Pulmonary tb
Reading File
Finding Sources
Finding Sources
Searching PubMed
"pulmonary tuberculosis"[MeSH Terms] AND treatment
Reading File
Reading File
Searching PubMed
tuberculosis[MeSH Terms] AND treatment
Reading File
Reading File
Reading File
Loading Image
I now have comprehensive information to compile a detailed, well-structured answer on Pulmonary TB. Let me deliver it.
Pulmonary Tuberculosis (Pulmonary TB)
Overview
Pulmonary TB is caused by Mycobacterium tuberculosis, an aerobic, acid-fast bacillus transmitted via respiratory droplet nuclei. It is the most common form of TB disease and the leading infectious cause of death worldwide. The lungs are the primary site of infection, but the bacterium can disseminate to virtually any organ.
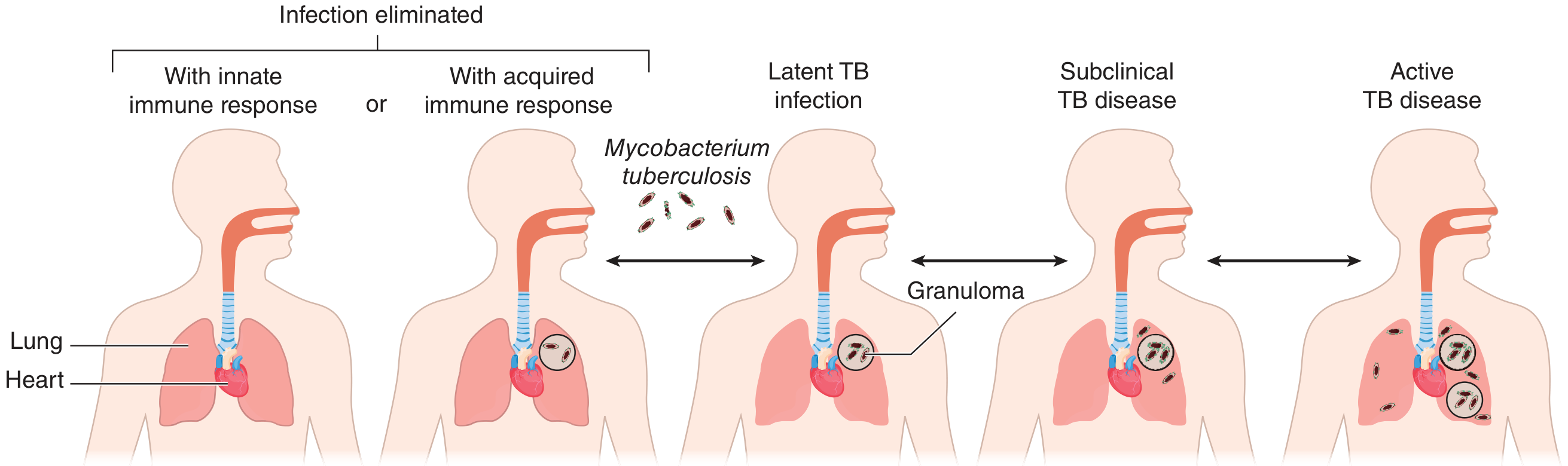
Spectrum of outcomes after M. tuberculosis infection: infection may be eliminated, remain latent (contained in granulomas), progress to subclinical disease, or advance to active TB disease.
Pathogenesis
After inhalation, bacilli reach the alveoli and are engulfed by macrophages. A cell-mediated immune response develops over 2-8 weeks, forming granulomas (tubercles) that contain the infection. The outcome depends on host immunity:
- Infection eliminated - innate or acquired immune response clears the bacteria
- Latent TB infection (LTBI) - bacteria persist dormant in granulomas; TST/IGRA positive, culture negative, no symptoms
- Progressive primary infection - active disease within the first year of initial infection
- Reactivation (post-primary) TB - reactivation of LTBI, typically years later, often due to immunosuppression
About 5-10% of immunocompetent infected persons will progress to active disease during their lifetime, with the highest risk in the first 2 years.
