Common Congenital heart disease in pediatrics .. answer for saq in mbbs exam 7 marks ..refer book o.p. ghai
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
Loading Image
I now have everything needed for a thorough, exam-ready 7-mark SAQ answer. Here it is:
Common Congenital Heart Diseases in Pediatrics
(O.P. Ghai Essential Pediatrics - aligned answer; supplemented with Robbins & Kumar Basic Pathology)
Definition & Overview
Congenital heart diseases (CHD) are structural abnormalities of the heart or great vessels present at birth. Incidence: ~8-10 per 1000 live births. They account for ~20-30% of all birth defects.
Classification:
| Category | Examples |
|---|---|
| Acyanotic (L→R shunt) | VSD, ASD, PDA |
| Acyanotic (Obstructive) | Pulmonary stenosis, Aortic stenosis, Coarctation of aorta |
| Cyanotic (R→L shunt) | Tetralogy of Fallot, Transposition of Great Arteries |
Frequency Table (Robbins & Kumar)
| Malformation | Frequency |
|---|---|
| VSD | 42% |
| ASD | 10% |
| Pulmonary stenosis | 8% |
| PDA | 7% |
| Tetralogy of Fallot | 5% |
| Coarctation of aorta | 5% |
Left-to-Right Shunt Defects (Acyanotic)
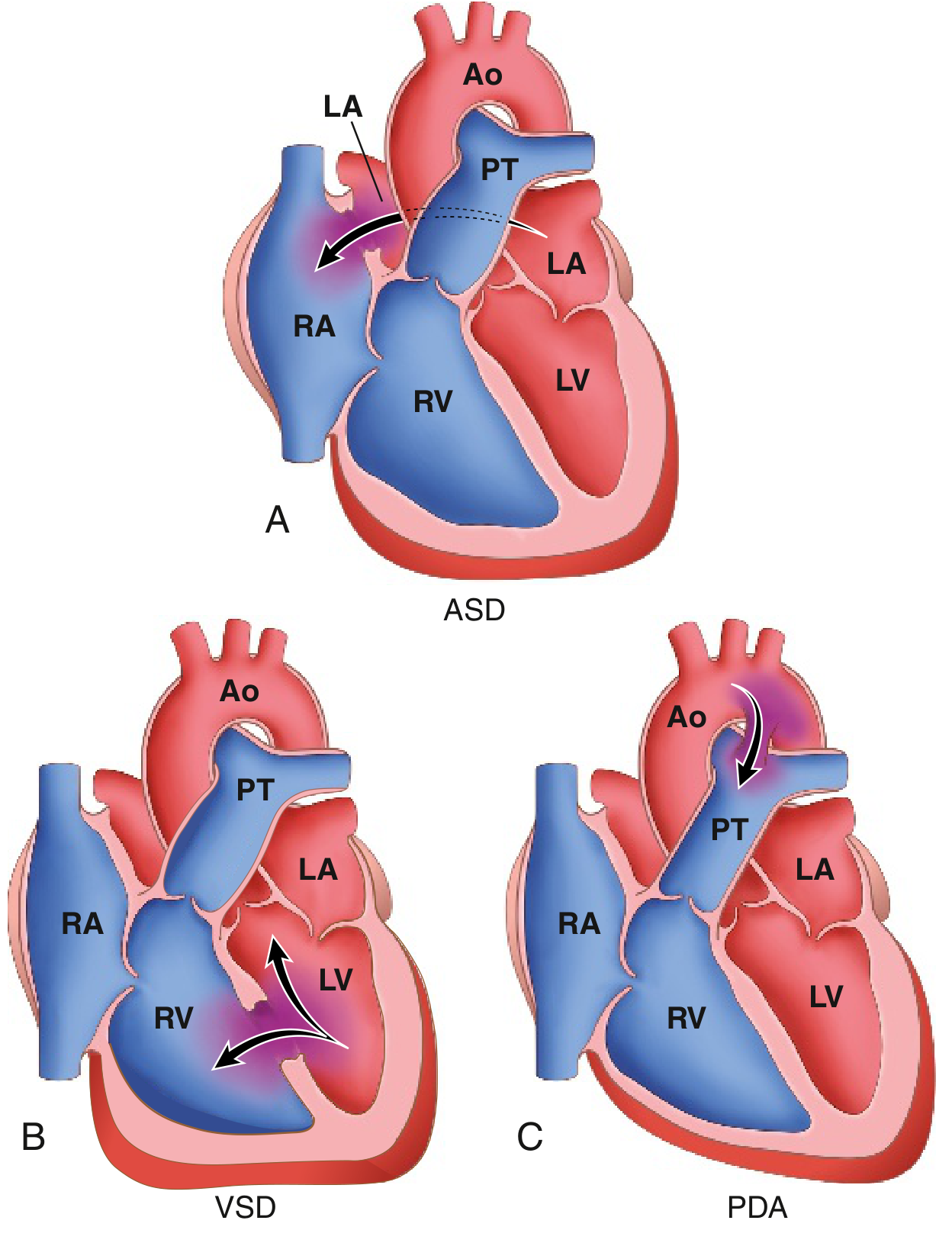
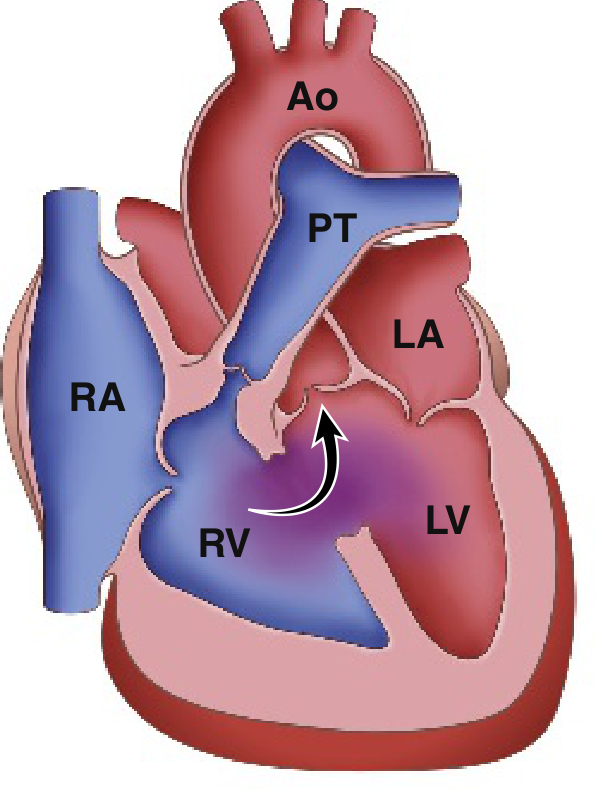
1. Ventricular Septal Defect (VSD) - Most common CHD (~42%)
Pathology:
- Defect in the interventricular septum - most commonly in the membranous (perimembranous) portion (90%)
- Allows left-to-right shunting due to higher LV pressure
Clinical Features:
- Small VSDs: asymptomatic; pansystolic murmur at left lower sternal border; may close spontaneously in childhood
- Large VSDs: recurrent chest infections, failure to thrive, congestive heart failure (CHF), pulmonary hypertension
- Loud harsh pansystolic murmur with thrill at 3rd-4th left intercostal space
Complications:
- Pulmonary hypertension
- Eisenmenger syndrome (shunt reversal - late cyanosis)
- Infective endocarditis (risk)
Treatment: Small VSDs - observe; large VSDs - surgical closure or catheter-based device closure
2. Atrial Septal Defect (ASD) - ~10%
Types:
- Ostium secundum (most common, ~70%) - mid-septal
- Ostium primum - lower septum, associated with AV canal defects
- Sinus venosus - near SVC/IVC junction
Pathology: LA→RA shunting; right atrium and ventricle dilate; pulmonary blood flow increases
Clinical Features:
- Often asymptomatic in childhood (well tolerated)
- Wide, fixed split S2 (hallmark)
- Soft systolic ejection murmur at pulmonary area (due to increased flow across pulmonary valve)
- Recurrent respiratory infections, fatigue, exercise intolerance in larger defects
Complications: Pulmonary hypertension, arrhythmias (AF), Eisenmenger syndrome (late)
Treatment: Device (transcatheter) closure or open-heart surgery
3. Patent Ductus Arteriosus (PDA) - ~7%
Pathology:
- Failure of the ductus arteriosus to close after birth (normally closes within 1-2 days by increased O2 tension + falling prostaglandin E2)
- High-pressure aorta→pulmonary artery shunting (left-to-right)
- Common in premature infants and with rubella infection
Clinical Features:
- Continuous "machinery-like" murmur, best heard at left infraclavicular area (Gibson murmur)
- Wide pulse pressure, bounding pulses
- Larger PDAs: CHF, pulmonary hypertension
Treatment:
- Premature neonates: Indomethacin (prostaglandin synthesis inhibitor) to promote closure
- Term infants/children: Surgical ligation or catheter-based device closure
Right-to-Left Shunt Defects (Cyanotic)
4. Tetralogy of Fallot (TOF) - Most common CYANOTIC CHD (~5%)
Four cardinal features (mnemonic: PROVE or RVOP):
- VSD (large, perimembranous)
- Right ventricular outflow tract obstruction (subpulmonic/infundibular stenosis)
- Overriding aorta (aorta straddles the VSD)
- Right ventricular hypertrophy
All four result from anterosuperior displacement of the infundibular septum during development.
Clinical Features:
- Cyanosis from birth or early infancy (central cyanosis)
- Clubbing of fingers/toes (chronic hypoxia)
- Polycythemia
- Hypercyanotic ("Tet") spells - acute episodes of severe cyanosis, irritability, breathlessness; child squats to relieve (squatting increases SVR, decreases R→L shunt)
