Explain in detail about lumbar pathology ...start with basic anatomy, then pathologu ..investigation with proper clinical examination..do provide the relatablr diagram and mnemonics so that it becomes easy to learn and understand
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the complete, detailed response:
Lumbar Pathology: A Complete Study Guide
Sources: Gray's Anatomy for Students, Bailey & Love's Surgery 28e, Tintinalli's Emergency Medicine, Campbell's Operative Orthopaedics 15e 2026, THIEME Atlas of Anatomy, Grainger & Allison's Diagnostic Radiology
PART 1 - BASIC ANATOMY
1.1 The Lumbar Vertebrae
The lumbar spine consists of 5 vertebrae (L1-L5), forming the lowest movable part of the vertebral column. They are the largest vertebrae in the body - a functional adaptation to bear the full body weight above.
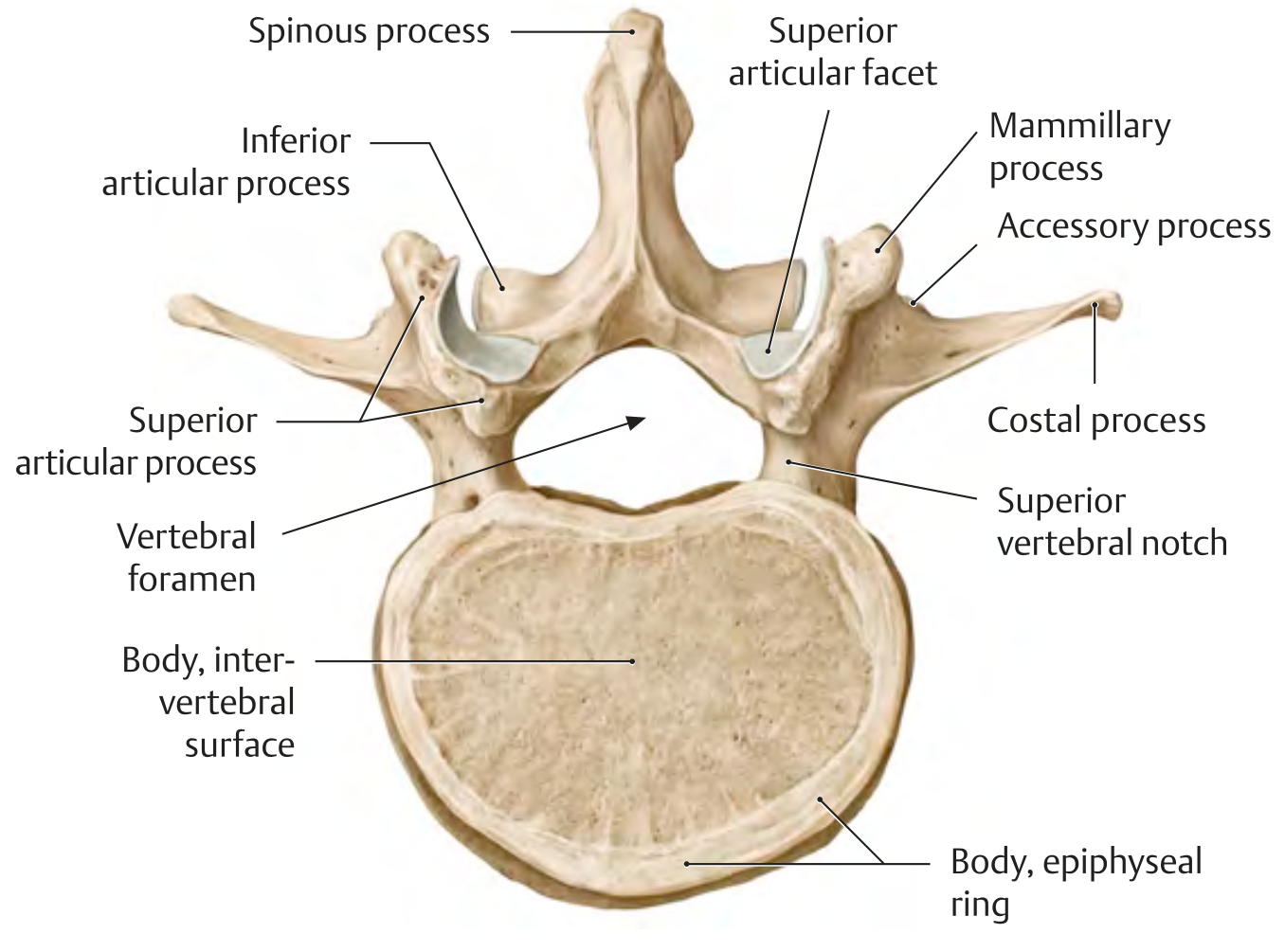
Key features of a lumbar vertebra (mnemonic: "Big Lumpy Vertebra, Strong Spinous Processes"):
| Feature | Description |
|---|---|
| Body | Large, cylindrical, kidney-shaped - increases in size from L1 to L5 |
| Vertebral foramen | Triangular (larger than thoracic) |
| Pedicles | Short and stocky, project directly posteriorly |
| Transverse processes | Long and slender (costal processes - vestigial ribs); LV has massive transverse processes for iliolumbar ligament attachment |
| Spinous processes | Large, stubby, horizontal (hatchet-shaped) - unlike cervical (bifid) or thoracic (angled down) |
| Articular facets | Oriented in sagittal plane (medially facing on superior, laterally on inferior) - promotes flexion/extension |
| Mammillary process | Small tubercle on superior articular process (unique to lumbar) |