Clinical Features
Symptoms
| Symptom | Notes |
|---|---|
| Persistent cough | Most common symptom; productive or dry; can be absent in up to 25% of culture-confirmed cases |
| Fever | Often low-grade, evening rise |
| Night sweats | Classic constitutional symptom |
| Weight loss / anorexia | Gradual, "consumption" |
| Hemoptysis | Seen in more advanced/cavitary disease; may be from Rasmussen aneurysm or aspergilloma in old cavity |
| Chest pain | Pleuritic, if pleura is involved |
| Dyspnea | Extensive disease or pleural effusion |
Physical Examination
- Often unremarkable in early disease
- Post-tussive rales in upper lung zones
- Amphoric breath sounds suggest cavity
- Lymphadenopathy is uncommon in immunocompetent adults (more prominent in HIV)
Radiological Features
Chest X-Ray:
- Primary TB: Lower or middle lobe infiltrate + hilar/mediastinal lymphadenopathy (Ghon complex); pleural effusion
- Reactivation TB: Upper lobe infiltrates (posterior segments), fibronodular opacities, cavitation (hallmark of advanced disease), volume loss
- Miliary TB: Diffuse 1-2 mm nodules throughout both lungs (hematogenous spread)
CT Chest: More sensitive - shows tree-in-bud opacities (endobronchial spread), cavities, consolidation, pleural involvement, lymphadenopathy.
Diagnosis
Step 1: Clinical suspicion
Persistent cough (any duration) + systemic symptoms (fever, night sweats, weight loss) + epidemiological risk factors (high-incidence country origin, HIV, immunosuppression, close contact, incarceration, homelessness).
Step 2: Sputum Specimens
- At least 2-3 sputum specimens for:
- AFB smear microscopy (Ziehl-Neelsen or fluorochrome stain) - rapid but ~40-60% sensitive
- Mycobacterial culture (gold standard; Lowenstein-Jensen medium or liquid MGIT system) - 3-8 weeks for solid, 1-3 weeks for liquid; needed for drug susceptibility testing
- NAAT/PCR - at least 1 specimen; recommended as initial test in low-incidence settings
Step 3: Nucleic Acid Amplification Testing (NAAT)
| Situation | Interpretation |
|---|---|
| AFB smear+ and NAAT+ | Confirms TB rapidly |
| AFB smear+ and NAAT- | Suggests NTM (NAATs distinguish MTb from NTM) |
| AFB smear- and NAAT+ | Presumptive TB in intermediate/high risk |
| AFB smear- and NAAT- | Does NOT exclude active TB; culture still required |
Xpert MTB/RIF (GeneXpert): Detects M. tuberculosis AND rifampicin resistance in 90 minutes; recommended by WHO as the preferred initial test in HIV+ patients, MDR-TB risk, and seriously ill patients.
Step 4: Drug Susceptibility Testing (DST)
- Required for all culture-positive cases
- Phenotypic DST for first-line drugs (HRZE)
- Targeted next-generation sequencing (tNGS) increasingly used for rapid genotypic DST - a 2024 meta-analysis in Lancet Infect Dis (PMID: 38795712) shows high diagnostic accuracy
Step 5: Tests for Latent TB Infection (LTBI)
- Tuberculin Skin Test (TST/Mantoux): Intradermal 5 TU PPD, read at 48-72h
- Cut-off ≥5 mm: HIV+, immunosuppressed, close contacts, chest X-ray with old fibrotic lesions
- Cut-off ≥10 mm: Recent immigrants, IV drug users, high-risk groups, children <4 years
- Cut-off ≥15 mm: No risk factors
- IGRA (Interferon-Gamma Release Assay): QuantiFERON-TB Gold, T-SPOT.TB
- Preferred in BCG-vaccinated persons (not affected by BCG)
- More specific than TST
Treatment
Drug-Susceptible TB (Standard Regimen)
Total duration: 6 months (2HRZE/4HR)
| Phase | Drugs | Duration |
|---|---|---|
| Intensive phase | Isoniazid (H) + Rifampicin (R) + Pyrazinamide (Z) + Ethambutol (E) | 2 months |
| Continuation phase | Isoniazid (H) + Rifampicin (R) | 4 months |
Key points:
- Ethambutol can be omitted if the organism is known to be fully susceptible
- Pyridoxine (vitamin B6) supplemented with isoniazid to prevent peripheral neuropathy (especially in malnourished, diabetic, HIV+, pregnant)
- Monitor liver function (hepatotoxicity from H, R, Z)
- Monitor visual acuity and colour vision (ethambutol optic neuritis)
Important Drug Side Effects
| Drug | Key Adverse Effects |
|---|---|
| Isoniazid | Hepatotoxicity, peripheral neuropathy, drug-induced lupus, seizures (pyridoxine deficiency) |
| Rifampicin | Hepatotoxicity, orange discolouration of fluids, enzyme inducer (reduces OCP, warfarin efficacy), flu-like syndrome |
| Pyrazinamide | Hepatotoxicity, hyperuricaemia/gout, arthralgia |
| Ethambutol | Optic neuritis (dose-dependent, reversible if caught early) |
Drug-Resistant TB
- MDR-TB: Resistant to at least isoniazid + rifampicin; requires 18-24 months of second-line drugs (fluoroquinolones, bedaquiline, linezolid, etc.)
