Septal Spur complete information
Reading File
Finding Sources
Finding Sources
Searching PubMed
"septal spur" nasal septum
Searching the Web
septal spur nasal complete information clinical features treatment
Reading File
Reading File
Reading Article
Searching Images
nasal septal spur anatomy endoscopic
Reading File
Loading Image
Loading Image
Loading Image
I now have comprehensive information to provide a complete answer on septal spurs. Let me compile this into a thorough clinical overview.
Septal Spur — Complete Information
Definition
A septal spur (also called a nasal septal spur) is a sharp, shelf-like projection arising from the nasal septum — composed of cartilage, bone, or a combination of both. It most commonly occurs at the bony-cartilaginous junction of the septum, where the quadrilateral cartilage meets the vomer and perpendicular plate of the ethmoid. Spurs represent an anatomical variant of the deviated nasal septum.
"A septal spur or a projection of either cartilage, bone, or a combination of both is frequently seen at the bony-cartilaginous junction." — Cummings Otolaryngology Head and Neck Surgery
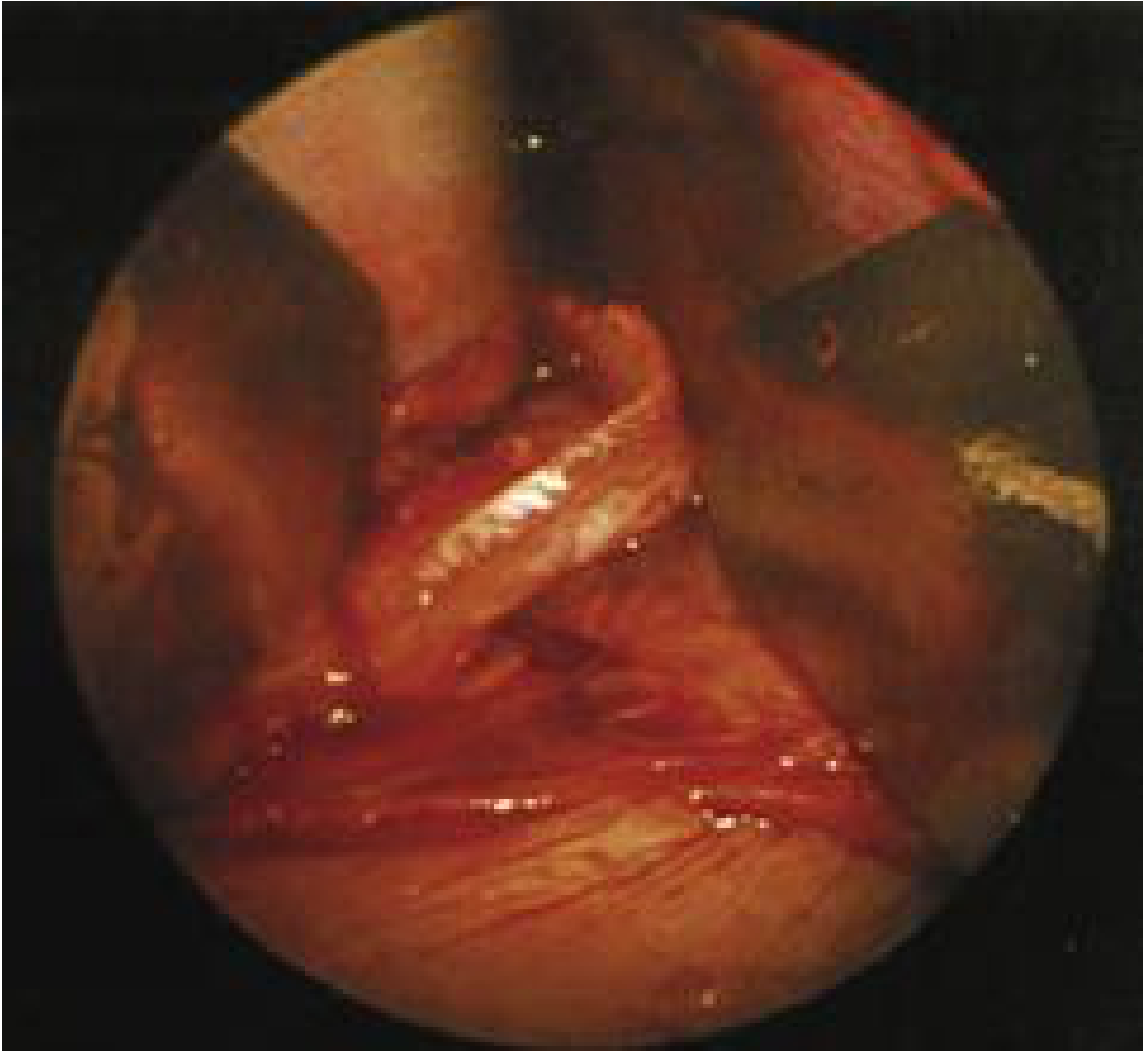
Anatomy
Endoscopic intraoperative view of a septal spur (cartilage and bone overlap at the bony-cartilaginous junction):
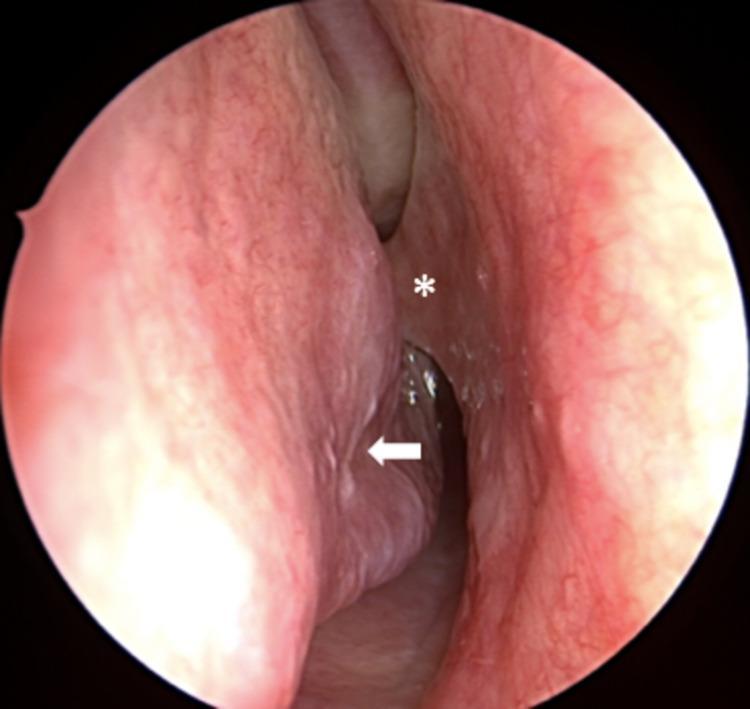
Endoscopic view: septal spur (*) impinging on inferior turbinate (arrow) in right nasal cavity:
Structural Composition
| Component | Description |
|---|---|
| Cartilaginous spur | Arising from the quadrilateral cartilage near the bony junction |
| Bony spur | From the vomer or perpendicular plate of ethmoid |
| Mixed (most common) | Cartilage-bone overlap at the bony-cartilaginous junction |
Associated Structures
- Vomeronasal cartilages — narrow cartilage strips lying between the inferior edge of the quadrilateral cartilage and the vomer — are frequently found in conjunction with a septal spur and may serve as grafting material when other cartilage sources are unavailable.
- Spurs are frequently associated with a deviated nasal septum and inferior turbinate hypertrophy on the contralateral side (compensatory).