Mnemonic for lumbar vs. other vertebrae: "Lumber is HEAVY" - Lumbar = Huge bodies, Extra-large spinous, Articular facets sagittal, V-shaped triangular foramen, Years (sagittal plane promotes flexion/extension)
1.2 Intervertebral Relationships
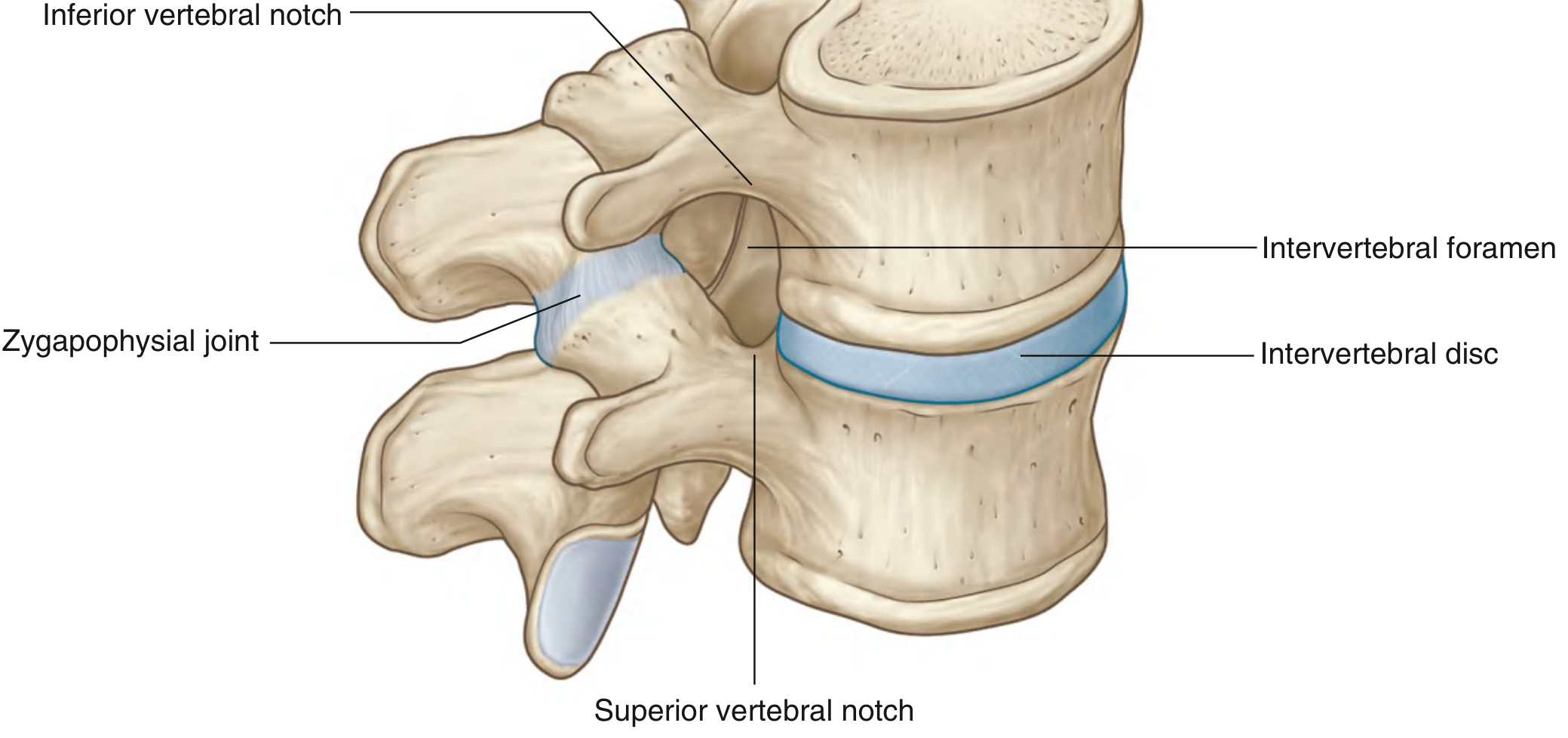
The intervertebral foramen is bounded:
- Anteriorly - intervertebral disc + adjacent vertebral bodies
- Posteriorly - zygapophysial (facet) joint
- Above and below - pedicles (superior and inferior vertebral notches)
The intervertebral disc comprises:
- Nucleus pulposus - gelatinous core (80% water in youth), high proteoglycan content
- Annulus fibrosus - concentric lamellae of fibrocartilage; posterior annulus is thinnest (site of herniation)
- Vertebral endplates - hyaline cartilage
Mnemonic for disc layers (outside in): "All Nice People Love Nucleus" Annulus fibrosus outer → Annulus fibrosus inner → Posterior Longitudinal Lig. → Nucleus pulposus
1.3 Lumbar Lordosis
The lumbar curve is a secondary (acquired) curve with anterior convexity (lordosis). It develops when the child begins to stand and walk. The lumbar lordosis increases the load-bearing efficiency and shifts the center of gravity over the feet.
1.4 Important Ligaments
| Ligament | Location | Function |
|---|---|---|
| Anterior Longitudinal Lig. (ALL) | Front of vertebral bodies | Resists extension |
| Posterior Longitudinal Lig. (PLL) | Back of vertebral bodies | Resists flexion; thinner at lumbar level (explains posterolateral herniation) |
| Ligamentum Flavum | Between laminae | Resists flexion; thickens in stenosis |
| Interspinous / Supraspinous | Between spinous processes | Resists flexion |
| Iliolumbar Lig. | L5 to ilium | Stabilizes L5-S1 junction |
Mnemonic: "ALL PLL LF IS" - ALL, PLL, Ligamentum Flavum, Interspinous/Supraspinous
1.5 Lumbar Nerve Roots - the Cauda Equina
