knee joint
Reading File
Finding Sources
Searching the Web
knee joint anatomy biomechanics overview
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
I now have comprehensive content from multiple authoritative textbooks. Let me compile the full answer.
The Knee Joint
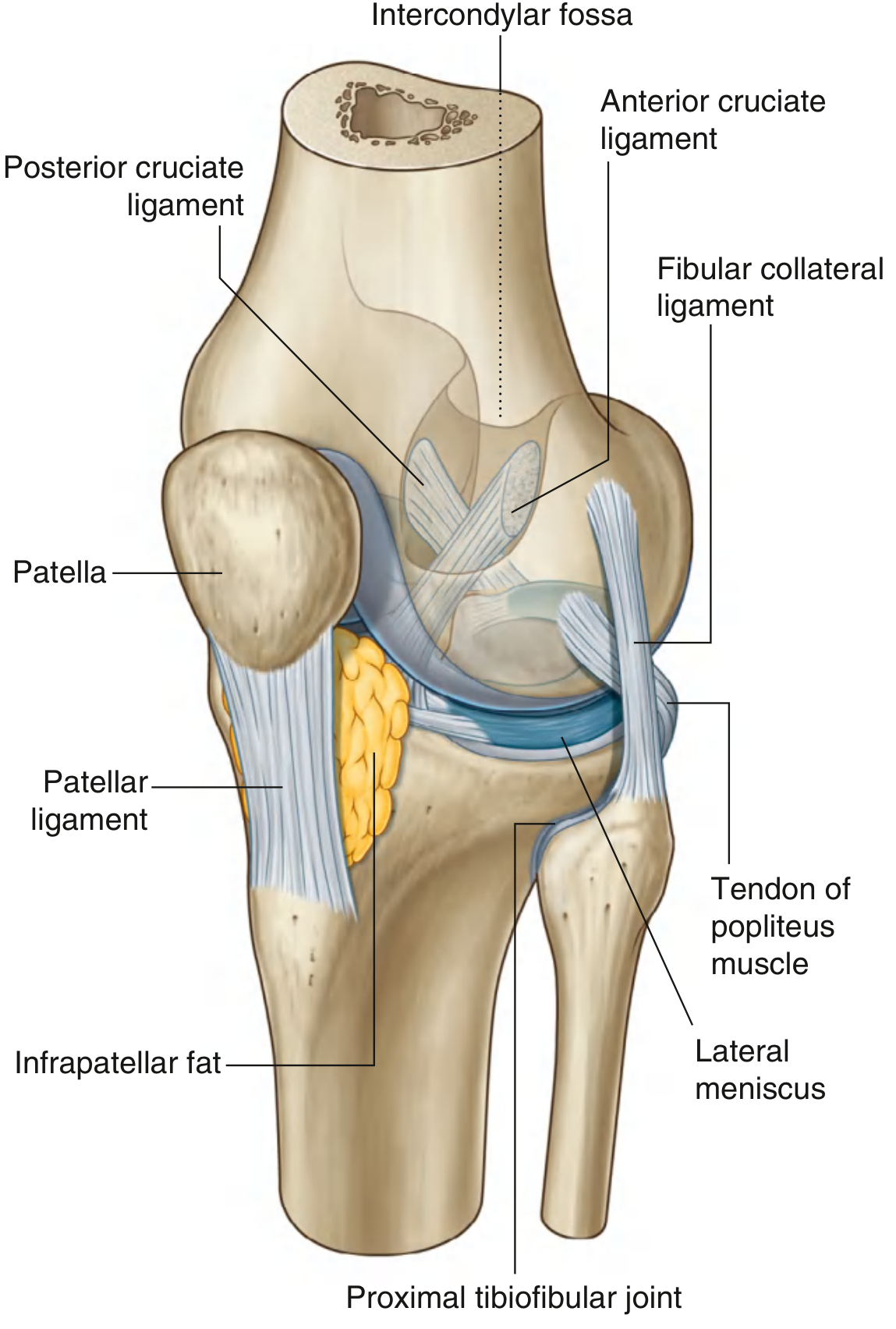
Fig. 6.73 - Knee Joint (Gray's Anatomy for Students)
Overview
The knee joint is the largest synovial joint in the body. It consists of two articulations within a single joint cavity:
- Tibiofemoral joint - between the femoral condyles and the tibial plateau (weight-bearing)
- Patellofemoral joint - between the posterior patella and the V-shaped trochlear groove of the femur (redirects the pull of quadriceps anteriorly over the knee without tendon wear)
The joint is a modified hinge joint - primarily allowing flexion and extension, with limited rotation when partially flexed. Its bony shape makes it inherently unstable; stability depends on ligaments and muscles.
