Squat asssement in detail and each muscle work with their rationale and if the patient is able to do squat but not able to balnce and does squat on forefoot which muscle is not working properly and which is over working and how to correct it
squat assessment forefoot weight bearing muscle imbalance physiotherapy correction
squat on toes forefoot overactive underactive muscles gastrocnemius soleus hip flexor weakness correction exercises
https://blog.nasm.org/certified-personal-trainer/how-to-perf…
Squat Assessment - Complete Clinical Guide
PART 1: THE SQUAT ASSESSMENT FRAMEWORK
How to Set Up the Assessment
- Feet shoulder-width apart, toes pointing forward (or slightly out at 5-7 degrees)
- Arms raised overhead or in front
- Perform 3-5 repetitions of a bodyweight squat
- Observe from three views: anterior (front), lateral (side), posterior (back)
What You Are Observing at Each Joint
| View | Joint/Region | What to Check |
|---|---|---|
| Lateral | Ankle | Heel rise, dorsiflexion availability |
| Lateral | Knee | Excessive forward travel, flexion depth |
| Lateral | Hip/LPHC | Forward lean of torso, lumbar arch |
| Anterior | Feet | Turn-out, pronation/supination |
| Anterior | Knee | Valgus (caving in) or varus (bowing out) |
| Anterior | Hip | Level, not shifting |
| Posterior | Heels | Lifting off ground |
| Lateral | Upper body | Arms falling forward |
PART 2: MUSCLE-BY-MUSCLE ROLE IN THE SQUAT
A. ANKLE COMPLEX
1. Gastrocnemius & Soleus (Calf Complex)
- Action during squat: Eccentrically control forward tibial translation (dorsiflexion) as you descend; concentrically plantarflex as you rise
- Rationale: They must LENGTHEN during the descent phase to allow the tibia to move forward over the foot. If they are tight/overactive, they resist this tibial advance, causing the heel to rise or the torso to lean forward
- Normal requirement: ~15-20 degrees of dorsiflexion at the ankle is needed for a proper squat
2. Anterior Tibialis
- Action: Dorsiflexor - pulls the foot/shin forward during descent; controls rate of plantarflexion during rise
- Rationale: Acts as an antagonist to the calf. An underactive anterior tibialis means loss of dorsiflexion control and poor eccentric loading of the ankle. This is commonly underdeveloped
3. Peroneals (Fibularis Longus/Brevis)
- Action: Evert the foot, stabilize the lateral ankle
- Rationale: Prevent the arch from collapsing inward (pronation) during load. Underactivity leads to foot flattening and ankle instability during squat
B. KNEE COMPLEX
4. Quadriceps (Rectus Femoris, Vastus Medialis/Lateralis/Intermedius)
- Action: Primary knee extensors - control the eccentric descent and power the concentric rise
- Rationale: Vastus Medialis Oblique (VMO) specifically stabilizes the patella medially. Without adequate VMO activation, the patella tracks laterally, causing knee pain and valgus tendency
- Key note: Rectus femoris crosses both hip and knee; it also flexes the hip, making it prone to shortening in sedentary individuals
5. Hamstrings (Biceps Femoris, Semitendinosus, Semimembranosus)
- Action: Eccentrically control knee extension; assist hip extension; stabilize the knee against anterior tibial shear
- Rationale: The hamstrings act as synergists to the ACL - they protect the knee during loaded squatting. They also co-contract with quads for joint compression and stability at the bottom of the squat
