Create a clinical case with a diagnosis of acute tubulointerstitial nephritis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Here is a complete clinical case of acute tubulointerstitial nephritis (ATIN).
Clinical Case: Acute Tubulointerstitial Nephritis
Patient Presentation
Patient: Maria G., 52-year-old woman
Chief complaint: Fatigue, decreased urine output, and low-grade fever for 10 days
History of present illness:
Three weeks ago, the patient was prescribed omeprazole 20 mg/day for gastroesophageal reflux and trimethoprim-sulfamethoxazole (TMP-SMX) for a urinary tract infection. Ten days after starting these medications she developed generalized fatigue, oliguria, bilateral flank discomfort, mild fever (38.2 °C), and a diffuse maculopapular rash on her trunk. She denies dysuria, vomiting, or diarrhea. No prior kidney disease.
Past medical history: Hypertension (lisinopril), type 2 diabetes (metformin), recurrent UTIs
Medications: Lisinopril 10 mg/day, metformin 500 mg BID, omeprazole 20 mg/day (new), TMP-SMX DS (new)
Allergies: No known drug allergies prior to this episode
Physical Examination
| Finding | Result |
|---|---|
| Temperature | 38.2 °C |
| Blood pressure | 148/92 mmHg |
| Heart rate | 94 bpm |
| Respiratory rate | 18 rpm |
| Bilateral costovertebral angle tenderness | Present (mild) |
| Skin | Diffuse maculopapular rash, trunk and upper limbs |
| Eyes | No uveitis, no injection |
| Edema | Absent |
Laboratory Results
| Test | Result | Reference |
|---|---|---|
| Serum creatinine | 3.4 mg/dL | 0.6–1.1 mg/dL |
| BUN | 48 mg/dL | 7–20 mg/dL |
| eGFR | 18 mL/min/1.73 m² | >60 |
| Serum potassium | 5.6 mEq/L | 3.5–5.0 mEq/L |
| Serum sodium | 138 mEq/L | 135–145 mEq/L |
| Bicarbonate (HCO₃⁻) | 16 mEq/L | 22–28 mEq/L |
| Chloride | 112 mEq/L | 98–107 mEq/L |
| Serum IgE | Elevated | Normal |
| Complete blood count | WBC 11,200/μL; Eosinophils 12% | Eosinophils <5% |
| Serum albumin | 3.8 g/dL | 3.5–5.0 g/dL |
Urine analysis (midstream):
| Finding | Result |
|---|---|
| Color | Amber, turbid |
| Leukocyte esterase | +++ |
| RBCs | 10–15/HPF (non-dysmorphic) |
| WBCs | 25–30/HPF |
| Eosinophiluria | Present (Hansel stain) |
| WBC casts | Present |
| Proteinuria | +1 (trace/mild, < 1 g/24 h) |
| β₂-microglobulin | Elevated (indicating proximal tubular dysfunction) |
Spot urine sodium: 42 mEq/L (FENa > 2%, consistent with intrinsic renal injury)
Imaging
Renal ultrasound:
- Kidneys bilaterally enlarged (right 12.1 cm; left 12.4 cm), echogenic parenchyma
- No hydronephrosis, no stones, no masses
- Normal vascular flow on Doppler
Renal Biopsy
Biopsy was performed given rapid AKI without a clear single offending agent.