- Gray's Anatomy for Students, p. 709
Articular Surfaces
All articular surfaces are covered by hyaline cartilage:
- Femoral condyles - curved surfaces in flexion, flat surfaces in full extension (this shape change is why the menisci are needed)
- Tibial condyles (tibial plateau) - medial and lateral condylar surfaces
- Posterior patella - articulates with the anterior trochlear groove of the femur
All surfaces share a single articular cavity.
Menisci
Two fibrocartilaginous C-shaped structures sit between the femoral and tibial condyles:
| Feature | Medial Meniscus | Lateral Meniscus |
|---|---|---|
| Shape | Larger, more open C | Smaller, more circular |
| Capsule attachment | Firmly attached + attached to tibial collateral ligament | NOT attached to capsule |
| Mobility | Less mobile | More mobile |
| Injury risk | More commonly torn | Less commonly torn |
Both are connected anteriorly by the transverse ligament of the knee. The lateral meniscus is also connected to the popliteus tendon.
Functions of menisci:
- Improve congruency between curved femoral condyles and flat tibial plateau
- Transmit and distribute weight-bearing forces
- Act as shock absorbers
- Improve lubrication and nutrition of articular cartilage
Meniscal tears typically occur during forceful rotation or twisting. Patterns include vertical, horizontal, and bucket-handle tears. MRI is the modality of choice; arthroscopy is used for repair or debridement.
- Gray's Anatomy for Students, p. 710-711
Ligaments
Cruciate Ligaments (Intra-articular, Extra-synovial)
| Ligament | Attachment | Function |
|---|---|---|
| ACL (Anterior Cruciate) | Anterior tibial intercondylar area → posterior lateral femoral condyle | Prevents anterior tibial displacement on femur; limits internal rotation |
| PCL (Posterior Cruciate) | Posterior tibial intercondylar area → anterior medial femoral condyle | Prevents posterior tibial displacement; strongest ligament of the knee |
Both cruciate ligaments lie within the fibrous capsule but outside the synovial cavity - the synovial membrane loops forward around them.
Collateral Ligaments (Extra-articular)
| Ligament | Description | Function |
|---|---|---|
| Tibial (Medial) Collateral | Broad, flat; fused to medial meniscus and capsule | Resists valgus stress; taut in extension |
| Fibular (Lateral) Collateral | Cord-like; NOT attached to lateral meniscus | Resists varus stress; taut in extension |
Other Ligaments
- Patellar ligament - continuation of the quadriceps tendon; attaches patella to tibial tuberosity
- Oblique popliteal ligament - posterior reinforcement
- Arcuate popliteal ligament - posterolateral reinforcement
Synovial Membrane & Bursae
The synovial membrane attaches to articular margins and to the outer edges of the menisci. Important associated bursae:
- Suprapatellar bursa - large, communicates with joint cavity; continuous superiorly between femur and quadriceps tendon. The articularis genus muscle prevents it from getting trapped during extension
- Prepatellar bursa - subcutaneous, anterior to patella ("housemaid's knee" when inflamed)
- Infrapatellar bursae - deep and superficial, around the patellar ligament
- Subpopliteal recess - posterolateral, between lateral meniscus and popliteus tendon
- Semimembranosus bursa - posteromedial; enlarged bursa becomes more prominent on extension and disappears in flexion
The infrapatellar fat pad separates the patellar ligament from the synovial membrane anteriorly. Alar folds project into the articular cavity on each side of the fat pad.
- Gray's Anatomy for Students, p. 712-713
Muscles (Stabilizers)
Static stabilizers: joint capsule, menisci, cruciate ligaments, collateral ligaments
Dynamic stabilizers:
- Quadriceps femoris (via patellar ligament) - primary extensor; patella increases lever arm
- Hamstrings (semimembranosus, semitendinosus, biceps femoris) - primary flexors; also aid in rotation
- Popliteus - "unlocks" the knee from full extension by internally rotating the tibia; passes between lateral meniscus and capsule
- Gastrocnemius - weak flexor; two heads arise from femoral condyles
Movements & Biomechanics
Range of motion: 5° hyperextension to 135° flexion (normal)
| Movement | Range | Key Muscles |
|---|---|---|
| Flexion | 0-135° | Hamstrings, popliteus, gastrocnemius |
| Extension | 0-5° hyperextension | Quadriceps femoris |
| Internal rotation (tibia) | Increases with flexion | Popliteus, semimembranosus |
| External rotation (tibia) | Increases with flexion | Biceps femoris |
Screw-home mechanism: During the final 10-15° of extension, the tibia externally rotates and "locks" the knee in a close-packed (fully extended) position. This reduces muscle energy needed to maintain standing. Popliteus initiates flexion by internally rotating the tibia to "unlock" the joint.