C. HIP COMPLEX
6. Gluteus Maximus
- Action: Primary hip extensor - drives the body upward from the bottom position; eccentrically controls hip flexion on descent
- Rationale: The most powerful muscle in the squat. Inhibited gluteus maximus is the most common finding in dysfunctional squats. When it does not fire, the hip flexors dominate, creating anterior pelvic tilt and compensatory forward lean
7. Gluteus Medius & Minimus
- Action: Hip abductors and internal rotators - stabilize the pelvis in the frontal plane, prevent hip adduction and knee valgus
- Rationale: Without adequate gluteus medius activity, the hip drops or adducts during single-leg loading. In bilateral squat, weakness shows as knee cave (valgus) or hip shift
8. Hip Flexors (Iliopsoas, Rectus Femoris, TFL)
- Action: Eccentrically decelerate hip extension during rise; concentrically flex hip during descent phase
- Rationale: Overactive/tight hip flexors tilt the pelvis anteriorly. This increases lumbar lordosis, inhibits the gluteus maximus (reciprocal inhibition), and causes excessive forward lean. One of the most common sources of squat dysfunction
9. Deep Hip External Rotators (Piriformis, Obturator group, Gemelli)
- Action: Maintain femoral head centralization in the acetabulum; provide rotational stability
- Rationale: They keep the femur in proper alignment throughout the range of motion. Tightness causes excessive foot turn-out; weakness causes internal rotation and knee valgus
10. Adductors (Magnus, Longus, Brevis, Gracilis)
- Action: Control hip abduction; Adductor Magnus is also a powerful hip extensor (posterior fibers)
- Rationale: Tight adductors (especially short head Biceps Femoris and TFL) contribute to knee valgus. Adductor Magnus assists gluteus maximus in the final push of hip extension
D. LUMBOPELVIC-HIP COMPLEX (CORE)
11. Transverse Abdominis (TVA), Multifidus, Internal Oblique
- Action: Create intra-abdominal pressure (IAP); stabilize the lumbar spine and pelvis
- Rationale: These intrinsic core stabilizers MUST fire first (milliseconds before limb movement). Without them, the lumbar spine is unsupported, leading to excessive arch or flexion during the squat
12. Erector Spinae
- Action: Extend the lumbar spine; maintain upright torso position
- Rationale: Work eccentrically to control forward lean. If overactive (without core co-activation), they create hyperextension of the lumbar spine (excessive arch/butt wink)
PART 3: THE SPECIFIC PROBLEM - SQUAT ON FOREFOOT (Heel Rise / Toe Squat)
What Is Actually Happening Biomechanically?
- Lifting the heels (rising onto forefoot) - reduces the dorsiflexion demand
- Shifting weight forward onto the ball of the foot - shifts center of mass anteriorly
- Producing excessive forward trunk lean - to keep center of mass over base of support
- Loss of balance - because the base of support (full foot) is no longer used
OVERACTIVE / TIGHT MUSCLES (the problem creators)
| Muscle | Why It Is Overactive | Effect |
|---|---|---|
| Gastrocnemius | Primary plantarflexor, crosses both ankle AND knee - tightens with prolonged sitting/heel wearing | Limits dorsiflexion - heel rises |
| Soleus | Deep plantarflexor, crosses only ankle - tightens with prolonged activity/footwear | Limits dorsiflexion even with knee bent |
| Hip Flexor Complex (Iliopsoas, Rectus Femoris, TFL) | Tight from sitting, sedentary lifestyle | Pulls pelvis anteriorly, causes forward trunk lean and weight shift to forefoot |