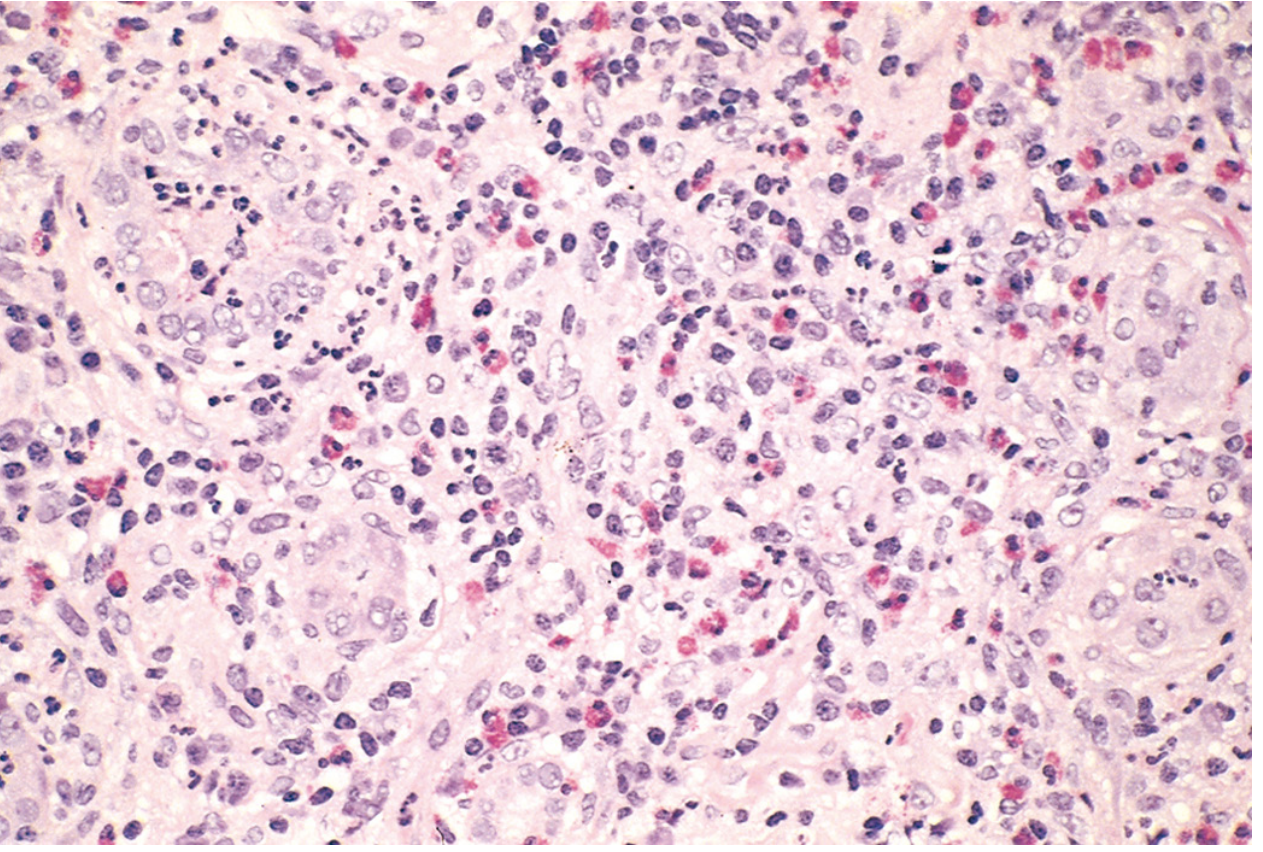
Histopathology findings:
- Interstitium: Pronounced edema with dense mononuclear infiltrate (lymphocytes, macrophages). Prominent eosinophils and neutrophils present in clusters.
- Tubules: Tubulitis (lymphocytic infiltration into tubular epithelium); variable tubular injury and early regenerative changes.
- Glomeruli: Normal morphology (no glomerulonephritis).
- Vessels: No vasculitis.
- Granulomas: Absent in this case.
Diagnosis
Acute Tubulointerstitial Nephritis (ATIN) — Drug-induced (TMP-SMX and/or proton pump inhibitor)
Pathophysiology
The drugs (secreted by renal tubules) bind covalently to cytoplasmic or extracellular components of tubular cells, creating immunogenic neo-antigens. The resulting injury is mediated by:
- Type I hypersensitivity (IgE-mediated): Elevated serum IgE, eosinophilia, and skin rash suggest involvement of this arm.
- Type IV hypersensitivity (T cell–mediated): The dense mononuclear interstitial infiltrate and tubulitis are characteristic of delayed-type hypersensitivity.
Key features supporting a hypersensitivity mechanism:
- Latent period of ~10 days after drug initiation
- Idiosyncratic reaction (not dose-dependent)
- Triad of fever + rash + eosinophilia (present in ~25% of cases)
- Recurrence expected upon re-exposure
Tubular dysfunction manifests as:
- Impaired urine concentration → polyuria/nocturia
- Impaired acid excretion → hyperchloremic metabolic acidosis (non-anion gap)
- Impaired potassium handling → hyperkalemia
- β₂-microglobulinuria → proximal tubule dysfunction
— Robbins, Cotran & Kumar Pathologic Basis of Disease; Harrison's Principles of Internal Medicine, 22nd ed.
