditions, multiple gestation)
- Dose: 75-150 mg/day (most guidelines use 100-150 mg)
- Start ideally before 16 weeks gestation; evidence shows 43% risk reduction when started early
- Cochrane review of 59 trials: 17% reduction in preeclampsia risk overall
- RCT (Rolnik et al.): 150 mg aspirin from 11-14 weeks in high-risk women - OR 0.38 (95% CI 0.20-0.74) for preeclampsia
Calcium Supplementation
- WHO recommends 1.5-2 g/day after 20 weeks in women with low calcium intake
- Cochrane review: ~50% reduction in preeclampsia with high-dose calcium supplementation (>1 g/day), greatest benefit in low-calcium diet and high-risk women
- Not given routinely in most high-income countries
Not Recommended
- Vitamins C and E (associated with worse outcomes)
- Fish oils, folic acid, magnesium, garlic supplements
- Anticoagulation for preeclampsia prevention alone
Source: NKF Primer on Kidney Diseases 8th Ed., p.491-492; Comprehensive Clinical Nephrology 7th Ed.
8. Postpartum Management
- BP typically improves after delivery but can worsen in the first 3-5 days postpartum
- Women with preeclampsia are at continued risk for eclampsia for at least 48-72 h postpartum
- Methyldopa should be avoided postpartum (risk of depression)
- NSAIDs should be avoided if hypertension is difficult to control postpartum
- Breastfeeding-compatible antihypertensives: nifedipine, labetalol, methyldopa
- ACE inhibitors (enalapril, captopril) are acceptable postpartum for non-breastfeeding women
- Recent RCT (Marques et al., PMID 39884047, 2025): evaluated early postpartum hypertension management
Long-Term Follow-Up
- Preeclampsia significantly increases lifetime cardiovascular risk: chronic HTN risk (RR 3.6-3.7), CVD risk, CKD
- Cardiovascular risk assessment recommended at 3 months postpartum and annually thereafter
9. Special Situations
Chronic Hypertension Pre-pregnancy Counseling
- Screen for secondary causes: renal artery stenosis, pheochromocytoma, primary hyperaldosteronism, OSA (40% of women with HTN in pregnancy have OSA by polysomnography)
- Switch to pregnancy-safe antihypertensives pre-conception
- Counsel on risks: preeclampsia, preterm birth, IUGR
Secondary Hypertension in Pregnancy
- Fibromuscular dysplasia/renovascular HTN: consider MR angiography; angioplasty has been done in 2nd/3rd trimester
- Pheochromocytoma: devastating if missed - suspect with paroxysmal severe hypertension
- Primary hyperaldosteronism: spironolactone has theoretical fetal risk; eplerenone is safer alternative
- OSA: screen high-risk women (snoring, obesity); treat with CPAP
Sources:
- Brenner and Rector's The Kidney (Comprehensive Clinical Nephrology)
- Comprehensive Clinical Nephrology, 7th Edition
- NKF Primer on Kidney Diseases, 8th Ed.
- Goodman & Gilman's The Pharmacological Basis of Therapeutics
- Fuster and Hurst's The Heart, 15th Ed.
- ACOG Practice Bulletin #203 / 2024 ACOG Annual Meeting update (CHAP trial-based)
- ISSHP 2021 Classification and Management Recommendations
- CHIPS Trial (Control of Hypertension in Pregnancy Study)
- PubMed: PMID 38949541 (nifedipine vs labetalol RCT 2024), PMID 39884047 (postpartum HTN management RCT 2025)
This is a shared conversation. Sign in to Orris to start your own chat.