Write a note on cervical intraepithelial neoplasia
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Searching PubMed
"cervical intraepithelial neoplasia" AND management
I now have all the material needed to write a comprehensive, well-illustrated note on CIN. Here it is:
Cervical Intraepithelial Neoplasia (CIN)
1. Introduction and Historical Background
The concept of preinvasive disease of the cervix was introduced in 1947 when pathologists identified features suggestive of invasive cancer that were still confined to the epithelium. Subsequent studies showed these lesions could progress to cervical cancer if left untreated. Early terminology used the word "dysplasia" to denote malignant potential, and carcinoma in situ (CIS) was treated aggressively (often by hysterectomy). The term cervical intraepithelial neoplasia (CIN) was coined in 1968 by Richart, who proposed that dysplasias have the potential for progression through a continuous spectrum. The diagnostic criteria for CIN center on: cellular immaturity, cellular disorganization, nuclear abnormality, and increased mitotic activity - Berek & Novak's Gynecology.
2. Anatomy and Site of Origin
Normal Cervical Epithelium
The cervix is lined by two epithelial types:
- Original squamous epithelium (exocervix): four layers - basal (single row of immature cells with large nuclei), parabasal (2-4 rows of replacement cells), intermediate (4-6 rows with glycogen production), and superficial (5-8 rows of flattened cells with pyknotic nuclei - these exfoliate and form the basis of the Pap test).
- Columnar epithelium (endocervix): a single layer of mucus-secreting columnar cells with infoldings and clefts.
Squamocolumnar Junction (SCJ) and Transformation Zone
The SCJ is the boundary between squamous and columnar epithelium. Its location shifts throughout life (ectropion in reproductive years, recession into the endocervix postmenopausally). The transformation zone is the area of metaplastic squamous replacement of the original columnar epithelium, formed as metaplasia advances inward from the original SCJ. CIN characteristically originates in the transformation zone at the advancing SCJ - Berek & Novak's Gynecology.
3. Etiology and Pathogenesis
Role of HPV
HPV infection is the primary cause of cervical cancer and its precursor lesions. The cytologic changes of HPV (koilocytosis) were first recognized by Koss and Durfee in 1956. Key facts:
- Over 120 HPV types exist; ~30 infect the squamous epithelium of the lower anogenital tract.
- High-risk (oncogenic) types: HPV-16, -18, -31, -33, -35, -39, -45, -51, -52, -56, -58, -59, and -68 account for ~90% of high-grade intraepithelial lesions and invasive cancer. HPV-16 is the most common type found in invasive cancer, CIN 2, and CIN 3.
- HPV detection is associated with a 250-fold increase in risk of high-grade CIN.
- In the vast majority of cases, HPV infection clears spontaneously within 9-15 months.
Molecular Mechanism of Transformation
In low-grade lesions (CIN 1), the virus exists as an episome (extrachromosomal) in productive infection - koilocytes show perinuclear halos, nuclear hyperchromasia, and enlargement. As lesions become more severe, koilocytes disappear, HPV copy numbers decrease, and the viral DNA integrates into the host cell genome. Integration disrupts the E2 regulatory gene, leading to overexpression of E6 and E7 oncoproteins, which are essential for malignant transformation:
- E6 binds and degrades p53 (tumor suppressor)
- E7 binds and inactivates pRb (retinoblastoma protein), driving uncontrolled cell proliferation
4. Classification / Grading
CIN System
| Grade | Extent of Dysplastic Change | Bethesda Equivalent |
|---|---|---|
| CIN 1 | Dysplastic cells in lower 1/3 of epithelium; koilocytosis present | LSIL (Low-grade SIL) |
| CIN 2 | Dysplastic cells in lower 2/3 of epithelium | HSIL (High-grade SIL) |
| CIN 3 | Dysplastic cells spanning >2/3 or full thickness (CIS) | HSIL |
CIN 1 is considered a histopathologic manifestation of HPV infection rather than a true cancer precursor. CIN 2 and CIN 3 are grouped together as neoplastic precursors for the purposes of management.
The rationale for combining CIN 2 and CIN 3 into HSIL is that biologic studies show a comparable mix of high-risk HPV types, the lesions are not reproducibly distinguishable, and the management is identical.