Differential Diagnosis
| Condition | Features distinguishing from ATIN |
|---|---|
| Acute glomerulonephritis | Nephritic syndrome, dysmorphic RBCs, RBC casts, heavy proteinuria |
| Acute pyelonephritis | Positive urine culture, bacteria, fever, no eosinophils; usually no AKI this severe |
| Prerenal AKI | FENa < 1%, low urine Na, responds to fluids |
| Acute tubular injury (ATI) | Granular "muddy brown" casts, no eosinophilia, no rash, often ischemic/nephrotoxic cause |
| IgG4-related TIN | Elevated IgG4, fibrosis, often older males |
| TINU syndrome | Tubulointerstitial nephritis + uveitis; typically adolescent girls |
Management
- Immediate cessation of offending drugs (TMP-SMX and omeprazole) — the most critical step. Recovery may take weeks to several months.
- Corticosteroids: Prednisone 1 mg/kg/day (up to 60 mg/day) for 4–8 weeks with gradual taper, considered when renal function fails to improve within 1 week of drug withdrawal or in severe AKI.
- Supportive measures:
- IV fluids with close monitoring of fluid balance
- Dietary potassium restriction; consider potassium binders if K⁺ remains elevated
- Discontinue lisinopril temporarily (RAAS blockade may worsen hyperkalemia and AKI)
- Hold metformin until renal function recovers (risk of lactic acidosis)
- Close monitoring: Serum creatinine, electrolytes, and urinalysis every 48–72 hours during acute phase.
- Avoidance of re-exposure to sulfonamides and PPIs; document allergy in medical record.
- Nephrology referral given AKI stage 3 (creatinine 3.4 mg/dL from presumed baseline ~0.9 mg/dL).
Teaching Points
- ATIN accounts for up to 15–20% of AKI cases and is the second most common cause of drug-induced AKI after pyelonephritis. — Robbins, Cotran & Kumar Pathologic Basis of Disease
- The classic triad (fever, rash, eosinophilia) is present in only ~25% of patients; its absence does not exclude the diagnosis.
- PPIs and sulfa drugs are among the most frequent culprits today; immune checkpoint inhibitors are an increasingly recognized cause in oncology patients.
- Eosinophiluria (Hansel stain) supports the diagnosis but has limited sensitivity.
- Tubular dysfunction (non-anion gap acidosis, impaired concentration, β₂-microglobulinuria) distinguishes TIN from glomerulonephritis.
- Glomeruli are normal on biopsy unless NSAIDs are the cause, in which case concurrent minimal change disease and nephrotic syndrome may develop.
- Early recognition and drug withdrawal are the key determinants of reversibility.
Make a little shorter
Clinical Case: Acute Tubulointerstitial Nephritis
Patient Presentation
Patient: Maria G., 52-year-old woman
Chief complaint: Fatigue, oliguria, and low-grade fever for 10 days
Three weeks ago she was prescribed omeprazole and TMP-SMX for a UTI. Ten days later she developed fatigue, decreased urine output, bilateral flank discomfort, fever (38.2 °C), and a diffuse maculopapular rash on her trunk. No prior kidney disease.
Medications: Lisinopril, metformin, omeprazole (new), TMP-SMX DS (new)
Physical Examination
- Temperature 38.2 °C, BP 148/92 mmHg
- Bilateral costovertebral angle tenderness (mild)
- Diffuse maculopapular rash on trunk and upper limbs
- No edema, no uveitis
Laboratory & Urinalysis
| Test | Result |
|---|---|
| Serum creatinine | 3.4 mg/dL ↑ |
| eGFR | 18 mL/min/1.73 m² |
| K⁺ | 5.6 mEq/L ↑ |
| HCO₃⁻ | 16 mEq/L ↓ (non-anion gap metabolic acidosis) |
| Eosinophils | 12% ↑ |
| Serum IgE | Elevated |
| Urinalysis | WBCs 25–30/HPF, RBCs 10–15/HPF, WBC casts, eosinophiluria (Hansel stain +), mild proteinuria (+1), elevated β₂-microglobulin |
| FENa | > 2% (intrinsic renal injury) |
Renal ultrasound: Bilaterally enlarged kidneys, echogenic parenchyma, no hydronephrosis.