| Abdominal Complex (in some cases) | Short/overactive abs pull thorax forward | Contributes to excessive forward lean |
UNDERACTIVE / WEAK MUSCLES (the muscles not doing their job)
| Muscle | Why It Is Underactive | Effect |
|---|---|---|
| Anterior Tibialis | Neurologically inhibited by overactive calf (reciprocal inhibition); often simply undertrained | Cannot pull the tibia forward; dorsiflexion is blocked |
| Gluteus Maximus | Inhibited by overactive hip flexors (reciprocal inhibition); neurologically "switched off" | Cannot extend hip properly; person collapses forward |
| Erector Spinae | Underactive relative to hip flexors | Cannot maintain upright torso; trunk leans forward |
| Intrinsic Core Stabilizers (TVA, Multifidus) | Poor core activation patterns | Pelvis becomes unstable; balance is lost |
| Tibialis Posterior | Weak ankle stabilizer | Contributes to poor medial arch stability and ankle wobble during squat |
The Vicious Cycle Explained
Tight Gastrocnemius/Soleus
↓
Limited Ankle Dorsiflexion
↓
Heels Rise → Weight Shifts to Forefoot
↓
Centre of Mass Shifts Forward
↓
Body Compensates with Forward Trunk Lean
↓
Hip Flexors Dominate → Gluteus Maximus is Inhibited
↓
Loss of Posterior Chain Power → Instability + Poor Balance
PART 4: CORRECTION PROTOCOL
STEP 1 - Release / Inhibit Overactive Muscles (First 5-10 minutes)
- Foam Rolling / Myofascial Release: Roll the entire calf (medial/lateral heads), pausing on tender spots for 30-90 seconds
- Standing Gastrocnemius Stretch: Straight knee, foot flat on wall, lean forward - hold 30-60 seconds x 3
- Soleus Stretch (bent-knee calf stretch): Slight knee bend, lean into wall - this specifically targets the soleus which the straight-leg stretch misses. Hold 30-60 seconds x 3
- Half-kneeling hip flexor stretch (90/90 stretch): Kneeling on one knee, lunge forward, posteriorly tilt pelvis, feel stretch in front of rear hip - hold 30-60 seconds
- Foam roll rectus femoris / TFL
STEP 2 - Activate / Strengthen Underactive Muscles
- Seated toe raises / ankle dorsiflexion with resistance band: Pull foot upward against resistance - 3 x 15
- Heel walking: Walk on heels for 20-30 meters - direct tibialis anterior training
- Dorsiflexion with band while squatting: Attach band at ankle to provide resistance to dorsiflexion during squat
- Supine Glute Bridges: 3 x 15, hold 2 seconds at top - classic gluteus maximus isolation
- Hip Thrusts (progressed): More hip extension range, stronger glute activation
- Prone Hip Extension: Lying face down, lift one leg - isolates gluteus maximus
- Clamshells (also activates glute medius)
- Dead Bug: Supine, arms/legs in air, alternate lowering opposite arm/leg while maintaining neutral spine - activates TVA/multifidus
- Bird Dog: Quadruped, extend opposite arm and leg - builds core stability
- Pallof Press: Anti-rotation core stability
STEP 3 - Re-train the Squat Pattern (Corrective Exercises)
- Place a 1-2 inch heel elevation (wedge, plates) under heels
- This reduces the dorsiflexion demand and allows the patient to learn proper squat depth and pattern without the ankle restriction
- Gradually reduce elevation over weeks
- Squat to a box, emphasizing sitting back rather than down
- Cues: "Push your knees out," "Keep your chest up," "Feel weight through your heels"
- Back against wall, slide down slowly