5. Histology
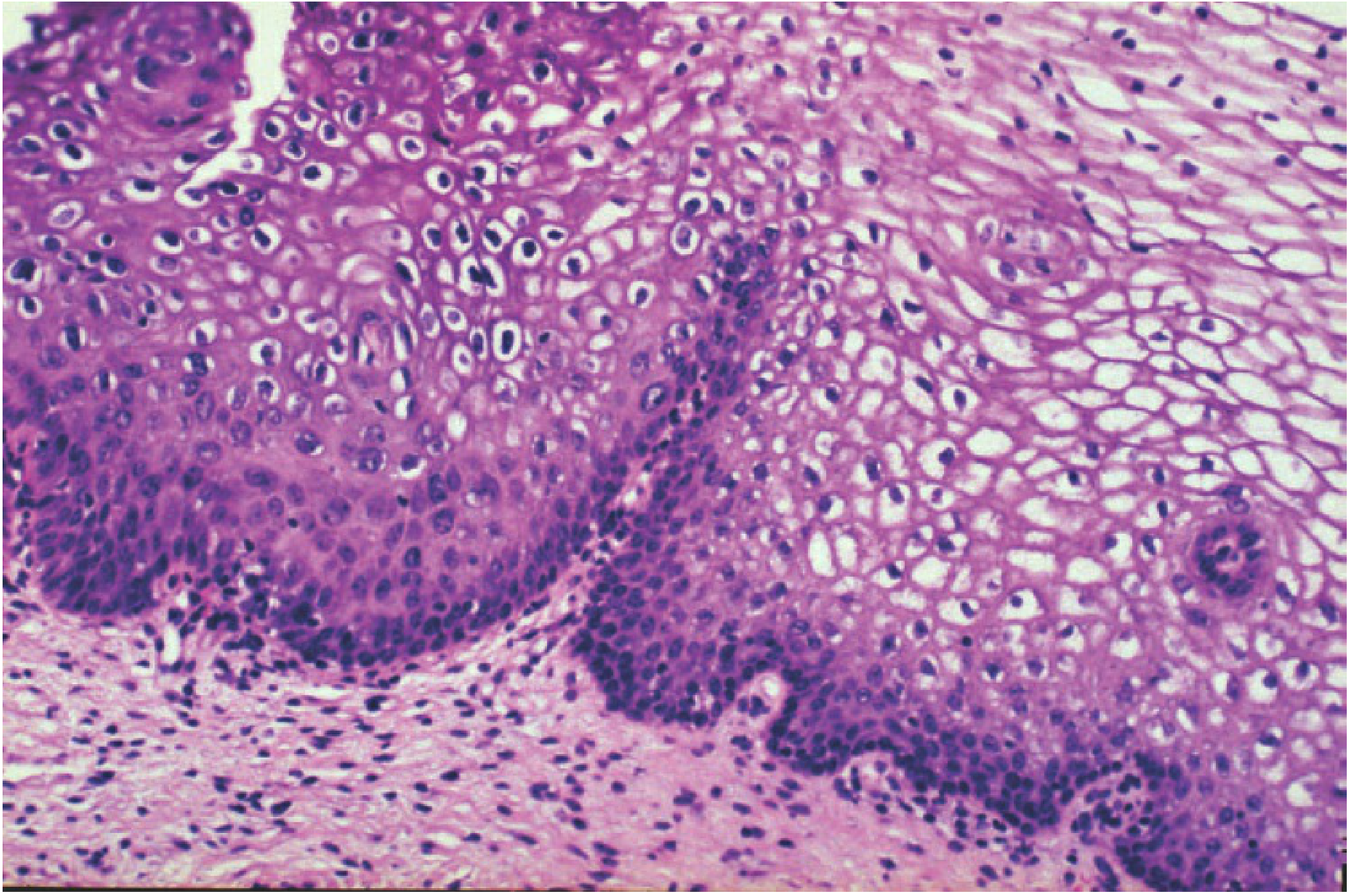
CIN 1 with koilocytosis: The normal maturation pattern is maintained. Koilocytes in the upper layers show characteristic perinuclear halos, well-defined cell borders, and nuclear hyperchromasia, irregularity, and enlargement. (Berek & Novak's Gynecology, Fig. 16-6)
Key histologic features across grades:
- CIN 1: Productive HPV infection; immature/dysplastic cells in lower 1/3; surface koilocytosis; mitoses in basal layers; maturation present in upper 2/3.
- CIN 2: Dysplastic cells extending to 2/3 thickness; increased mitoses including abnormal forms; reduced maturation.
- CIN 3/CIS: Full-thickness replacement by immature, atypical cells; near-total loss of maturation; frequent mitoses at all levels; nuclear pleomorphism.
