Ventricular ektopic beats ???
Reading File
Finding Sources
Finding Sources
Searching PubMed
"ventricular ectopic beats"[MeSH Terms] AND management
Finding Sources
Finding Sources
Searching PubMed
"premature ventricular complexes" AND treatment
Reading File
Reading File
Reading File
Reading File
Loading Image
Now I have comprehensive material. Let me compile the full answer.
Ventricular Ectopic Beats (Premature Ventricular Contractions)
Definition & Overview
Ventricular ectopic beats - also called premature ventricular contractions (PVCs) or ventricular premature beats (VPBs) - are impulses that arise from an ectopic focus within the ventricular myocardium rather than from the sinoatrial (SA) node. They are extremely common and are often discovered incidentally on telemetry or during evaluation for palpitations. In the vast majority of cases they are benign, especially in a structurally normal heart.
Related forms of ventricular ectopy include:
- Nonsustained ventricular tachycardia (NSVT) - a run of 3 or more PVCs at <30 seconds duration
- Accelerated idioventricular rhythm (AIVR) - a slow ventricular escape rhythm (60-100 bpm), classically seen post-MI reperfusion
Mechanisms
PVCs can arise via three electrophysiological mechanisms:
- Enhanced automaticity - spontaneous phase 4 depolarization of a latent ventricular pacemaker
- Triggered activity - afterdepolarizations (early or delayed) that reach threshold, often in the setting of ischemia, hypoxia, or catecholamine excess
- Localized reentry - a micro-reentrant circuit within diseased ventricular myocardium
They are sensitive to sympathetic stimulation and can be provoked by ischemia, hypoxia, electrolyte disturbances (especially hypokalemia), or structural heart disease.
ECG Characteristics
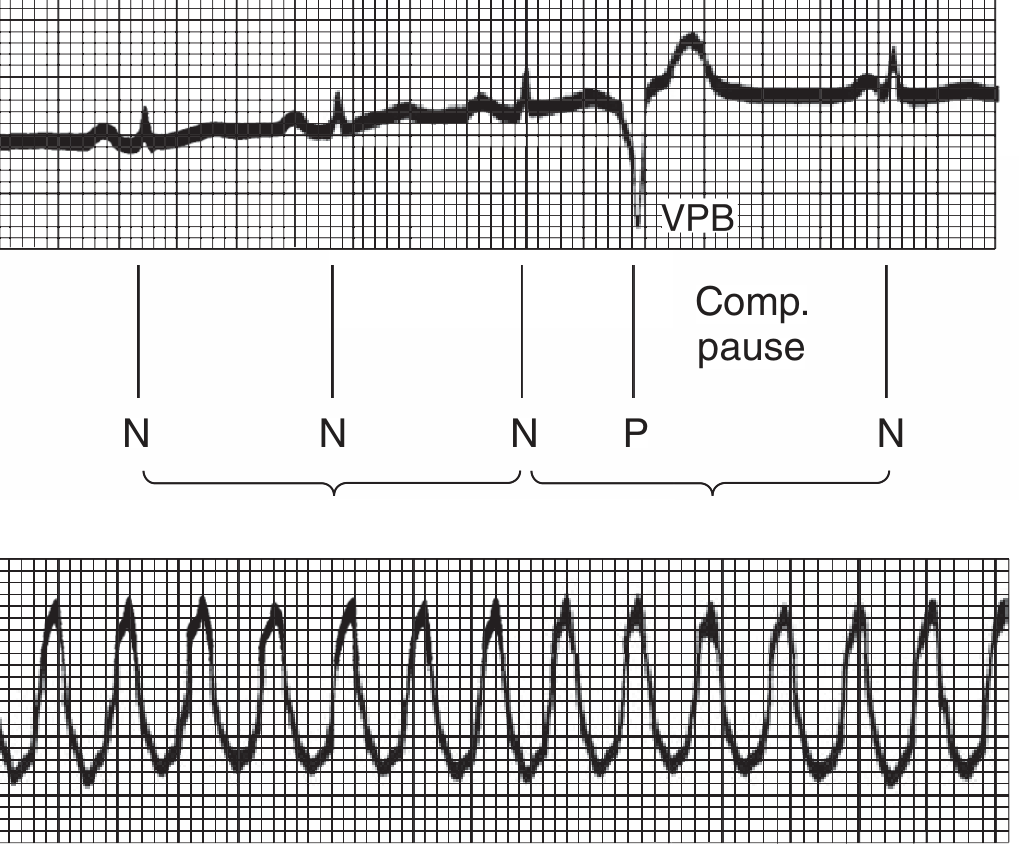
Top: Ventricular premature beat (VPB) with compensatory pause. The duration of premature beat + preceding normal beat equals two normal RR intervals. Bottom: Ventricular tachycardia.