- Squeezing the ball between knees activates VMO and adductors
- Forces posterior weight distribution
- Stand facing wall, foot 10 cm from wall, drive knee toward wall over 5th toe
- Measure how far the foot can be from wall while knee touches it
- Normal: ~10-12 cm; less = restricted dorsiflexion
- Perform as a daily mobility drill: 3 x 10 reps each side
- Static single-leg stance: 30 seconds eyes open → eyes closed → unstable surface
- Single-leg squat to box: Small depth, controlled
- Builds proprioceptive feedback from the ankle and hip
STEP 4 - Full Integration (Return to Functional Squat)
- Goblet Squat: Holding a weight in front keeps the torso upright and teaches proper depth. One of the best teaching tools for the squat
- Bulgarian Split Squat: Challenges single-leg strength and ankle mobility
- Tempo Squats (3-1-1): Slow eccentric (3 seconds down), pause, drive up - builds eccentric control and teaches patience at the bottom
QUICK REFERENCE SUMMARY TABLE
| Finding | Overactive (Tight) | Underactive (Weak) | Correction Focus |
|---|---|---|---|
| Heels rise / squat on forefoot | Gastrocnemius, Soleus | Anterior Tibialis, Tibialis Posterior | Calf stretching + ankle mobility + dorsiflexor strengthening |
| Excessive forward trunk lean | Gastrocnemius, Soleus, Hip Flexors, Abdominals | Gluteus Maximus, Anterior Tibialis, Erector Spinae | Hip flexor release + glute activation |
| Loss of balance | Gastrocnemius/Soleus (limits ankle proprioception base) | Intrinsic core stabilizers, Gluteus Maximus, Tibialis Anterior | Proprioception training + single-leg balance + full chain stability |
| Knee valgus (if present) | Adductors, Biceps Femoris (short head), TFL, Vastus Lateralis | Gluteus Medius/Maximus, VMO | Glute med activation + VMO strengthening |
| Low back arch | Hip Flexors, Erector Spinae, Latissimus Dorsi | Gluteus Maximus, Hamstrings, Intrinsic Core | Posterior chain strengthening + hip flexor release |
CLINICAL PRIORITIES FOR YOUR PATIENT
- Day 1-2: Assess ankle dorsiflexion with the knee-to-wall test to confirm restriction. Check if heels-elevated squat fixes the balance problem (if yes, it is predominantly ankle/calf restriction)
- Week 1-2: Aggressive calf release (foam rolling, manual therapy) + static stretching twice daily + ankle dorsiflexion exercises
- Week 1-2: Activate anterior tibialis (heel walks, banded dorsiflexion)
- Week 2-3: Add glute activation (bridges, hip thrusts) and core stabilization
- Week 3-4: Progress to heels-elevated squats, then gradually bring heels to level ground
- Ongoing: Proprioception and balance training (single-leg, unstable surfaces) to address the balance deficit specifically
Create an infographic showing the normal vs. forefoot squat muscle firing patterns
Medical physiotherapy infographic titled "Squat Assessment: Normal vs Forefoot Squat - Muscle Firing Patterns". Split into two main columns side by side. LEFT COLUMN - "NORMAL SQUAT" with green color theme: - Stick figure/anatomical figure in proper deep squat position: feet flat on ground, knees tracking over toes, upright torso, hips below knees - Muscle activation indicators (green glowing highlights) on: Gluteus Maximus (ACTIVE - large label), Gluteus Medius (ACTIVE), Quadriceps/VMO (ACTIVE), Hamstrings (ACTIVE), Anterior Tibialis (ACTIVE), Core/TVA (ACTIVE), Gastrocnemius/Soleus (NORMAL LENGTHENING) - Ankle shows full dorsiflexion arrow - Center of mass line passes through mid-foot - Label: "Weight distributed through FULL FOOT" - Small green checkmarks next to each active muscle RIGHT COLUMN - "FOREFOOT SQUAT (Dysfunction)" with red/orange color theme: - Same figure but with heels raised off ground, excessive forward trunk lean, weight on toes/ball of foot - OVERACTIVE muscles shown in bright red/orange with flame or warning icons: Gastrocnemius (OVERACTIVE - TIGHT), Soleus (OVERACTIVE - TIGHT), Hip Flexors/Iliopsoas (OVERACTIVE), with arrows showing they are pulling/restricting - UNDERACTIVE muscles shown in faded grey/blue with sleeping or weak icons: Anterior Tibialis (UNDERACTIVE), Gluteus Maximus (INHIBITED), Core Stabilizers (UNDERACTIVE) - Ankle shows restricted dorsiflexion with a red X or block symbol - Center of mass line shifted forward over toes - Label: "Weight shifted to FOREFOOT / TOES" - Red warning symbols BOTTOM SECTION - "Correction Protocol" banner in purple/blue: Three boxes: 1) "RELEASE" - foam roll calf, stretch gastroc/soleus, hip flexor stretch | 2) "ACTIVATE" - tibialis anterior, gluteus maximus, core stabilizers | 3) "RETRAIN" - heels-elevated squat, ankle mobility drill, single-leg balance Clean medical infographic style, white background, professional clinical design, anatomical accuracy, bold clear labels, arrows indicating muscle pull directions, color-coded legend at bottom (Green = Normal/Active, Red = Overactive, Grey = Underactive)
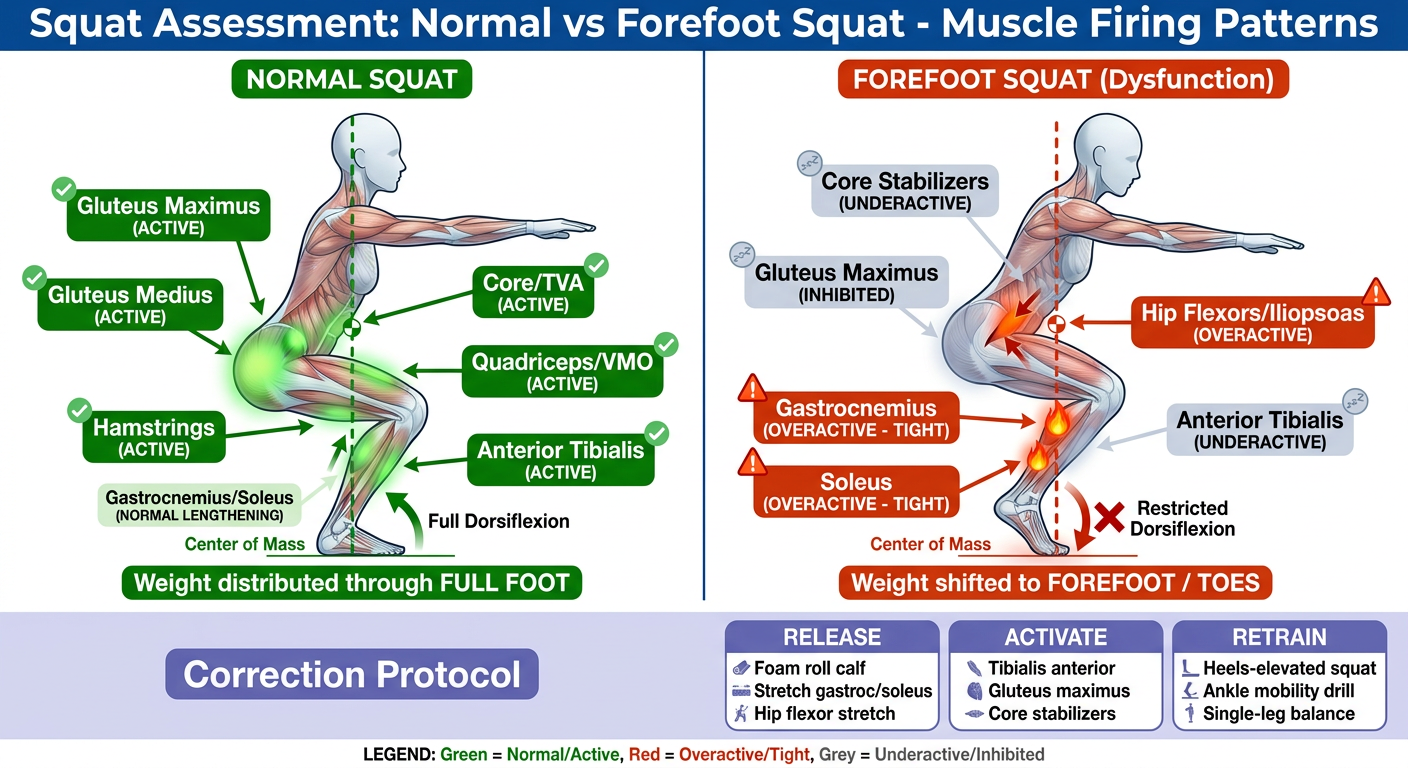
- Full foot contact, center of mass over mid-foot
- Gluteus Maximus, VMO, Anterior Tibialis, and Core all firing normally
- Gastrocnemius/Soleus elongating eccentrically to allow dorsiflexion
- Heels raised, forward trunk lean, weight on toes
- Gastrocnemius + Soleus = Overactive (tight, blocking dorsiflexion)
- Hip Flexors = Overactive (pulling pelvis forward)
- Anterior Tibialis + Gluteus Maximus + Core = Underactive/Inhibited
- Release - Foam roll calf, stretch gastroc/soleus and hip flexors
- Activate - Heel walks, glute bridges, dead bug for core
- Retrain - Heels-elevated squat progressing to flat ground, ankle mobility drills, single-leg balance
How to improve with manual theraphy in single session
manual therapy single session squat improvement ankle dorsiflexion joint mobilization techniques physiotherapy
manual therapy ankle dorsiflexion squat improvement
manual therapy session protocol calf soft tissue release hip flexor MET muscle energy technique squat dysfunction physiotherapy
manual therapy mobilization squat movement improvement
https://pmc.ncbi.nlm.nih.gov/articles/PMC12585996
Manual Therapy: Single Session Protocol for Forefoot Squat Correction
Baseline First (2 minutes)
- Knee-to-wall test (WBLT): foot distance from wall when knee just touches - record in cm
- Perform squat - observe heel rise, trunk lean, balance
- Re-assess after each intervention block to demonstrate change in the same session
BLOCK 1 - Soft Tissue Release: Calf Complex (10-12 min)
A. Deep Transverse Friction / Myofascial Release - Gastrocnemius
- With thumbs or heel of palm, apply sustained deep pressure along the medial and lateral heads of gastrocnemius from the knee to the musculotendinous junction
- Use cross-fiber friction strokes perpendicular to muscle fibers
- Work for 2-3 minutes per side
- Locate and hold trigger points (tender nodules) for 60-90 seconds each until tissue releases or pain drops from 7/10 to 3/10