The spinal cord ends at L1-L2 (conus medullaris). Below this, nerve roots form the cauda equina ("horse's tail"). Each nerve root exits below its corresponding vertebra (L4 root exits at L4-L5 foramen).
Posterolateral disc herniation affects the traversing (descending) root:
- L4/5 disc → compresses L5 root
- L5/S1 disc → compresses S1 root
Far-lateral (extraforaminal) herniation affects the exiting root:
- Far-lateral L5/S1 disc → compresses L5 root
Mnemonic: "Posterolateral hits the LOWER number, Far-lateral hits the UPPER number" Actually: "Poster=Traversing, Far=Exiting"
PART 2 - PATHOLOGY
2.1 Lumbar Disc Herniation (LDH)
Epidemiology:
- Affects 2-4% of the population during their lifetime
- Peak age: 30-50 years, male predominance
- >90% occur at L4/5 or L5/S1 - these two levels account for almost all clinical sciatica
Risk factors (mnemonic: "FLASH-M"):
- Family history
- Lifting heavy objects / twisting
- Age 30-50
- Stressful occupation / Smoking
- Heavy physical work
- Male gender
Pathophysiology:
- Nucleus pulposus desiccates with age (water content drops from ~90% in childhood to ~70% in adults)
- Annular fibres develop radial and circumferential tears
- Nuclear material migrates through tears
Classification of disc herniation:
| Type | Description |
|---|---|
| Bulge | Diffuse, >180° of disc circumference; annulus intact |
| Protrusion | Focal, <25% of disc circumference; annulus intact |
| Extrusion | Nuclear material breaks through annulus but connected to disc |
| Sequestration | Free fragment in canal (no longer connected to disc) |
Mnemonic: "Be-Pro-Ex-Seq" = Bad Progressively Exits the Sequester
2.2 Spinal Stenosis
Defined as narrowing of the spinal canal, nerve root canal or intervertebral foramen causing nerve root ischaemia.