- XDR-TB: MDR-TB + resistance to fluoroquinolones + at least one of bedaquiline/linezolid
- Consultation with a TB specialist is mandatory for drug-resistant cases
Special Situations
HIV-TB Co-infection
- Most important risk factor for progression from LTBI to active TB
- Antiretroviral therapy (ART) started within 2 weeks of TB treatment initiation (unless TB meningitis)
- Risk of TB-IRIS (immune reconstitution inflammatory syndrome): occurs in 5-50% of HIV patients starting ART; manifests as paradoxical worsening - fever, lymphadenitis, new infiltrates
- Rifampicin interactions with antiretrovirals require regimen adjustments
Pregnancy
- TB treatment is safe in pregnancy
- Streptomycin is contraindicated (ototoxicity to fetus)
- Standard HRZE regimen used; pyridoxine supplemented
Diabetes
- DM is a major risk factor for TB and for treatment failure; a 2024 systematic review (PMID: 38346381) documents significantly worse treatment outcomes in TB-DM comorbidity
- Rifampicin reduces sulfonylurea and metformin levels; glycaemic monitoring required
Monitoring Treatment Response
- Sputum smear and culture at 2 months (end of intensive phase) - culture conversion is the key marker of response
- If culture positive at 2 months: extends treatment consideration; rule out resistance
- Chest X-ray improvement expected but lags behind bacteriological response
- Monthly clinical review for adherence and side effects
Infection Control & Public Health
- Airborne precautions (negative pressure room, N95 respirators) until patient is non-infectious (typically 3 negative AFB smears on 3 separate days + clinical improvement + 2 weeks of effective therapy)
- Contact tracing for close contacts of smear-positive cases
- Directly Observed Therapy (DOT): The standard of care to ensure adherence and prevent resistance
- Notification: TB is a notifiable disease in most countries
Prognosis
With appropriate treatment, drug-susceptible pulmonary TB is curable in >95% of cases. Untreated, TB has a mortality of approximately 50%. Poor prognostic factors include MDR/XDR-TB, HIV co-infection, malnutrition, poor adherence, and delayed diagnosis.
Sources: Goldman-Cecil Medicine, 27th Ed., p. 3252-3256; Murray & Nadel's Textbook of Respiratory Medicine; Park's Textbook of Preventive and Social Medicine; Red Book 2021 (Committee on Infectious Diseases)
Recurrent vomiting since 1 year in 15 years old boy . What may be possible cause
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
I now have comprehensive material covering the differential diagnosis of recurrent/chronic vomiting from multiple authoritative gastroenterology textbooks. I have enough to compile a thorough, well-organized answer.
Recurrent Vomiting for 1 Year in a 15-Year-Old Boy - Possible Causes
Recurrent vomiting lasting 1 year in an adolescent is a chronic symptom requiring a systematic differential. The duration rules out acute infectious causes; the focus shifts to functional, structural, metabolic, neurological, and psychosocial etiologies. A 15-year-old male has specific considerations - notably cyclic vomiting syndrome (CVS), GERD/peptic disease, eating disorders, and cannabis use.
1. Functional / Motility Disorders (Most Common Category)
Cyclic Vomiting Syndrome (CVS)
Top diagnosis to consider in this age group.