Renal Biopsy
- Pronounced interstitial edema with dense lymphocytic and macrophage infiltrate; eosinophils and neutrophils in clusters
- Tubulitis (lymphocytes infiltrating tubular epithelium); variable tubular injury
- Normal glomeruli; no granulomas; no vasculitis
Diagnosis
Acute Tubulointerstitial Nephritis — Drug-induced (TMP-SMX / PPI)
Pathophysiology
The drugs are secreted by renal tubules, bind to tubular cell components, and create immunogenic neo-antigens. Injury results from:
- Type I hypersensitivity (IgE-mediated): explains elevated IgE, eosinophilia, and rash
- Type IV hypersensitivity (T cell–mediated): explains the interstitial mononuclear infiltrate and tubulitis
The reaction is idiosyncratic (not dose-dependent), with a latent period of days to weeks and recurrence upon re-exposure. — Robbins, Cotran & Kumar Pathologic Basis of Disease
Management
- Stop the offending drugs immediately — the most critical step
- Corticosteroids (prednisone 1 mg/kg/day) if creatinine does not improve within ~1 week of drug withdrawal
- Hold lisinopril and metformin until renal function recovers
- Fluid balance management and electrolyte correction (K⁺, HCO₃⁻)
- Nephrology referral; document allergy and avoid re-exposure
Key Teaching Points
- The classic triad of fever + rash + eosinophilia is present in only ~25% of patients — its absence does not exclude ATIN
- PPIs and sulfa drugs are among the most common culprits today; immune checkpoint inhibitors are increasingly recognized
- Tubular dysfunction (non-anion gap acidosis, hyperkalemia, β₂-microglobulinuria) distinguishes ATIN from glomerulonephritis
- Glomeruli are normal on biopsy unless NSAIDs are the cause (concurrent minimal change disease may occur)
- Early drug withdrawal is the key determinant of reversibility; recovery may take several months — Harrison's Principles of Internal Medicine, 22nd ed.
Now make a case about chronic
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Searching Images
chronic tubulointerstitial nephritis fibrosis histology biopsy
Reading File
Loading Image
Clinical Case: Chronic Tubulointerstitial Nephritis
Patient Presentation
Patient: Roberto A., 61-year-old man
Chief complaint: Progressive fatigue, nocturia, and slowly worsening renal function over 3 years
He reports daily use of a combination analgesic (aspirin + acetaminophen + caffeine) for chronic lower back pain for at least 8 years ("at least 6 tablets a day"). He minimized this use during previous medical consultations. Over the past year he has noted increasing nocturia (3–4 times/night), difficulty concentrating urine, and mild nausea. No fever, no rash, no gross hematuria.
Past medical history: Chronic low back pain, hypertension, type 2 diabetes
Medications: Amlodipine, metformin, over-the-counter analgesic combination (heavy long-term use)
Physical Examination
- BP 162/96 mmHg; HR 78 bpm; afebrile
- Pallor of mucous membranes (anemia)
- No significant edema
- No costovertebral angle tenderness
- No rash or uveitis
Laboratory & Urinalysis
| Test | Result |
|---|---|
| Serum creatinine | 3.1 mg/dL ↑ (baseline 1.2 mg/dL 3 years ago) |
| eGFR | 22 mL/min/1.73 m² |
| BUN | 44 mg/dL ↑ |
| K⁺ | 5.2 mEq/L ↑ |
| HCO₃⁻ | 17 mEq/L ↓ (non-anion gap metabolic acidosis / distal RTA) |
| Uric acid | 9.1 mg/dL ↑ |
| Hemoglobin | 9.4 g/dL ↓ (out of proportion to degree of CKD) |
| Urinalysis | Fixed specific gravity ~1.010, glycosuria (normal serum glucose), mild proteinuria (<1 g/day), occasional RBCs and WBCs, granular casts |
| β₂-microglobulin (urine) | Elevated (proximal tubular dysfunction) |
No eosinophilia. No eosinophiluria.