Types:
- Congenital - achondroplasia, short pedicles
- Acquired (degenerative) - most common, age 50-70 years
Triple mechanism of narrowing (mnemonic: "FDL"):
- Facet joint hypertrophy
- Disc bulging
- Ligamentum flavum thickening
Classic symptom - Neurogenic Claudication:
- Back, buttock, thigh, and calf pain provoked by walking
- Worse with extension (standing, walking downhill)
- Relieved by flexion (sitting, leaning on cart - "shopping cart sign")
Neurogenic vs. Vascular Claudication (mnemonic: "SPINE vs. VEINS"):
| Feature | Neurogenic (Spinal) | Vascular |
|---|---|---|
| Walking distance | Variable (position-dependent) | Fixed |
| Posture effect | Worse in extension, better in flexion | Not affected |
| Relief | Sitting/flexion (minutes) | Stopping (seconds) |
| Pulses | Present | Absent / diminished |
| Skin changes | Absent | Present (pallor, hair loss) |
| Cycling | Comfortable | Painful |
| Uphill/downhill | Downhill worse | Uphill worse |
2.3 Spondylolysis and Spondylolisthesis
- Spondylolysis = defect in the pars interarticularis (isthmic defect), usually L5; common in gymnasts, cricketers, fast bowlers
- Spondylolisthesis = forward slippage of one vertebra on the one below
Meyerding grading of spondylolisthesis:
- Grade I: 0-25% slip
- Grade II: 25-50% slip
- Grade III: 50-75% slip
- Grade IV: 75-100% slip
- Grade V (spondyloptosis): >100%
Mnemonic: "1-2-3-4-ALL" = 25, 50, 75, 100, ALL OFF
Types (mnemonic: "I DIDN'T"):
- Isthmic (most common in young)
- Degenerative (most common in elderly, facet arthritis)
- Iatrogenic
- Dysplastic (congenital)
- Neoplastic
- Traumatic
2.4 Cauda Equina Syndrome (CES) - SURGICAL EMERGENCY
Compression of the cauda equina nerve roots, most commonly by a large central disc herniation.
Classic features (mnemonic: "BUSS"):
- Bladder dysfunction (retention is the most common; "painless urinary retention")
- Unable to control bowel (fecal incontinence)
- Saddle anesthesia (perineal/perianal numbness)
- Sexual dysfunction
Additional features: bilateral leg weakness, absent ankle jerks.
This is a surgical emergency - MRI + urgent decompression within 24-48 hours of onset.
2.5 Lumbar Spondylosis (Degenerative Disc Disease)
A spectrum of degenerative change described by Kirkaldy-Willis in three stages:
- Dysfunction phase - disc dehydration, small annular tears, facet synovitis
- Instability phase - disc height loss, ligamentous laxity, abnormal motion
- Stabilization phase - osteophyte formation, spontaneous fusion, reduced motion (often symptom relief)
Axial back pain - which should be distinguished from radicular pain - is attributed to disc degeneration but does not always cause symptoms. 80% of individuals experience back pain at some point in their lives (Campbell's Operative Orthopaedics 2026).
2.6 Ankylosing Spondylitis
- HLA-B27 associated seronegative spondyloarthropathy
- Affects sacroiliac joints first, ascending to lumbar and thoracic spine
- Bamboo spine on X-ray (syndesmophytes bridging vertebral bodies)
- Morning stiffness improved by exercise
- Schober's test used clinically
PART 3 - CLINICAL EXAMINATION
3.1 History - Red Flags (SNOOP Mnemonic)
"TUNA" for red flags in back pain:
- Trauma / fracture
- Unexplained weight loss / fever / cancer history
- Neurological deficit (saddle anaesthesia, bowel/bladder)
- Age extremes (<20 or >50 for first presentation)
Additional red flags: Night pain/rest pain, progressive neurological deficit, intravenous drug use, immunosuppression, prolonged steroid use (fracture risk).