B. Deep Transverse Friction - Soleus
- Press thumbs deep medially and laterally beneath the gastrocnemius bulk
- Firm longitudinal stripping strokes from proximal to distal soleus
- 2 minutes each side
- Soleus responds well to sustained ischemic compression on trigger points
C. MET for Gastrocnemius - Post-Isometric Relaxation
- Bring foot to end-range dorsiflexion (knee straight) until resistance is felt
- Ask patient: "Gently push your foot downward against my hand" (isometric plantarflexion) at 20-30% effort
- Hold 7-10 seconds
- Patient relaxes completely
- Therapist takes up new slack - moves to next dorsiflexion barrier
- Repeat 3-5 times
- Final stretch hold: 30 seconds
D. MET for Soleus
BLOCK 2 - Joint Mobilization: Ankle (8-10 min)
A. Anterior-to-Posterior (A-P) Talar Mobilization - Maitland Grade III/IV
- Stabilize the distal tibia/fibula with one hand (wrap around behind)
- Place both thumbs on the anterior dome of the talus (just below the ankle joint line)
- Apply a posterior glide to the talus (pressing it back into the mortise)
- Perform rhythmic oscillations using 1-second glides to end-range
- Grade III: reaching end-range on each oscillation
- Grade IV: small amplitude, at end-range with gentle overpressure
- Volume: 3-4 sets of 30-60 seconds (60-120 total gliding movements)
- Reassess WBLT after each set
B. Mobilization With Movement (MWM) - Mulligan Technique
- Therapist stands beside patient
- Apply a posterior/posterior-lateral glide to the talus with thumbs (same direction as above) while maintaining the glide firmly
- Patient actively bends knee forward over foot (performs a mini-squat or lunge) moving into dorsiflexion
- The movement should be pain-free - if painful, adjust glide angle
- At end-range, hold 2-3 seconds, return to start (maintain glide throughout)
- Volume: 4 sets x 10-15 repetitions
- Reassess WBLT between sets
C. Subtalar Joint Mobilization (if eversion is restricted)
- Stabilize talus with one hand
- Apply lateral (eversion) glide to the calcaneus with the other hand
- 2-3 sets x 30 seconds rhythmic Grade III oscillations
BLOCK 3 - Hip Flexor Release (5-7 min)
A. Soft Tissue Release - Iliopsoas
- Palpate 2 cm medial to ASIS, slowly sink fingers deep into the iliac fossa medially
- Wait for the muscle to soften under your fingers (do not force) - 30-60 seconds
- Ask patient to take deep belly breaths - on exhale, slowly sink deeper
- Move progressively to the psoas belly along the lateral border of the lumbar spine
- Hold trigger points with sustained pressure (ischemic compression) for 60-90 seconds until release
B. MET for Iliopsoas
- Lower hanging leg to first resistance barrier of hip extension
- "Gently lift your thigh upward against my hand" - isometric hip flexion at 20-30% effort, 7 seconds
- Patient fully relaxes
- Take up new slack - hip extends further
- Repeat 3-4 times
- Final stretch: 30 seconds
C. MET for Rectus Femoris
- Bring heel toward buttock to first resistance barrier of knee flexion/hip extension
- "Gently push your foot toward the floor against my hand" - isometric knee extension, 20% effort, 7 seconds
- Relax, take up new slack
- Repeat 3-4 times
BLOCK 4 - Neuromuscular Activation: Underactive Muscles (8-10 min)
A. Gluteus Maximus - Activation
- Patient prone, knee bent 90 degrees
- Therapist applies manual resistance at distal posterior thigh