Imaging
Renal ultrasound / CT without contrast:
- Bilateral small kidneys (right 8.6 cm; left 8.9 cm) with irregular cortical contour and atrophic scars
- Increased parenchymal echogenicity
- Papillary calcifications visible on CT (characteristic of analgesic nephropathy)
- No hydronephrosis
Renal Biopsy
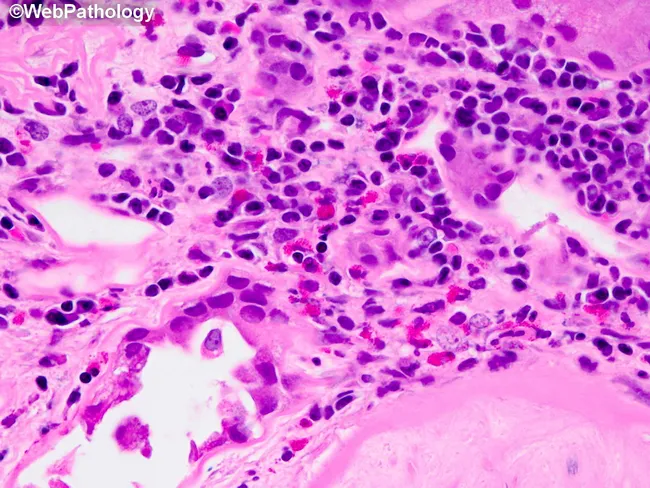
Histopathology findings:
- Interstitium: Diffuse tubulointerstitial fibrosis with collagen deposition; scattered chronic infiltrate of lymphocytes and macrophages (less abundant than in acute TIN)
- Tubules: Tubular atrophy with loss of tubular epithelium; dilated tubular lumens in some areas
- Glomeruli: Relatively spared early; global sclerosis in advanced foci
- Vessels: Hyaline arteriolosclerosis (related to hypertension)
- No eosinophils, no granulomas
— Goldman-Cecil Medicine; Brenner and Rector's The Kidney
Diagnosis
Chronic Tubulointerstitial Nephritis — Analgesic nephropathy (chronic combination analgesic use)
Pathophysiology
Long-term ingestion of combination analgesics (aspirin + acetaminophen ± caffeine) produces:
- Toxic metabolites (particularly from acetaminophen) that concentrate in the renal medulla via the normal urinary concentrating mechanism — medullary cells are selectively exposed to high toxic concentrations
- Medullary ischemia — aspirin inhibits prostaglandin-mediated vasodilation of vasa recta, reducing medullary blood flow
- Papillary necrosis — combined ischemia and toxicity leads to coagulative necrosis of the papillae, with eventual sloughing and calcification
- Over years: progressive cortical scarring, fibrosis, and CKD
The reaction is dose- and duration-dependent (typically >6 tablets/day for >3 years), unlike the idiosyncratic reaction of acute TIN. — Harrison's Principles of Internal Medicine, 22nd ed.
Management
- Complete cessation of all analgesic combinations — the single most important intervention; progression may halt if stopped early
- BP control — target <130/80 mmHg; avoid NSAIDs; ACE inhibitor or ARB preferred for renoprotection
- Correct metabolic acidosis — oral sodium bicarbonate supplementation
- Anemia management — erythropoiesis-stimulating agents ± iron if EPO-deficient anemia confirmed
- Hold metformin given eGFR <30 mL/min/1.73 m²
- Screen for urothelial malignancy — increased risk of transitional cell carcinoma of renal pelvis, distal ureter, and bladder in analgesic nephropathy; urine cytology + cystoscopy
- Nephrology referral for CKD stage 4 management and preparation for renal replacement therapy planning
Key Teaching Points
- Chronic TIN is insidious — patients often present with advanced CKD; analgesic use frequently goes unreported
- Anemia out of proportion to the degree of renal failure is a characteristic early clue
- Tubular dysfunction precedes significant GFR loss: nocturia, fixed specific gravity, glycosuria, RTA, and β₂-microglobulinuria
- The classic CT finding is bilateral small kidneys with papillary calcifications and irregular cortical scarring
- On biopsy: interstitial fibrosis replaces the acute inflammatory infiltrate — far less cellular than acute TIN
- Chronic analgesic use raises the risk of uroepithelial malignancy — screening is mandatory
- Unlike acute TIN, there is no fever, rash, or eosinophilia; the course is slow and smoldering — Goldman-Cecil Medicine
Remove key teaching points
Clinical Case: Chronic Tubulointerstitial Nephritis
Patient Presentation
Patient: Roberto A., 61-year-old man
Chief complaint: Progressive fatigue, nocturia, and slowly worsening renal function over 3 years
He reports daily use of a combination analgesic (aspirin + acetaminophen + caffeine) for chronic lower back pain for at least 8 years ("at least 6 tablets a day"). He minimized this use during previous medical consultations. Over the past year he has noted increasing nocturia (3–4 times/night), difficulty concentrating urine, and mild nausea. No fever, no rash, no gross hematuria.