Kinematics: Knee motion is predominantly in the sagittal plane. During flexion, the femur undergoes a combination of rolling and sliding on the tibia, plus internal tibial rotation. The larger medial femoral condyle rolls back less than the smaller lateral condyle, contributing to this rotation.
Patellofemoral mechanics: The patella functions as a pulley for the quadriceps, increasing its lever arm and thus its power. The patella has the thickest articular cartilage in the body.
Mechanical axis of the lower limb runs from the femoral head center through the intercondylar notch to the ankle center. The anatomical and mechanical axes of the femur diverge by 5-7° (the valgus cut angle used in total knee replacement). Malalignment (genu valgum/varum) accelerates wear in the loaded compartment.
- Bailey & Love's Short Practice of Surgery 28th Ed, p. (Biomechanics section)
Clinical Examination of the Knee
Common symptoms: Pain, swelling, stiffness, locking, giving way, clicking, limp
Inspection
- Gait: stiff knee = leg swings outward; other conditions = lurch to sound side
- Attitude: arthritic joints adopt moderate flexion (optimum position for maximum fluid accommodation)
- "Triple displacement" of late arthritis (e.g., TB knee): flexion + posterior subluxation + lateral rotation of tibia - indicates cruciate and collateral ligament destruction
- Genu valgum (knock-knee), genu varum (bow-leg), genu recurvatum (back-knee)
- Effusion: horse-shoe swelling above and around the patella, obliterating normal hollows on either side of the patellar ligament
Palpation
- Patellar tap test: pathognomonic of joint effusion. Compress suprapatellar pouch to drive fluid into joint cavity, then press patella sharply down - it "taps" on the femur
- Fluctuation test: for smaller effusions
- Synovial thickening: spongy/boggy feel, no patellar tap, edge can be rolled under finger
- Joint line tenderness: suggests meniscal tear or arthritis
- Patellofemoral crepitus: suggests chondromalacia patellae
Movements
Flexion, extension, and limited rotation are tested. Range of motion and quality of movement are assessed with the patient in supine and prone positions.
- S Das: A Manual on Clinical Surgery 13th Ed, p. 253-256
Common Clinical Conditions
| Condition | Key Features |
|---|---|
| Meniscal tear | Twisting injury; joint line pain; locking; McMurray's / Thessaly tests; MRI diagnosis |
| ACL tear | Anterior drawer test, Lachman test positive; pivot shift |
| PCL tear | Posterior sag; posterior drawer test |
| Medial/Lateral collateral ligament tear | Valgus/varus stress tests |
| Osteoarthritis | Joint line tenderness, crepitus, osteophytes on X-ray; common medial compartment |
| Rheumatoid arthritis | Synovitis, morning stiffness, bilateral involvement |
| Prepatellar bursitis | "Housemaid's knee"; swelling anterior to patella |
| Baker's cyst | Distended semimembranosus bursa; posteromedial swelling |
| Chondromalacia patellae | Anterior knee pain; crepitus; positive Clarke's test |
| Patellar dislocation | Usually lateral; apprehension sign |
| Genu valgum/varum | Malalignment accelerates compartmental OA |
Blood Supply & Nerve Supply
Blood supply: Genicular anastomosis - branches from the popliteal artery (medial and lateral superior/inferior genicular arteries) + descending genicular (femoral), anterior tibial recurrent, and circumflex fibular arteries
Nerve supply: Femoral, obturator, common fibular (peroneal), and tibial nerves. The Hilton's law applies: nerves supplying the knee also supply the hip and ankle - explaining referred pain patterns.
Sources: Gray's Anatomy for Students | Bailey & Love's Short Practice of Surgery, 28th Ed | S Das: A Manual on Clinical Surgery, 13th Ed | Campbell's Operative Orthopaedics, 15th Ed 2026
This is a shared conversation. Sign in to Orris to start your own chat.