Etiology / Pathogenesis
| Cause | Details |
|---|---|
| Traumatic | Most common — nasal trauma during childhood or adulthood causes fracture and aberrant healing at the septum-vomer junction |
| Growth-related | Unequal growth between the septal cartilage and the bony framework during puberty can cause the cartilage to buckle and spur |
| Congenital | Less common; related to abnormal fusion of medial nasal processes |
| Idiopathic | No identifiable cause in some patients |
Clinical Features
Symptoms
| Symptom | Notes |
|---|---|
| Nasal obstruction | Typically unilateral; more marked on the side of the spur; the narrowest airway is at the spur level |
| Contact-point headache / facial pain | Spur contacts the lateral nasal wall, turbinate, or floor, creating pressure-mediated pain — classically described as rhinogenic/contact-point headache |
| Epistaxis | The mucosa overlying a spur is thin and friable; prone to drying, cracking, and bleeding |
| Postnasal drip | Secondary to impaired nasal airflow and mucociliary drainage |
| Snoring / mouth breathing | Due to chronic nasal obstruction |
| Rhinosinusitis | Spur narrows the middle meatus; impairs sinus drainage; may precipitate recurrent sinusitis |
| Hyposmia | Reduced airflow over the olfactory cleft |
| Sleep-disordered breathing | Worsens in lateral decubitus position when spur-side is dependent |
Contact-Point Headache (Spur Headache)
A spur contacting the turbinate or lateral nasal wall generates rhinogenic headache — typically:
- Unilateral, periorbital, frontal or temporal in location
- Worsened by nasal congestion (e.g., in upper respiratory infections)
- Positive topical anesthetic (lidocaine) test: temporary pain relief when anesthetic applied to the contact point supports this diagnosis
- Mimics migraines or tension headaches; requires careful differentiation
Diagnosis
Clinical Examination
- Anterior rhinoscopy — Identifies gross septal deviation and visible spurs anteriorly
- Nasal endoscopy — Gold standard for visualizing posterior and superior spurs, turbinate contact, and mucosal status
- Contact points between spur and turbinate are directly visualized
- Topical anesthetic test — Lidocaine applied to the contact point; relief of headache strongly suggests rhinogenic etiology
Imaging
- CT scan of paranasal sinuses (coronal + axial views):
- Best for characterizing spur morphology (size, extent, composition)
- Identifies coexisting sinonasal anatomic variants: concha bullosa, paradoxical turbinate, etc.
- Essential preoperative planning tool
- Also identifies associated rhinosinusitis or sinus drainage obstruction
Associations / Related Conditions
| Association | Clinical Relevance |
|---|---|
| Deviated nasal septum | Spur is a variant/component of septal deviation |
| Inferior turbinate hypertrophy | Compensatory enlargement on contralateral side |
| Rhinosinusitis | Obstructs ostiomeatal complex; predisposes to recurrent sinusitis |
| Lobular capillary hemangioma | Polyp-like vascular tumors may adhere to a septal spur |
| Cleft-lip nasal deformity | Posterior nasal spur on the cleft side is a consistent feature requiring attention at septorhinoplasty |
| Contact-point headache syndrome | Spur-turbinate contact mediates facial pain via trigeminal nerve |
Surgical Management
Indications for Surgery
- Significant nasal airway obstruction not responding to medical management
- Recurrent epistaxis from the spur
- Contact-point headache with confirmed rhinogenic etiology
- Recurrent rhinosinusitis attributed to anatomical obstruction
- As part of septorhinoplasty or functional endoscopic sinus surgery (FESS)
Surgical Procedure: Septoplasty with Spur Correction
Key Steps (Cummings Otolaryngology)
- Mucosal incision — Hemitransfixion or Killian incision is made; bilateral mucoperichondrial flaps are elevated
- Flap elevation around the spur — This is the most technically demanding step:
- Mucosa overlying a spur is thin, tightly adherent, and friable
- Risk of mucosal fenestration (tear) is highest at the spur apex
- Becker septal scissors are used to make cuts in the bony septum above and below the spur to mobilize the bony deviation