- "Boot-shaped" heart on X-ray (coeur en sabot) - due to RV hypertrophy + small pulmonary trunk
- Right ventricular hypertrophy on ECG
- Systolic ejection murmur (pulmonary stenosis)
Management of Tet spell: Knee-chest position, O2, morphine, IV beta-blockers (propranolol), IV fluids
Definitive treatment: Total surgical correction (VSD closure + relief of RVOT obstruction)
5. Coarctation of Aorta (~5%)
Types:
- Preductal (infantile form): narrowing proximal to ductus - presents early in life with cyanosis in lower body, severe CHF
- Postductal (adult form): discrete narrowing adjacent to ligamentum arteriosum - often asymptomatic until adulthood
Clinical Features:
- Upper limb hypertension with weak/absent femoral pulses (radio-femoral delay)
- Blood pressure difference between upper and lower limbs (>20 mmHg)
- Rib notching on chest X-ray (due to dilated collateral intercostal arteries - seen after ~5 years)
- Systolic murmur between shoulder blades
Associations: Bicuspid aortic valve (50%), Turner syndrome
Treatment: Balloon dilation + stenting or surgical resection with end-to-end anastomosis
Key Associations to Remember
| Feature | Condition |
|---|---|
| Maternal rubella | PDA, pulmonary stenosis, ASD |
| Down syndrome (Trisomy 21) | AV canal defect, VSD |
| Turner syndrome | Coarctation of aorta, bicuspid aortic valve |
| DiGeorge syndrome | Truncus arteriosus, TOF |
| Marfan syndrome | Aortic root dilation, MVP |
| Eisenmenger syndrome | Any large L→R shunt with pulmonary HTN reversal |
Summary Diagram
Acyanotic → Cyanotic conversion:
L→R shunt → pulmonary hypertension → shunt reversal (R→L) → Eisenmenger syndrome (irreversible - contraindication to surgical repair)
Sources: Robbins & Kumar Basic Pathology (9th ed., pp. 347-351); O.P. Ghai Essential Pediatrics (8th ed.) - standard MBBS pediatrics reference for classification, clinical features, and management
This is a shared conversation. Sign in to Orris to start your own chat.