Key ECG features:
| Feature | Description |
|---|---|
| QRS morphology | Broad, bizarrely shaped, >120 ms - due to slow cell-to-cell conduction through myocardium rather than His-Purkinje system |
| No preceding P wave | (P wave may be buried in the QRS) |
| Compensatory pause | Usually fully compensatory - the next sinus beat occurs on time but finds ventricles refractory, so a pause follows |
| Retrograde conduction | Usually absent - the VPB is "incapable of exciting the bundle of His" |
| T wave deflection | Opposite to the main QRS deflection (secondary repolarization abnormality) |
QRS Morphology as a Localising Tool
| Configuration | Origin |
|---|---|
| LBBB-like (dominant S in V1) | Right ventricle or interventricular septum |
| RBBB-like (dominant R in V1) | Left ventricle |
| Inferior axis (+ in II, III, aVF) | Cranial heart (RVOT / LVOT) - usually benign |
| Superior axis (- in II, III, aVF) | Inferior wall / diaphragmatic surface |
- Smooth, sharp QRS deflections suggest a normal myocardial substrate
- Broad, notched, slurred QRS suggests diseased myocardium
- Multifocal PVCs (multiple morphologies) strongly suggest structural heart disease or cardiomyopathy
Patterns & Terminology
| Term | Meaning |
|---|---|
| Bigeminy | Alternating normal beat - PVC - normal beat - PVC |
| Trigeminy | Every 3rd beat is a PVC |
| Couplet | Two consecutive PVCs |
| Interpolated PVC | Sandwiched between two normal beats, no compensatory pause |
| Fusion beat | Simultaneous activation from sinus + ectopic focus - intermediate QRS morphology |
| R-on-T phenomenon | PVC falls on the T wave of the preceding beat (vulnerable period) - risk of VF |
Causes / Precipitants
Cardiac:
- Myocardial ischemia / acute MI (can herald VF in peri-infarct period)
- Cardiomyopathy (dilated, hypertrophic, ARVC)
- Mitral valve prolapse / mitral annular disjunction
- Heart failure
Systemic / Metabolic:
- Hypokalemia (most common electrolyte cause)
- Hypomagnesemia
- Hypoxia
- Catecholamine excess (stress, phaeochromocytoma)
- Caffeine, alcohol, stimulants
Drugs:
- Digoxin toxicity
- Class I/III antiarrhythmics (proarrhythmia)
- Sympathomimetics
Idiopathic: Most common - especially outflow tract origin (RVOT > LVOT) in structurally normal hearts
Clinical Evaluation
Symptoms: Palpitations, "skipped beats," thudding in the chest, occasionally presyncope. Often asymptomatic.
When to investigate further:
- Symptoms are significant or exercise-related
- Abnormal 12-lead ECG (repolarization changes, prolonged QT, Brugada pattern, epsilon waves)
- Family history of sudden cardiac death
- Evidence of structural disease on examination
- High PVC burden (>10,000/24 hrs)
Investigations:
- 12-lead ECG - morphology, QT interval, ARVC/Brugada patterns
- 24-hr Holter monitor - quantify burden (PVCs/24 h), complexity (couplets, NSVT)
- Echocardiogram - LV function, wall motion, valvular disease
- Cardiac MRI - most sensitive for detecting myocardial fibrosis/scar (substrate for sustained VT), especially for ARVC
- Exercise stress test - exercise-induced PVCs, ischaemia evaluation
- Electrolytes - K+, Mg2+
PVC-Induced Cardiomyopathy
An important complication when PVCs are very frequent:
- Characterised by LV dilatation and/or systolic dysfunction
- Dose-response relationship demonstrated: >20,000 PVCs/24 h associated with subclinical reduction in LVEF; >10,000 PVCs/24 h associated with LV dilatation
- In the Cardiovascular Health Study, a high PVC burden was associated with a 3-fold greater odds of LVEF decline, 48% increased risk of incident heart failure, and 31% increased mortality
- Potentially reversible - successful catheter ablation normalises LV function in 47-100% of cases
Management
No Structural Heart Disease
| Situation | Management |
|---|---|
| Asymptomatic | Reassurance - no specific treatment needed |
| Symptomatic (mild) | Avoid triggers (caffeine, alcohol, stimulants) |
| Symptomatic (significant) | Beta-blockers or non-dihydropyridine CCBs (verapamil, diltiazem) first-line |
| Refractory to above | Membrane-active antiarrhythmics: flecainide, propafenone, mexiletine, amiodarone |
| High burden + LV dysfunction OR refractory symptoms | Catheter ablation (~90% success rate) |
Acute Illness / Hospital Setting
- Identify and correct precipitants: ischemia, hypokalemia, hypomagnesaemia, hypoxia
- Asymptomatic PVCs/NSVT in hospital do not require specific treatment beyond treating the underlying illness
Peri-Infarct (ACS Setting)
- Beta-blockers + electrolyte correction (K+, Mg2+) are the mainstay
- Prophylactic antiarrhythmics are NOT recommended; lidocaine reduces VF but increases overall mortality
Structural Heart Disease (non-ischemic cardiomyopathy, ARVC, etc.)
- Treat the underlying disease
- Beta-blockers, amiodarone for symptomatic NSVT
- ICD if meeting criteria for SCD prevention
- Ablation for frequent symptomatic PVCs or PVC-induced cardiomyopathy
Key Risk Stratification Points
- Benign indicators: Monomorphic, LBBB morphology, inferior axis, occurs at rest, suppressed with exercise, structurally normal heart
- Concerning indicators: Polymorphic, RBBB morphology, short-coupled (R-on-T), exercise-induced, family history of SCD, abnormal ECG (QT prolongation, epsilon waves, ST changes), structural heart disease, very high burden (>10,000-20,000/24 h)
Sources:
- Harrison's Principles of Internal Medicine, 22nd ed. (2025), Ch. 260 - Sauer & Tedrow
- Fuster and Hurst's The Heart, 15th ed. - PVC-Induced Cardiomyopathy
- Ganong's Review of Medical Physiology, 26th ed., Ch. 29
Recent evidence: A 2025 systematic review (PMID: 40654169) evaluated intramyocardial needle ablation for refractory ventricular tachycardia and PVCs in patients failing conventional catheter ablation, suggesting emerging options for drug-refractory cases.
This is a shared conversation. Sign in to Orris to start your own chat.