6. Risk Factors
- Persistent high-risk HPV infection (principal risk factor)
- Early age of first intercourse
- Multiple sexual partners
- Cigarette smoking (promotes persistence of HPV)
- Immunosuppression (HIV, transplant patients - higher risk of persistence and progression)
- High parity
- Long-term oral contraceptive use
- Co-infection with other STIs (Chlamydia, HSV-2)
7. Natural History and Progression
CIN lesions may regress, persist, or progress. The probability varies by grade:
| Lesion | Regression | Persistence | Progression to CIS | Progression to Invasion |
|---|---|---|---|---|
| CIN 1 | ~60% | ~30% | ~10% | ~1% |
| CIN 2 | ~40% | ~35% | ~20% | ~5% |
| CIN 3 / CIS | ~32% | ~56% | - | ~12% |
CIN 2 progresses to CIS in ~20% of cases and to invasion in ~5%. Progression of established CIS to invasion occurs in ~5% of untreated cases - Berek & Novak's Gynecology.
8. Clinical Features
CIN is almost always asymptomatic and discovered only on screening. Occasionally, patients may have:
- Postcoital bleeding (usually indicates higher-grade lesion or early invasion)
- Abnormal vaginal discharge
9. Diagnosis
Cervical Cytology (Pap Test)
The Papanicolaou test uses exfoliated cervical cells. Liquid-based cytology (LBC) has largely replaced conventional Pap smears; LBC transfers 80-90% of cells vs. 10-20% with conventional methods and reduces unsatisfactory samples by 70-90%. Sensitivity for detecting CIN 2/3: 47-62%; specificity: 60-95%. Pap smear screening reduced cervical cancer incidence by 79% and mortality by 70% since 1950.
Bethesda System categories relevant to CIN:
- ASC-US: Atypical squamous cells of undetermined significance
- ASC-H: Atypical squamous cells, high-grade cannot be excluded
- LSIL: Low-grade squamous intraepithelial lesion
- HSIL: High-grade squamous intraepithelial lesion
HPV Testing
High-risk HPV testing:
- Triage for ASC-US cytology (identifies 90% of patients with CIN 2/3)
- Co-testing alongside cytology
- Primary screening modality (stand-alone)
- NOT appropriate for triage of ASC-H (these always go to colposcopy regardless of HPV status)
Screening Recommendations (Berek & Novak's Gynecology)
- Age <21 years: No screening regardless of sexual history
- 21-29 years: Cytology every 3 years
- 30-65 years: Co-testing (cytology + HPV) every 5 years, OR cytology alone every 3 years
- >65 years: Discontinue if documented negative history (3 negative cytologies or 2 negative co-tests in prior 10 years)
Colposcopy
Colposcopy is required for:
- Any LSIL cytology
- All HSIL cytology (with directed biopsy)
- ASC-US with positive HPV
- ASC-H
The minimum elements of a colposcopic examination include:
- Visualization of the SCJ
- Identification of acetowhitening or other lesions
- Overall colposcopic impression (normal/benign, low-grade, high-grade, cancer)
Key colposcopic findings of CIN:
- Acetowhitening: White epithelium after application of 3-5% acetic acid
- Punctation: Capillary loops appearing as red dots
- Mosaicism: Network of capillaries creating a tile-like mosaic pattern (seen in higher-grade lesions)
- Atypical vessels: Irregular vessels suggesting invasive cancer

Colposcopic image: Acetowhite lesion with mosaicism and punctation near the squamocolumnar junction, consistent with CIN 3. (Berek & Novak's Gynecology)
Colposcopic Adequacy
- Adequate/satisfactory: Entire SCJ is visible
- Inadequate/unsatisfactory: SCJ not visible (requiring endocervical sampling or excision for diagnosis)
Directed biopsy and endocervical curettage (ECC) confirm the histologic diagnosis. It is best practice for pathologists and colposcopists to jointly review cytology, molecular testing, biopsy, and ECC to formulate a management plan.
10. Management
CIN 1
- CIN 1 is not a cancer precursor but rather a manifestation of HPV infection.
- Management: Observation with cytology and/or HPV testing at 12-month intervals.
- CIN 1 preceded by ASC-H or HSIL cytology carries higher risk - co-testing at 12 and 24 months or LEEP may be more appropriate.
- For CIN 1 persisting ≥24 months: offer continued surveillance or ablation/excision.
CIN 2 and CIN 3
Women aged ≥25 years with adequate colposcopy and histologic CIN 2/3 require destruction or excision of the transformation zone.