- Stereotyped, recurrent discrete episodes of intense vomiting (up to 20-30 episodes/day), each lasting hours to days, with complete symptom-free intervals between attacks
- Rome IV criteria: ≥3 episodes in the prior year, ≥2 episodes in the past 6 months, each at least 1 week apart, each lasting <1 week
- Associated with abdominal pain, nausea, pallor, diaphoresis, photophobia
- Personal or family history of migraine is strongly supportive
- Four phases: preemetic (pallor, nausea) → intense vomiting → recovery → symptom-free interval
- Common triggers: emotional stress, sleep deprivation, infection, certain foods (chocolate, cheese, MSG, milk/soy/eggs), menses
- Can evolve into chronic daily nausea/vomiting or migraine headaches over time
Functional Dyspepsia (FD)
- Epigastric pain/discomfort, early satiety, nausea, and vomiting with normal upper endoscopy
- Postprandial distress syndrome subtype most common
- Gastric dysmotility and impaired accommodation are underlying mechanisms
Gastroparesis
- Delayed gastric emptying causing early satiety, nausea, postprandial vomiting, bloating
- In adolescents usually idiopathic; secondary causes include diabetes, post-viral (e.g., post-infectious autonomic neuropathy)
Chronic Nausea and Vomiting Syndrome (CNVS) - Rome IV
- At least 1 vomiting episode/week for ≥3 months; no organic cause found on routine investigations including upper endoscopy
2. Structural / Obstructive Causes
| Condition | Key Clues |
|---|---|
| Peptic ulcer disease (PUD) | Epigastric pain, relieved by food/antacids, H. pylori common in adolescents |
| GERD / Esophagitis | Heartburn, regurgitation, worse when lying down or after meals |
| Superior mesenteric artery (SMA) syndrome | Tall, thin/rapidly growing adolescent; bilious vomiting, postprandial pain; duodenal compression by SMA |
| Gastric outlet obstruction | Non-bilious projectile vomiting, epigastric fullness; may be from peptic ulcer/scarring |
| Malrotation / intermittent volvulus | Bilious vomiting; can present in adolescence; intermittent abdominal pain |
| Intestinal stricture / Crohn disease | Chronic abdominal pain, diarrhea, weight loss, rectal bleeding |
3. Neurological Causes
| Condition | Key Clues |
|---|---|
| Raised intracranial pressure (ICP) | Morning vomiting without nausea (classically projectile), headache worse on waking/Valsalva, papilloedema - must exclude in a child with chronic vomiting |
| Brain tumor | Posterior fossa tumors (medulloblastoma, ependymoma) classically cause vomiting via ICP or direct stimulation of the vomiting center |
| Chiari malformation | Hindbrain herniation; can cause chronic vomiting, headache, dysphagia |
| Abdominal migraine | Recurrent episodes of midline periumbilical pain + vomiting; often a CVS precursor; strong family history of migraine |
| Hydrocephalus | Headache, visual changes, cognitive changes |
| Seizure disorder | Ictal or postictal vomiting (rare as sole manifestation) |
Red flag: Projectile morning vomiting WITHOUT nausea in a child/adolescent = raised ICP until proven otherwise. Brain imaging mandatory.
4. Metabolic and Endocrine Causes
| Condition | Key Clues |
|---|---|
| Diabetic gastroparesis / poorly controlled DM | Polydipsia, polyuria, weight loss; postprandial vomiting |
| Addison's disease (adrenal insufficiency) | Fatigue, hyperpigmentation, postural hypotension, hyponatraemia, hyperkalaemia, hypoglycaemia |
| Hypothyroidism | Fatigue, constipation, weight gain, cold intolerance, bradycardia |
| Hyperthyroidism | Weight loss, palpitations, heat intolerance, anxiety |
| Uraemia (chronic kidney disease) | Oedema, hypertension, anaemia, haematuria, proteinuria |
| Hypercalcaemia | Bones, stones, groans, psychic moans; nausea and vomiting; usually due to hyperparathyroidism |
| Inborn errors of metabolism | Recurrent vomiting since childhood, triggered by fasting/illness; suspect mitochondrial, urea cycle, or organic acidaemia disorders |
5. Gastrointestinal Inflammatory Causes
| Condition | Key Clues |
|---|---|
| Crohn disease | Abdominal pain, diarrhea, weight loss, perianal disease, elevated ESR/CRP, anaemia |
| Eosinophilic gastroenteritis | Food allergy history, peripheral eosinophilia, responds to dietary exclusion |
| Celiac disease | Diarrhea, weight loss, iron deficiency anaemia, positive anti-tTG IgA |
| Helicobacter pylori gastritis | Epigastric pain, nausea, early satiety |
6. Psychosocial and Eating Disorder Causes
Especially relevant in an adolescent:
| Condition | Key Clues |
|---|---|