3.2 Inspection
- Gait - antalgic gait, Trendelenburg sign
- Posture - loss of lumbar lordosis (muscle spasm), scoliosis
- List - lateral lean away from the painful side (in disc herniation)
- Skin - café-au-lait spots (NF), hairy patches/pits (spina bifida occulta), bruising
3.3 Palpation
- Palpate midline spinous processes for step-off (spondylolisthesis), point tenderness (fracture, infection)
- Percuss vertebral bodies - point tenderness to percussion suggests fracture or infection
- Paraspinal muscle spasm
- Sacroiliac joint tenderness (FABER/FADIR tests)
3.4 Movement Assessment
| Movement | Normal Range | Relevant Pathology |
|---|---|---|
| Flexion | 90° (touch toes) | Disc herniation - pain increased |
| Extension | 30° | Stenosis - pain increased; facet arthritis |
| Lateral flexion | 30° each side | Asymmetry suggests pathology |
| Rotation | 30° each side | Facet joint disease |
Schober's Test (for lumbar flexion):
- Mark midpoint of posterior superior iliac spine (dimples of Venus)
- Mark 10 cm above and 5 cm below
- On full forward flexion, distance should increase from 15 cm to at least 20 cm
- <20 cm suggests ankylosing spondylitis or severe restriction
3.5 Neurological Tests - The Core Examination
Straight Leg Raise (SLR) / Lasegue's Test
With the patient supine, passively raise the affected leg (knee straight):
- Positive: radicular pain radiating below the knee when leg raised between 30-70°
- Worsened by ankle dorsiflexion (Bragard's sign)
- Improved by ankle plantar flexion or knee flexion
- Gluteal/hamstring pain is not a positive result (that is tight hamstrings)
Sensitivity: 68-80% for L4/L5 or L5/S1 disc herniation
Crossed SLR: Raising the asymptomatic leg causes pain in the symptomatic leg - highly specific but insensitive for nerve root compression
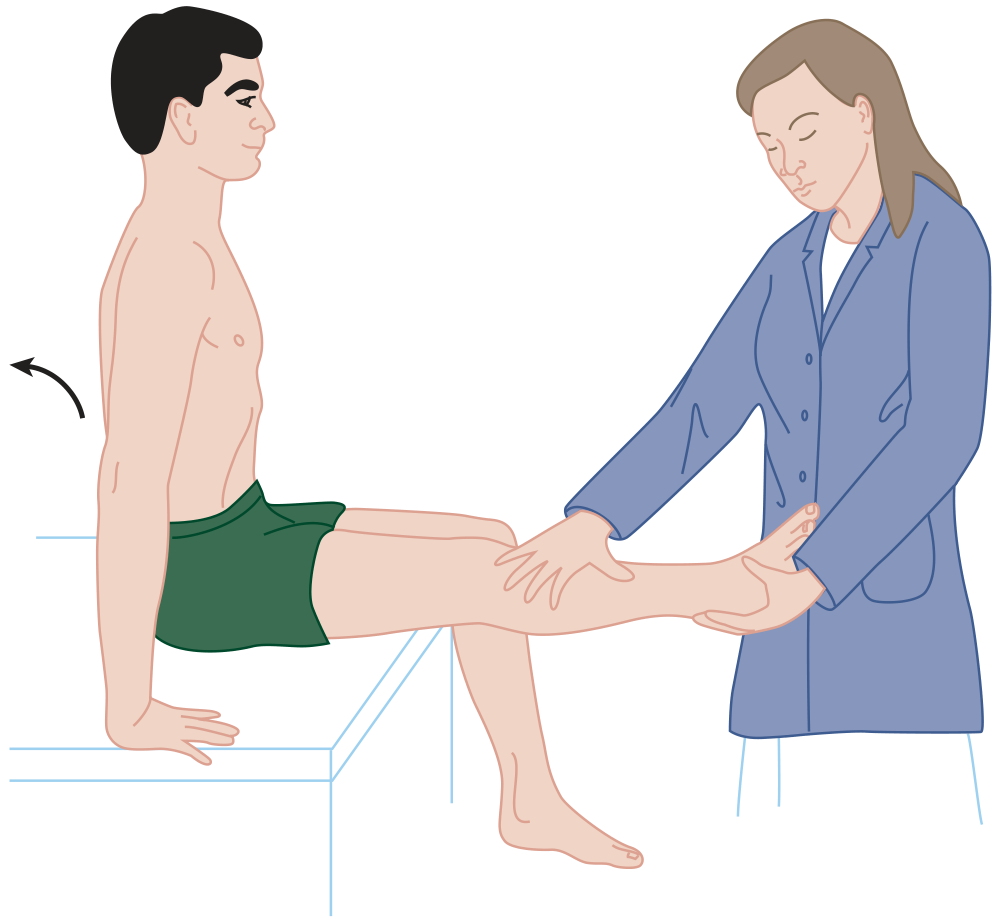
The sitting knee extension test replicates the SLR in the seated position and is harder to fake.