Exceptions:
- Pregnant women: Observation with cytology/colposcopy every 12 weeks; defer treatment to 6 weeks postpartum (invasive cancer must be excluded).
- Women <25 years: Due to risk of preterm birth with excisional procedures, intensive observation with colposcopy and cytology at 6 and 12 months; if normal, co-testing in another year.
Treatment Modalities
1. Cryotherapy (Cryosurgery)
- Uses nitrous oxide or CO₂ to freeze and destroy abnormal epithelium
- Suitable for small ectocervical lesions, adequate colposcopy, negative ECC
- Cure rate ~85-90% for CIN 2/3 in appropriate cases
- Contraindicated when SCJ is not fully visualized, lesion extends into endocervix, or invasion is suspected
2. Loop Electrosurgical Excision Procedure (LEEP)
- Preferred treatment for CIN 2/3
- Thin wire loop electrode removes a cone-shaped specimen under local anesthesia
- Advantages: provides specimen for histologic diagnosis, outpatient procedure, similar long-term cure rates to cold knife conization
- Complications include: operative hemorrhage, postoperative hemorrhage, cervical stenosis, and a small but real risk of preterm birth in subsequent pregnancies
- Not appropriate if there is evidence of microinvasive or invasive cancer on cytology, colposcopy, ECC, or biopsy
3. Laser Ablation / Laser Excision
- CO₂ laser vaporizes or excises abnormal tissue
- Results comparable to LEEP in long-term studies
4. Cold Knife Conization (Conization)
Indications include:
- Limits of the lesion cannot be visualized at colposcopy
- SCJ is not evaluable
- ECC positive for CIN 2/3
- Substantial discordance between cytology, biopsy, and colposcopy
- Suspicion of microinvasion
- Inability to rule out invasive cancer
Lesions with positive cone margins are more likely to recur. Endocervical gland involvement predicts recurrence (~23.6% vs. ~11.3% without gland involvement).
5. Hysterectomy
- Treatment of last resort for recurrent high-grade CIN
- Appropriate (not mandatory) in: microinvasion, histologically confirmed recurrent high-grade CIN, or co-occurring gynecologic pathology requiring hysterectomy (fibroids, prolapse, endometriosis, PID)
- Ablative therapy is NEVER appropriate if microinvasive or invasive cancer is suspected.
Post-Treatment Surveillance
After treatment for CIN 2/3, co-testing (cytology + HPV) at 12 and 24 months is required before returning to routine age-appropriate screening.
11. CIN in Pregnancy
- Approximately 2-7% of pregnancies are complicated by an abnormal Pap test.
- Goal of evaluation: rule out invasive cancer; defer treatment for preinvasive disease until after delivery.
- Cervical dysplasia rarely progresses in pregnancy; regression is common.
- Endocervical curettage (ECC) is contraindicated in pregnancy.
- Colposcopy with biopsy is safe (complication rate ~0.6%: bleeding, infection, spontaneous abortion, preterm labor).
- For HSIL (CIN 2-3) with invasive cancer excluded: observation with cytology/colposcopy every 12 weeks; reevaluate 6 weeks postpartum.
12. Prevention - HPV Vaccination
HPV vaccines (bivalent, quadrivalent, nonavalent) targeting high-risk HPV types (especially 16 and 18) are the primary prevention strategy. Vaccination is most effective before sexual debut but may benefit sexually active individuals as well. Vaccination does not eliminate the need for regular cervical screening.
13. Key Summary
| Feature | CIN 1 | CIN 2 | CIN 3 |
|---|---|---|---|
| Epithelial involvement | Lower 1/3 | Lower 2/3 | Full thickness |
| Koilocytosis | Prominent | Less prominent | Absent |
| HPV state | Episomal (productive) | Mixed | Integrated |
| Bethesda term | LSIL | HSIL | HSIL |
| Regression rate | ~60% | ~40% | ~32% |
| Nature | HPV manifestation | Precancerous | Precancerous |
| Management | Surveillance | Excision/ablation | Excision |
Sources: Berek & Novak's Gynecology | Creasy & Resnik's Maternal-Fetal Medicine | Goldman-Cecil Medicine
Recent evidence note: A 2026 meta-analysis (PMID: 41995269) found that p16/Ki67 dual staining is superior to cytology alone for triage of HR-HPV-positive women in identifying CIN 2+/CIN 3+, supporting its use in modern triage algorithms.
This is a shared conversation. Sign in to Orris to start your own chat.