- Spur removal:
- Cartilaginous component: excised or straightened
- Bony component: removed with a 4-mm curved osteotome or punch forceps
- Never manipulate the superior bony septum without a prior superior septal incision (to avoid cribriform plate injury)
- Reskeltonization — Crushed harvested cartilage is replaced into the mucoperichondrial pocket to prevent perforation and membrane flapping
- Flap re-approximation — Mattress sutures using 5-0 plain catgut on curved needle; avoids synechiae formation
Instruments Used
| Instrument | Purpose |
|---|---|
| Becker septal scissors | Bony cuts above and below the spur |
| 4-mm curved osteotome | Bony spur removal |
| Watson-Williams forceps | Cartilage removal (preferred over Jansen-Middleton — less risk) |
| No. 15 blade | Cartilage incision |
| Curved needle + 5-0 plain | Mattress suture of flaps |
CO₂ Laser Septoplasty (for small-moderate anterior spurs)
- Spur shaved with overlying mucoperichondrium in caudal-to-cephalic direction
- Only 2–3 mm vertical strip of mucoperichondrium burned
- Performed under local anesthesia in ~5 minutes
- 96% good-to-remarkable subjective improvement reported (Kamami, 1997)
- Requires controlled studies before widespread adoption
Endoscopic Septoplasty
- Literature reviews show endoscopic septoplasty achieves higher NOSE (Nasal Obstruction Symptom Evaluation) score improvement compared to conventional septoplasty
- Lower incidence of mucosal tearing
- Higher rates of complete relief from headache, hyposmia, nasal obstruction, post-nasal drip
Novel Technique: Endoscopic Septal Spur Pushback (2026)
A recently published technique specifically addresses the challenge of dissecting large and complex septal spurs:
Zhang AS et al., "The Endoscopic Septal Spur Pushback Technique." Otolaryngol Head Neck Surg. 2026. [PMID: 41353739]
Key features:
- Stepwise endoscopic approach that minimizes mucosal tension during dissection
- Leverages the endoscope's superior visualization
- In 493 consecutive patients: only 15 iatrogenic flap lacerations (3.0%), all <1 cm, none resulting in a mucosal defect at suturing
- Zero postoperative haematomas or perforations — a significant improvement over traditional approaches
Complications of Surgery
| Complication | Details |
|---|---|
| Septal perforation | Bilateral mucosal tears at same location; risk highest at spur apex |
| Haematoma | Requires drainage; prevented by mattress suturing |
| Recurrence of deviation | Incomplete correction or cartilage memory |
| Synaechiae | Adhesions between septum and turbinate; prevented by using curved needle |
| Cribriform plate injury | Rare but catastrophic; prevented by superior septal incision before posterior bone work |
| Over-resection | L-strut (≥1 cm caudal and dorsal strip) must be preserved for nasal tip and dorsal support |
| Epistaxis | Early postoperative |
| Infection | Uncommon with modern technique |
Postoperative Care
- Mattress suturing replaces nasal packing (modern best practice — avoids mucosal ischemia)
- Avoid intranasal packing or hard nasal splints
- Saline nasal irrigation for mucosal healing
- Review at 1–2 weeks for suture removal and endoscopic inspection
Key Points Summary
| Feature | Detail |
|---|---|
| Location | Bony-cartilaginous junction of nasal septum |
| Composition | Bone, cartilage, or mixed |
| Most common symptom | Unilateral nasal obstruction |
| Important complication | Contact-point headache |
| Imaging | CT paranasal sinuses |
| Treatment | Septoplasty with spur correction |
| Highest surgical risk | Mucosal tear at spur apex |
| Important preservation | L-strut (≥1 cm caudal + dorsal) |
| Latest technique (2026) | Endoscopic spur pushback — 3% tear rate, 0 perforations |
Sources:
- Cummings Otolaryngology Head and Neck Surgery, Chapters 29 (Septoplasty) and 31
- Grainger & Allison's Diagnostic Radiology — Rhinosinusitis section
- Zhang AS et al. [PMID: 41353739] — Endoscopic Septal Spur Pushback Technique, Otolaryngol Head Neck Surg 2026
This is a shared conversation. Sign in to Orris to start your own chat.