Femoral Stretch Test (Reverse SLR)
Patient prone, passively flex the knee - stretches L2, L3, L4 roots. Positive if pain radiates down anterior thigh.
3.6 Dermatomal / Myotomal Examination
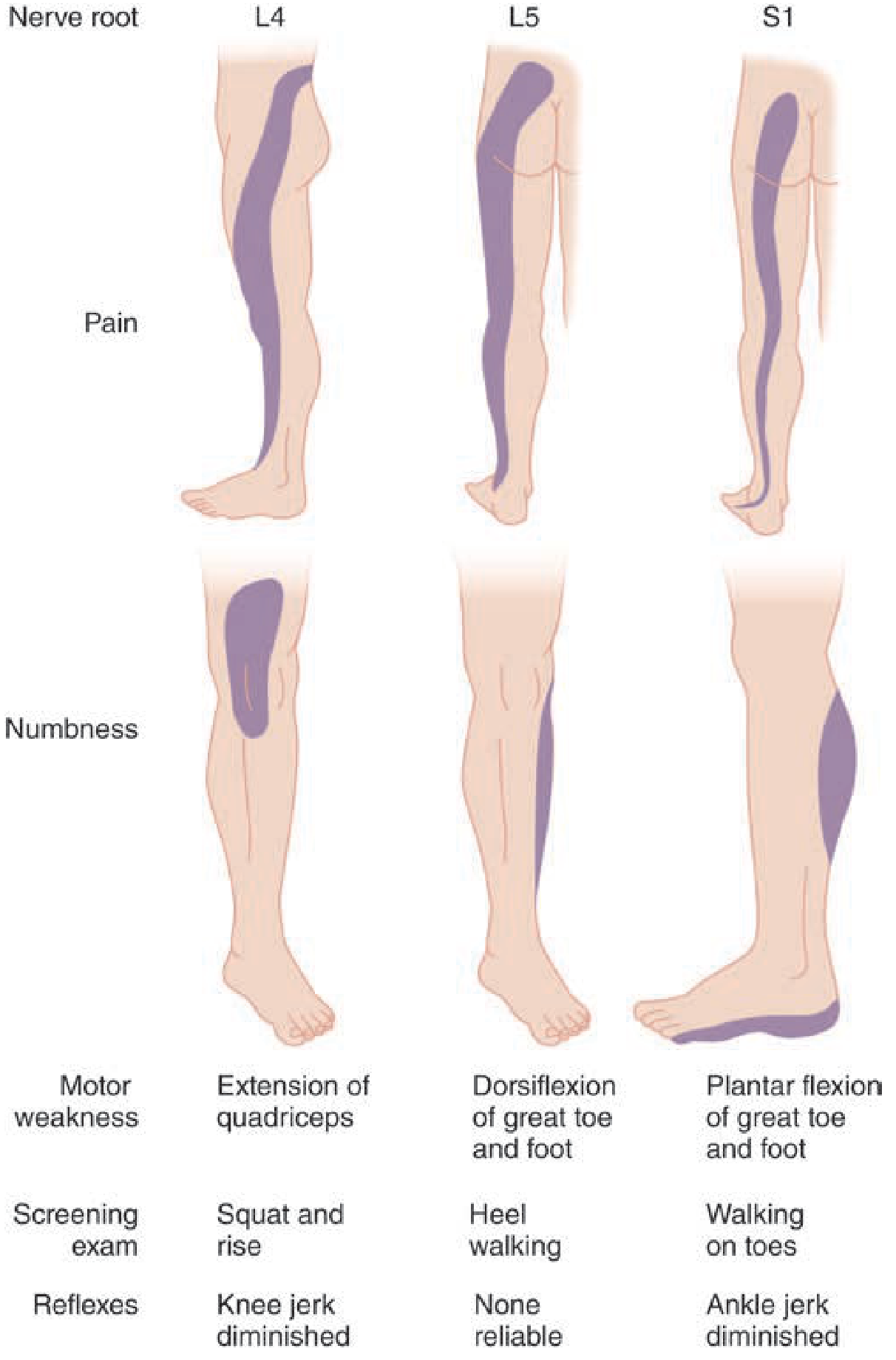
| Root | Dermatome (Pain/Numbness) | Motor | Reflex | Screening Test |
|---|---|---|---|---|
| L3 | Anterior thigh, medial knee | Knee extension (quad) | Knee jerk (partial) | Squat |
| L4 | Medial calf | Knee extension, ankle dorsiflexion | Knee jerk ↓ | Squat and rise |
| L5 | Lateral calf, dorsum foot, great toe | Great toe + foot dorsiflexion (EHL) | No reliable reflex | Heel walking |
| S1 | Lateral/plantar foot, heel | Plantar flexion, toe flexion | Ankle jerk ↓ | Toe walking |
| S2-4 | Perianal, perineum (saddle) | Sphincter tone | Anal wink | Rectal exam |
Mnemonic for L4/L5/S1 reflexes: "Kneel, Nothing, Ankle" L4 = Knee jerk | L5 = Nothing | S1 = Ankle jerk
Mnemonic for walking tests: "Heel = L5, Toe = S1" (Heel walking tests dorsiflexion = L5; Toe walking tests plantar flexion = S1)
3.7 Special Tests Summary
| Test | What it tests | How to do it | Positive result |
|---|---|---|---|
| SLR (Lasegue) | L4/5, L5/S1 root | Supine; raise extended leg | Radicular pain <70° |
| Crossed SLR | Same | Raise asymptomatic leg | Pain in affected leg |
| Bragard's | Confirms SLR | Add ankle dorsiflexion | Worsening of SLR pain |
| Femoral stretch | L2-L4 root | Prone; flex knee | Anterior thigh pain |
| Schober's | Lumbar mobility | Mark + flex | <20 cm = restricted |
| FABER/Patrick | SI joint / hip | Figure-4 position, press | Groin/SI pain |