- "Lift your thigh off the table" - resist through full hip extension range
- Cue: "Squeeze your glute, not your back"
- 2 sets x 10 reps
- This teaches the patient what gluteus maximus activation feels like
- Patient supine, knees bent
- Therapist taps/vibrates over gluteal mass as patient bridges up
- Tactile facilitation increases neural recruitment
- Hold at top 3 seconds, 10 reps x 2 sets
B. Anterior Tibialis - Activation with Taping (or resistance)
- Patient seated, dorsiflexion against manual resistance (or band)
- Therapist applies light resistance to dorsum of foot
- "Pull your foot up toward your shin" against resistance
- 2 x 15 reps
- Kinesio taping can be applied to tibialis anterior belly in facilitation direction (anchor at dorsal foot, apply toward tibial tuberosity with slight stretch) to maintain neural drive after session
BLOCK 5 - Re-Integration: Squat Practice (5 min)
A. Assisted Squat with Therapist Support
- Therapist faces patient, holds patient's hands
- Provides counter-balance (removes fear of falling backward)
- Guides the patient through a deep squat - they can now feel the heel staying down
- 3-5 reps - let them experience the corrected pattern neurologically
B. Wall Squat for Feedback
- Back against wall, feet 30 cm from wall
- Wall removes balance concern and provides proprioceptive cue
- 3 x 5 slow reps, hold 3 seconds at bottom
C. Squat with Heels on Thin Wedge (if still restricted)
- 1-2 cm heel elevation to demonstrate success
- Shows the patient the target movement while still reducing ankle demand slightly
- Plan to wean off wedge over subsequent sessions
Re-Assess at End (2 min)
- Repeat WBLT - expect improvement of +1.5 to +2.0 cm in dorsiflexion distance
- Perform squat - observe reduction in heel rise and improved balance
- Document before/after for patient motivation and clinical record
Single Session Timeline Summary
| Phase | Technique | Time |
|---|---|---|
| Baseline assessment | WBLT + squat observation | 2 min |
| Soft tissue - Gastroc/Soleus | Deep friction + MET | 12 min |
| Joint mobilization - Talar | A-P glide + MWM Mulligan | 10 min |
| Hip flexor release | STR + MET ilipsoas + RF | 7 min |
| Neuromuscular activation | Glute + tibialis anterior | 8 min |
| Squat re-training | Assisted + wall squat | 5 min |
| Re-assessment | WBLT + squat | 2 min |
| Total | ~46 min |
Key Clinical Principles for Maximum Same-Session Effect
-
Sequence matters - Always release before mobilize, mobilize before activate, activate before integrate. Reversing this order wastes effort.
-
Reassess between every block - If WBLT improves after talar MWM, you have objective proof and can spend less time on the next block. If it does not improve, try a different glide direction before moving on.
-
Pain-free techniques only - MWM especially must be completely pain-free. If it hurts, the joint glide angle is wrong - adjust it. Pain-free movement creates the neurological window for learning.
-
End with movement - The last thing the brain does in a session is what it retains. Always finish with the corrected squat pattern, not with passive treatment.
-
Individualize the glide direction - Evidence confirms that individualized manual therapy (glide direction chosen based on what actually improves ROM on reassessment) produces +1.7 cm dorsiflexion gain vs. +1.1-1.2 cm with a standard protocol applied to everyone.