Cardiac biomarkers
Reading File
Finding Sources
Searching the Web
cardiac biomarkers troponin BNP CRP clinical use 2024
Searching PubMed
"cardiac biomarkers" AND "troponin"
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Searching Images
cardiac biomarkers troponin BNP kinetics timeline after myocardial infarction
Loading Image
Loading Image
Here is a comprehensive overview of cardiac biomarkers, synthesized from Harrison's 22E, Goldman-Cecil Medicine, Tintinalli's Emergency Medicine, Robbins Pathology, and Tietz Textbook of Laboratory Medicine.
Cardiac Biomarkers
Cardiac biomarkers are proteins (or peptides) released from injured or stressed myocardium into the bloodstream. They serve two primary functions: diagnosis of myocardial injury/infarction and risk stratification/prognosis.
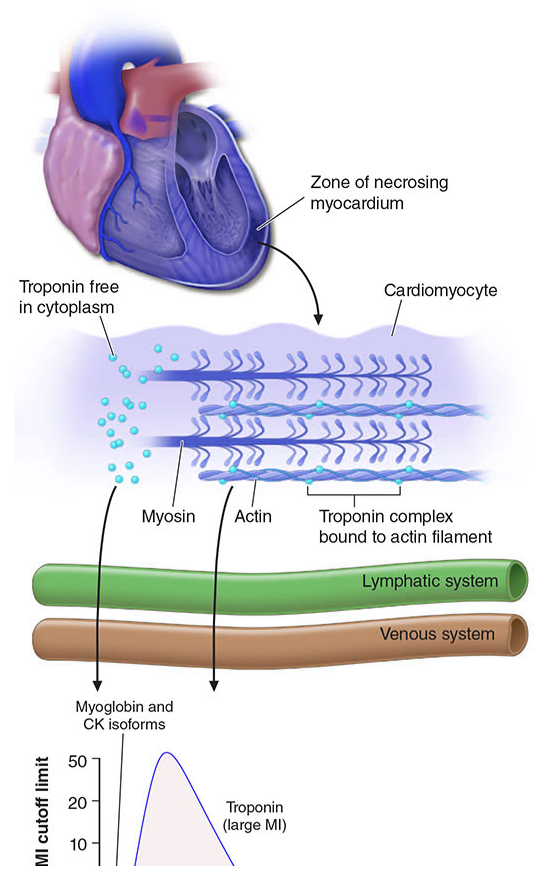
1. Mechanism of Release
When cardiomyocytes undergo necrosis, structural proteins are released into the interstitium. Biomarkers become detectable in peripheral blood once the cardiac lymphatics are overwhelmed and spillover into the venous circulation occurs. The rate of appearance depends on:
- Intracellular location (cytoplasmic vs. bound to structural complexes)
- Molecular weight
- Local blood and lymphatic flow
2. Cardiac Troponins (cTnI and cTnT) — Gold Standard
Structure & Specificity
- Cardiac troponin I (cTnI) and troponin T (cTnT) have amino-acid sequences distinct from skeletal muscle isoforms, enabling highly specific monoclonal antibody assays.
- Neither is released with skeletal muscle injury alone.
Diagnostic Criterion for AMI
- A rising and/or falling pattern with ≥1 value above the 99th percentile upper reference limit (URL) of a normal reference population.
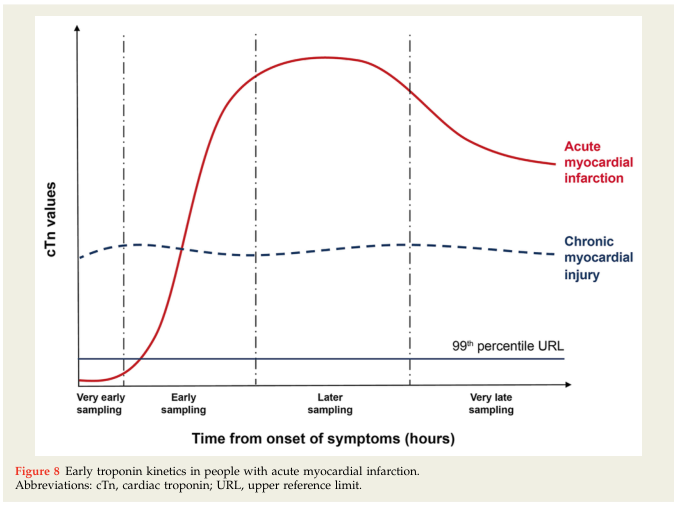
Kinetics
| Parameter | Timing |
|---|---|
| Detectable after onset | ~1–2 h (hs-cTn), 3–6 h (conventional) |
| Maximum sensitivity | 8–12 h |
| Peak | 10–24 h |
| Remains elevated | 5–14 days after STEMI (up to 7–10 days) |
High-Sensitivity Troponin (hs-cTn) Assays
- Preferred over conventional assays — greater negative predictive value.