Past medical history: Chronic low back pain, hypertension, type 2 diabetes
Medications: Amlodipine, metformin, over-the-counter analgesic combination (heavy long-term use)
Physical Examination
- BP 162/96 mmHg; HR 78 bpm; afebrile
- Pallor of mucous membranes (anemia)
- No significant edema
- No costovertebral angle tenderness
- No rash or uveitis
Laboratory & Urinalysis
| Test | Result |
|---|---|
| Serum creatinine | 3.1 mg/dL ↑ (baseline 1.2 mg/dL 3 years ago) |
| eGFR | 22 mL/min/1.73 m² |
| BUN | 44 mg/dL ↑ |
| K⁺ | 5.2 mEq/L ↑ |
| HCO₃⁻ | 17 mEq/L ↓ (non-anion gap metabolic acidosis / distal RTA) |
| Uric acid | 9.1 mg/dL ↑ |
| Hemoglobin | 9.4 g/dL ↓ (out of proportion to degree of CKD) |
| Urinalysis | Fixed specific gravity ~1.010, glycosuria (normal serum glucose), mild proteinuria (<1 g/day), occasional RBCs and WBCs, granular casts |
| β₂-microglobulin (urine) | Elevated (proximal tubular dysfunction) |
No eosinophilia. No eosinophiluria.
Imaging
Renal ultrasound / CT without contrast:
- Bilateral small kidneys (right 8.6 cm; left 8.9 cm) with irregular cortical contour and atrophic scars
- Increased parenchymal echogenicity
- Papillary calcifications visible on CT (characteristic of analgesic nephropathy)
- No hydronephrosis
Renal Biopsy
Histopathology findings:
- Interstitium: Diffuse tubulointerstitial fibrosis with collagen deposition; scattered chronic infiltrate of lymphocytes and macrophages (less abundant than in acute TIN)
- Tubules: Tubular atrophy with loss of tubular epithelium; dilated tubular lumens in some areas
- Glomeruli: Relatively spared early; global sclerosis in advanced foci
- Vessels: Hyaline arteriolosclerosis (related to hypertension)
- No eosinophils, no granulomas
— Goldman-Cecil Medicine; Brenner and Rector's The Kidney
Diagnosis
Chronic Tubulointerstitial Nephritis — Analgesic nephropathy (chronic combination analgesic use)
Pathophysiology
Long-term ingestion of combination analgesics (aspirin + acetaminophen ± caffeine) produces:
- Toxic metabolites that concentrate in the renal medulla via the normal urinary concentrating mechanism — medullary cells are selectively exposed to high toxic concentrations
- Medullary ischemia — aspirin inhibits prostaglandin-mediated vasodilation of vasa recta, reducing medullary blood flow
- Papillary necrosis — combined ischemia and toxicity leads to coagulative necrosis of the papillae, with eventual sloughing and calcification
- Over years: progressive cortical scarring, fibrosis, and CKD
The reaction is dose- and duration-dependent (typically >6 tablets/day for >3 years), unlike the idiosyncratic reaction of acute TIN. — Harrison's Principles of Internal Medicine, 22nd ed.
Management
- Complete cessation of all analgesic combinations — the single most important intervention
- BP control — target <130/80 mmHg; avoid NSAIDs; ACE inhibitor or ARB preferred for renoprotection
- Correct metabolic acidosis — oral sodium bicarbonate supplementation
- Anemia management — erythropoiesis-stimulating agents ± iron if EPO-deficient anemia confirmed
- Hold metformin given eGFR <30 mL/min/1.73 m²
- Screen for urothelial malignancy — increased risk of transitional cell carcinoma of renal pelvis, distal ureter, and bladder; urine cytology + cystoscopy
- Nephrology referral for CKD stage 4 management and renal replacement therapy planning
This is a shared conversation. Sign in to Orris to start your own chat.