| Slump test | Neural tension | Sitting slump + SLR | Radicular pain |
| Waddell's signs | Non-organic pain | 5 signs | ≥3 = non-organic component |
PART 4 - INVESTIGATIONS
4.1 Plain X-Ray (First-Line)
What to look for:
- Disc space narrowing (degeneration)
- Osteophyte formation (spondylosis)
- Vertebral body alignment (spondylolisthesis - lateral view)
- Pars defect (oblique view - "Scotty dog" sign with collar = spondylolysis)
- Fractures, compression fractures
- Bone density changes (metastases, osteoporosis)
Scotty Dog sign (oblique view):
- Nose = transverse process
- Eye = pedicle
- Ear = superior articular process
- Front leg = inferior articular process
- Body = lamina
- Collar around neck = pars interarticularis defect (spondylolysis)
Mnemonic for Scotty Dog: "NEEFBL" - Nose, Eye, Ear, Front leg, Body, Leash (collar = pars defect)
4.2 MRI (Gold Standard)
Indications for urgent MRI:
- Cauda equina syndrome (emergency)
- Progressive neurological deficit
- Red flag symptoms
- Failure of conservative treatment (>6 weeks for sciatica)
What MRI shows:
| Sequence | Finding |
|---|---|
| T1 | Anatomy, fat (bright), bone marrow |
| T2 | Water content (discs appear bright if hydrated; dark = degenerate) |
| STIR | Bone marrow edema (infection, fracture, spondylitis) |
| Gadolinium | Post-surgical scarring vs. recurrent disc (enhances scar but not disc) |
Important caveat: Incidental disc herniations are found on MRI in 20-36% of asymptomatic individuals - always correlate with clinical findings.