- Rapid rule-out protocols using serial testing over 1–2 hours perform well for ACS diagnosis.
- At presentation >2–3 h after symptoms: a very low hs-cTn (single sample) can exclude MI with NPV >99%.
- In STEMI: less immediately impactful since reperfusion decisions are made before lab results return.
cTnT Caveat: Elevated in renal failure (CKD/hemodialysis); in this setting, cTnI is preferred if available.
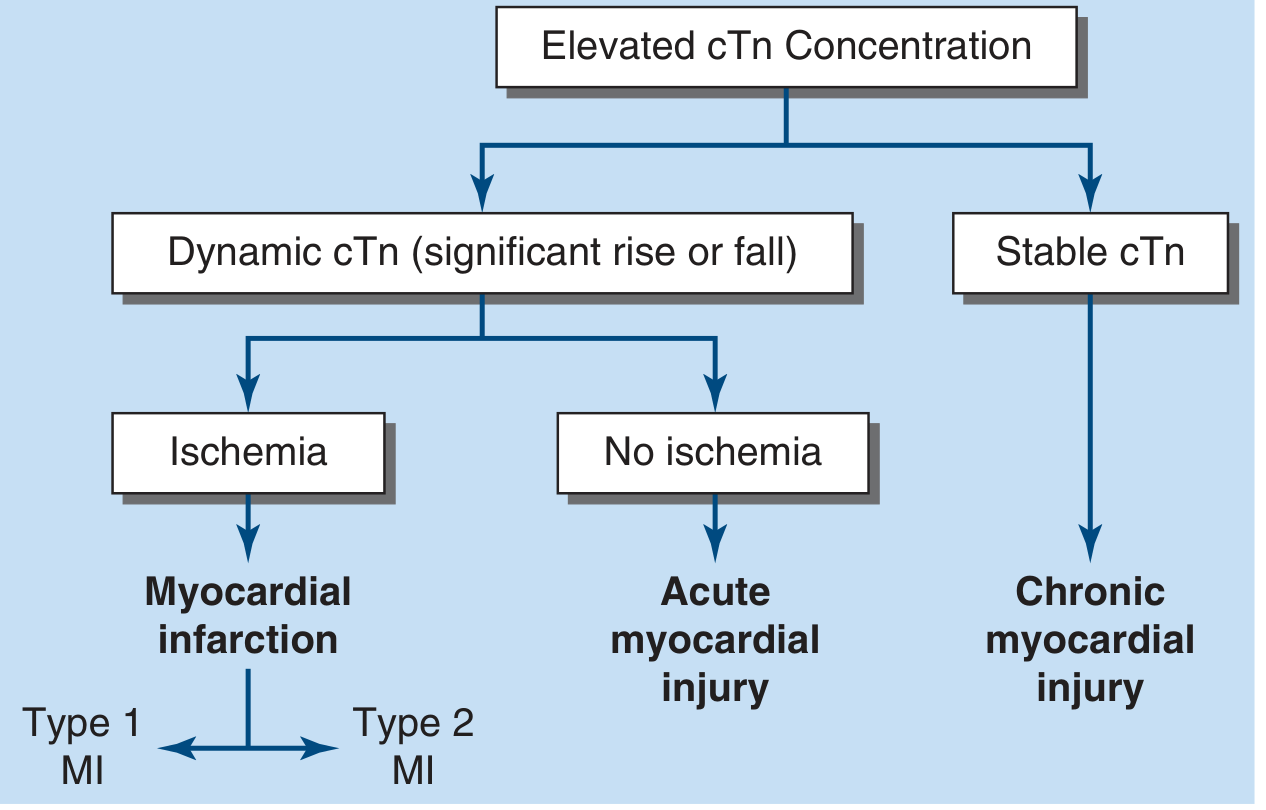
Classification of Elevated cTn:
3. Non-Ischemic Causes of Troponin Elevation ("Troponin Leak")
Troponin can rise in many non-ACS conditions. Clinical context and serial delta-troponin are critical:
| Category | Examples |
|---|---|
| Cardiac | Myocarditis, pericarditis, heart failure, cardiomyopathy, post-cardioversion/ablation |
| Pulmonary | Pulmonary embolism, severe COPD, respiratory failure |
| Renal | CKD, hemodialysis patients (particularly cTnT) |
| Neurologic | Stroke, subarachnoid/intracranial hemorrhage |
| Systemic | Septic shock, sepsis |
| Other | Rhabdomyolysis (non-specific), drug toxicity, cardiac contusion |
Key principle: Rising and falling kinetics (delta troponin) distinguish acute myocardial injury from chronic elevation. A stable, modestly elevated troponin suggests chronic structural disease rather than AMI.