| Bulimia nervosa | Self-induced vomiting after eating; normal or above-normal weight; dental erosions, parotid hypertrophy, Russell's sign (knuckle calluses); secretive behaviour |
| Anorexia nervosa | Severe weight loss, distorted body image, restrictive eating; vomiting may be self-induced or a consequence of restriction |
| Psychogenic/functional vomiting | Linked to school avoidance, anxiety, stress (exam periods, family conflict); absence of structural cause |
| Anxiety disorders / Depression | Somatic symptoms including chronic nausea and vomiting |
| Rumination syndrome | Effortless regurgitation of recently eaten food within minutes of eating; rechewed and reswallowed; no nausea; often misdiagnosed as vomiting |
7. Toxic / Substance-Related Causes
| Cause | Notes |
|---|---|
| Cannabinoid hyperemesis syndrome (CHS) | Chronic cannabis use; clinically indistinguishable from CVS; characteristic relief with hot bathing/showering; resolves completely with cannabis cessation |
| Alcohol / substance use | Common in adolescents; direct gastric irritation |
| Medications | NSAIDs (gastritis), opioids, antibiotics, anticonvulsants, chemotherapy agents |
| Chronic lead/heavy metal exposure | Rare; abdominal cramps, constipation, pallor, cognitive changes |
8. Miscellaneous Causes
- Pregnancy - must always be considered in adolescent females (even if boy in this case, relevant for differential completeness)
- Recurrent pancreatitis - episodic epigastric/back pain with vomiting; elevated amylase/lipase; gallstones, anatomic anomalies (pancreas divisum)
- Cholelithiasis / biliary dyskinesia - right upper quadrant pain after fatty meals
- Recurrent urinary tract infection / hydronephrosis - flank pain, UTI symptoms
Approach to This Patient
History - Key Questions
- Pattern: Episodic (with symptom-free periods) vs. continuous daily vomiting?
- Timing: Morning vomiting (raised ICP, pregnancy), postprandial (GERD, gastroparesis, FD), unrelated to meals (CVS, metabolic)
- Vomit character: Bilious (below pylorus, obstruction), blood/coffee grounds (peptic disease/bleeding), undigested food hours after eating (gastroparesis)
- Associated symptoms: Headache, visual changes (ICP/migraine), weight loss, diarrhea, abdominal pain, fever
- Triggers: Stress, food, menstruation, cannabis use
- Family history: Migraine
- Psychiatric history: Body image concerns, eating habits, anxiety
Red Flag Symptoms (Urgent Evaluation Required)
- Projectile vomiting without nausea - raised ICP / brain tumour
- Bilious vomiting - intestinal obstruction / malrotation
- Haematemesis - upper GI bleed
- Significant weight loss
- Neurological symptoms (headache, visual changes, diplopia)
- Papilloedema on fundoscopy
- Nocturnal vomiting (wakes patient from sleep)
Investigations
| Test | Purpose |
|---|---|
| Blood: FBC, ESR, CRP, LFTs, renal function, electrolytes | Screen for inflammatory, metabolic causes |
| Blood glucose, HbA1c | Diabetes |
| TFTs (TSH, T3, T4) | Thyroid disease |
| Serum calcium, PTH | Hypercalcaemia |
| Urine: urinalysis, urine pregnancy test | Renal disease; pregnancy (females) |
| H. pylori (stool antigen or UBT) | H. pylori gastritis |
| Anti-tTG IgA | Coeliac disease |
| Upper GI endoscopy | Peptic disease, oesophagitis, gastroparesis (if biopsy eosinophils) |
| Gastric emptying scintigraphy | Gastroparesis |
| Upper GI barium / CT abdomen | Structural anomaly, SMA syndrome, malrotation |
| MRI/CT brain | Raised ICP, brain tumour, Chiari malformation |
| Urine organic acids, plasma amino acids | Metabolic disorders (if other causes excluded) |
Summary - Most Likely Diagnoses in a 15-Year-Old Boy
| Priority | Diagnosis | Reason |
|---|---|---|
| 1st | Cyclic Vomiting Syndrome | Most common cause of episodic recurrent vomiting in adolescents; migraine link |
| 2nd | Functional dyspepsia / GERD / H. pylori | Very common in adolescents |
| 3rd | Cannabinoid hyperemesis syndrome | Common and under-recognised in adolescents; ask directly |
| 4th | Brain tumour / raised ICP | Must not be missed - morning vomiting, headache are red flags |
| 5th | Psychogenic / anxiety-related | School stress, family issues, exam pressure common in this age group |
| 6th | Metabolic (DM, adrenal, thyroid) | Treatable if detected early |
| 7th | Eating disorder / rumination | Less likely in males but not impossible |
Sources: Sleisenger and Fordtran's Gastrointestinal and Liver Disease (Box 50.1); Yamada's Textbook of Gastroenterology, 7th Ed.; Rosen's Emergency Medicine; Goldman-Cecil Medicine, 27th Ed.
This is a shared conversation. Sign in to Orris to start your own chat.