4.3 CT Scan
- Better for bony pathology (fractures, facet joints, pars defects)
- CT myelogram: if MRI contraindicated (pacemaker), shows thecal sac compression
- Used for surgical planning
4.4 Electrodiagnostic Studies (EMG/NCS)
- EMG: detects denervation in specific muscle groups - confirms root level, rules out peripheral neuropathy
- NCS: normal in radiculopathy (lesion is proximal to sensory ganglion); abnormal in peripheral neuropathy
- Useful when clinical picture is unclear or to distinguish radiculopathy from neuropathy
4.5 Blood Tests
| Investigation | Indication |
|---|---|
| ESR, CRP | Infection, ankylosing spondylitis, neoplasm |
| FBC | Anemia (metastases), leucocytosis (infection) |
| HLA-B27 | Ankylosing spondylitis (90% positive) |
| PSA | Prostate metastases |
| Serum/urine protein electrophoresis | Myeloma |
| ALP | Bone disease (Paget's, metastases) |
| PTH, Vitamin D, Calcium | Osteoporosis workup |
4.6 Bone Scan (Radionuclide Scintigraphy)
- Detects stress fractures (active pars defect in spondylolysis), metastases, infection
- SPECT scan improves sensitivity for pars defects
PART 5 - MANAGEMENT OVERVIEW
Conservative (First-Line for Most)
Mnemonic: "PEACE & LOVE" (modern guideline-based approach)
- Protect, Elevate, Avoid anti-inflammatories early, Compress, Educate
- Load, Optimism, Vascular care, Exercise
- NSAIDs, analgesics (paracetamol, tramadol)
- Physiotherapy, exercise (not bed rest - harmful)
- Pregabalin/gabapentin for neuropathic pain
- Transforaminal epidural steroid injections (for persistent sciatica >6 weeks)
- 90% of patients with sciatica return to work by 3 months
Surgical Indications
| Condition | Procedure |
|---|---|
| Disc herniation (failed conservative 6-12 wks) | Microdiscectomy |
| Spinal stenosis (severe symptoms) | Laminectomy / decompression |
| Spondylolisthesis (Grade III-IV or symptomatic) | Spinal fusion |
| Cauda equina syndrome | Emergency decompression |
MASTER SUMMARY TABLE
| Condition | Typical Age | Key Symptom | Special Test | Imaging | Rx |
|---|---|---|---|---|---|
| Disc herniation | 30-50 | Sciatica, worse flexion | +ve SLR | MRI disc herniation | Conservative → Microdiscectomy |
| Spinal stenosis | 50-70 | Neurogenic claudication, worse extension | Negative SLR usually | MRI canal narrowing | Conservative → Decompression |
| Spondylolisthesis | Young athletes (isthmic) | Back pain ± sciatica | Step-off on palpation | Lateral X-ray, CT | Conservative → Fusion |
| Cauda equina syndrome | Any | Saddle anaesthesia, retention | Absent anal wink | MRI (emergency) | Emergency surgery |
| Ankylosing spondylitis | <40 | Morning stiffness, bilateral SI pain | Schober's <20 cm | MRI SI joints, X-ray | NSAIDs, biologics |
QUICK REVISION MNEMONICS
| Topic | Mnemonic |
|---|---|
| Red flags in back pain | TUNA (Trauma, Unexplained weight loss, Neurological deficit, Age extremes) |
| Disc herniation risk | FLASH-M (Family, Lifting, Age, Stress, Heavy work, Male) |
| Stenosis narrowing causes | FDL (Facet hypertrophy, Disc bulge, Ligamentum flavum) |
| Neurogenic vs vascular | Neurogenic = position-dependent, pulses present, cycling OK |
| L4/L5/S1 reflexes | "Kneel, Nothing, Ankle" |
| Walking tests | "Heel = L5, Toe = S1" |
| Cauda equina | BUSS (Bladder, Unable to control bowel, Saddle anaesthesia, Sexual dysfunction) |
| Spondylolisthesis grades | 25-50-75-100 percent slippage |
| Scotty dog sign | Collar = pars defect (spondylolysis) |
Sources: Gray's Anatomy for Students (Elsevier), Bailey & Love's Surgery 28e, Tintinalli's Emergency Medicine, Campbell's Operative Orthopaedics 15e 2026, THIEME Atlas of Anatomy, Grainger & Allison's Diagnostic Radiology
This is a shared conversation. Sign in to Orris to start your own chat.