4. Creatine Kinase-MB (CK-MB)
- Historically the standard for AMI diagnosis; now largely superseded by troponin.
- CK-MB relative index (CK-MB mass / total CK activity ≥2.5%) suggests myocardial rather than skeletal source — but not diagnostic alone.
- Remains useful for detecting early re-infarction: because CK-MB clears more rapidly than troponin (returns to baseline in ~48–72 h), a new rise in CK-MB during a period of still-elevated troponin suggests reinfarction.
- Limitation: Elevated in severe skeletal muscle injury, liver, diaphragm, or intestinal trauma — unreliable in multi-trauma patients.
- Not cost-effective to measure CK-MB alongside troponin routinely.
5. Myoglobin
- Earliest marker: rises within 1–2 hours of AMI onset.
- Highly sensitive but not specific — also released from skeletal muscle.
- Serum half-life: 1–3 hours; absent after ~24 hours.
- No longer recommended as a standalone diagnostic tool; largely replaced by hs-cTn.
6. B-type Natriuretic Peptide (BNP) and NT-proBNP
Physiology: BNP is secreted by ventricular myocardium in response to wall stress and volume/pressure overload. The prohormone proBNP is cleaved into active BNP-32 and the inactive fragment NT-proBNP.
Clinical Uses:
- Diagnosis of heart failure: BNP/NT-proBNP is the preferred biomarker; elevated levels support HF diagnosis when assessed alongside history and exam.
- Risk stratification in ACS: BNP provides incremental prognostic information in acute MI.
- Pulmonary embolism: BNP is a prognostic (not diagnostic) marker for PE — reflects RV wall stress.
- Preoperative cardiac risk: Canadian Cardiovascular Society (CCS) 2017 guidelines recommend BNP/NT-proBNP for further risk stratification before non-cardiac surgery.
Specimen Requirements:
- BNP: EDTA-anticoagulated whole blood or plasma (plastic tubes only).
- NT-proBNP: serum, heparin plasma, or EDTA plasma acceptable; more assays available globally.
Thresholds (approximate, assay-dependent):
- BNP <100 pg/mL: HF unlikely
- BNP >400 pg/mL: HF probable
- NT-proBNP age-adjusted cut-offs apply (>450 pg/mL for <50 yrs; >900 for 50–75 yrs; >1800 for >75 yrs)
7. Summary Comparison Table
| Biomarker | Rises | Peaks | Normalizes | Primary Use |
|---|---|---|---|---|
| Myoglobin | 1–2 h | 4–8 h | 24 h | Early sensitivity (obsolete in practice) |
| CK-MB | 3–6 h | 12–24 h | 48–72 h | Reinfarction detection |
| cTnI / cTnT | 3–6 h (conv.) / 1–2 h (hs) | 10–24 h | 5–14 days | Gold standard for AMI diagnosis |
| BNP / NT-proBNP | Hours (wall stress) | Variable | Variable | HF diagnosis, risk stratification, PE prognosis |
8. Sampling Protocol
- Conventional troponin: measure at presentation and repeat at 3–6 hours; additional measurements if clinical suspicion persists.
- High-sensitivity troponin: measure at presentation and repeat at 1–3 hours (0h/1h or 0h/2h algorithms validated).
- Serial delta-troponin (the change between samples) is as important as absolute values — a significant rise or fall defines acute injury.
Key Clinical Pearls
- Troponin is the preferred biomarker for AMI; hs-cTn assays are preferred over conventional where available.
- Context matters: always interpret troponin in light of clinical probability, ECG, and serial kinetics — an elevated troponin does not equal MI.
- CK-MB retains a niche role for diagnosing reinfarction during the troponin-elevated window.
- BNP/NT-proBNP are not for diagnosing AMI — they assess myocardial wall stress and are used for HF and risk stratification.
- In renal failure, cTnT is chronically elevated — use cTnI and serial delta values.
- In trauma, troponin I is preferred over CK/CK-MB (EAST guideline Level 2: normal troponin + normal ECG rules out significant blunt cardiac injury).
Sources: Harrison's Principles of Internal Medicine 22E, Goldman-Cecil Medicine, Tintinalli's Emergency Medicine, Robbins & Cotran Pathologic Basis of Disease, Tietz Textbook of Laboratory Medicine, Fuster & Hurst's The Heart 15E
This is a shared conversation. Sign in to Orris to start your own chat.