Cat cut injury with tendon cause inability to move fingers
Reading File
Finding Sources
Finding Sources
Searching PubMed
"flexor tendon" AND "laceration" AND "repair"
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have comprehensive textbook information. Let me compile a thorough answer.
Flexor Tendon Laceration - Complete Clinical Guide
A "cat cut" (sharp laceration, often from glass, knife, or cat scratch/bite) over the palmar side of the hand or finger that severs a flexor tendon produces inability to flex (bend) the finger because the muscle-to-bone force transmission is physically interrupted. This is a true hand surgery emergency.
Anatomy - Why the Finger Can't Move
Two flexor tendons run through each finger inside a fibro-osseous tunnel (the flexor sheath):
| Tendon | Insertion | Action |
|---|---|---|
| Flexor Digitorum Profundus (FDP) | Base of distal phalanx | Flexes DIP joint |
| Flexor Digitorum Superficialis (FDS) | Base of middle phalanx | Flexes PIP joint |
When either or both are cut, the relevant joint cannot bend. The finger loses its natural resting cascade posture (the slightly curved "waterfall" alignment of the fingers at rest).
Clinical Signs
- Loss of the digital cascade - the injured finger sits extended/straight while others remain in natural flexion at rest
- FDP test: Hold MCP and PIP joints in extension - ask patient to flex the DIP joint only. Inability = FDP cut
- FDS test: Hold all other fingers in full extension (to neutralize FDP), then ask to flex at PIP. Inability = FDS cut
- Weakness or pain with resisted flexion may indicate a partial laceration (which can be clinically silent but still dangerous if untreated)
Tendon Injury Zones
The hand is divided into 5 zones, which determine repair difficulty and prognosis:
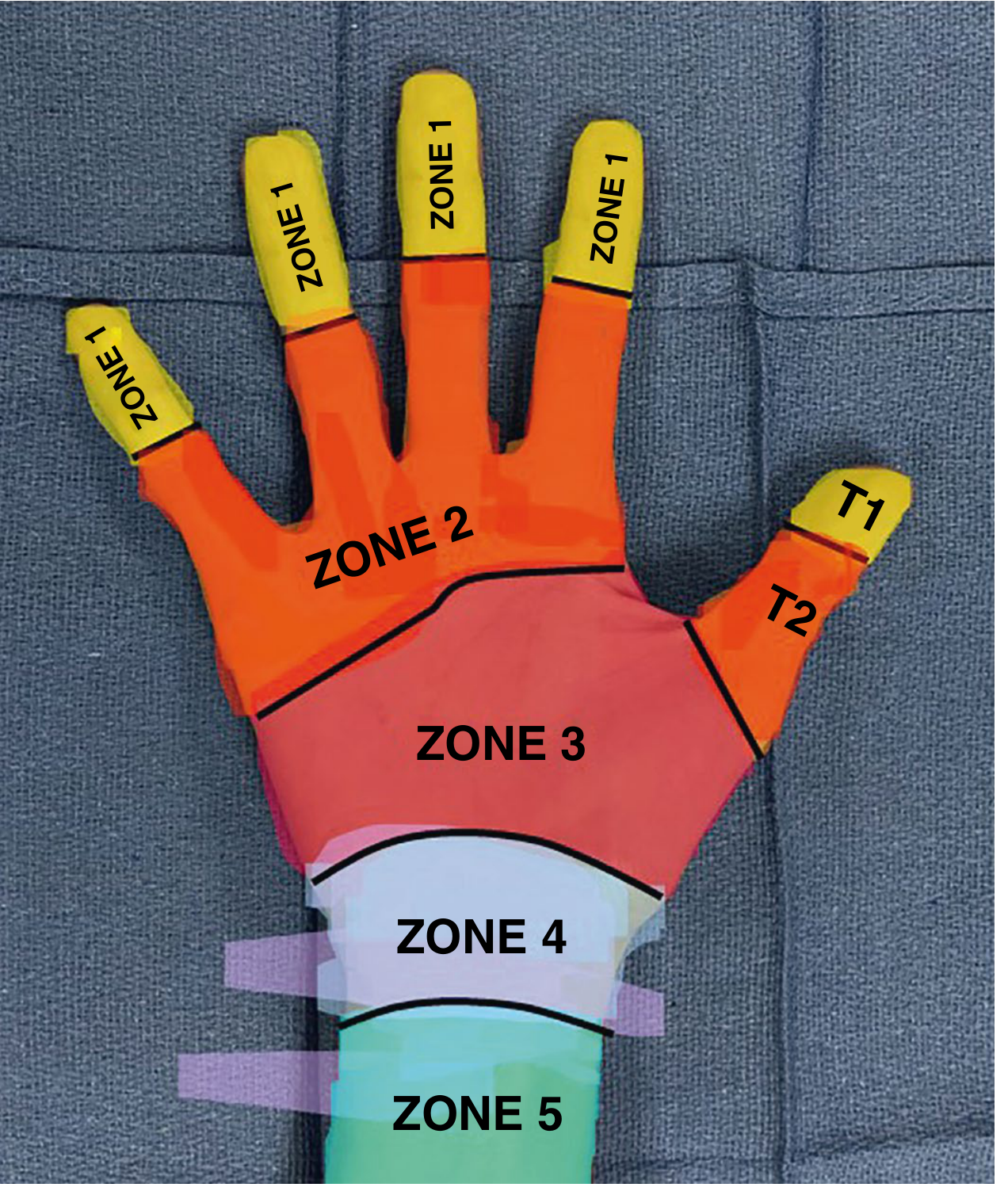
| Zone | Location | Key Notes |
|---|---|---|
| Zone 1 | Distal to FDS insertion (fingertip) | Only FDP injured; "jersey finger"; blood supply at risk |
| Zone 2 | Distal palm to mid-middle phalanx | Historically "no man's land" - tight sheath, technically demanding repair |
| Zone 3 | Distal to carpal tunnel → proximal flexor sheath | Generally good outcomes |
| Zone 4 | Carpal tunnel | Median nerve injury common |
| Zone 5 | Proximal to carpal tunnel | Often multiple tendons + nerve/vessel involvement |
- Sabiston Textbook of Surgery, p. 1187-1194
Emergency Management
Immediate steps in the ED:
- Do NOT close the wound and discharge without tendon assessment - partial lacerations can be clinically silent yet still catastrophic if missed
- Examine position-dependently - test the tendon with the hand in the same position as when the injury occurred (the cut tendon end moves with the finger)
- Splint in blocking position to prevent further retraction:
- Wrist neutral to slightly flexed
- MCP joints flexed 70-90°
- IP joints minimally flexed 10-15°
- Thumb spica if thumb involved
- Antibiotics for open wounds: Cephalexin 500 mg TID x 7-10 days (doxycycline 100 mg BID x 7-10 days if penicillin-allergic)
- X-ray to rule out avulsion fractures
Urgency of hand surgery referral:
| Situation | Timing |
|---|---|
| Open fracture, dislocation, arterial injury, grossly contaminated, or bite wound | Emergency consult same day |
| Clean laceration with confirmed tendon injury | Follow-up within 3 days |
| Zone 1 avulsion with disrupted blood supply | Surgery within 7-10 days |
| Delayed presentation | Within 2-3 weeks maximum (after this, scarring + retraction require tendon grafting) |
- Rosen's Emergency Medicine, pp. 3040-3049
Surgical Repair
- Primary repair (within 24 hours): end-to-end tenorrhaphy using a core strand suture technique
- Delayed primary repair (up to 3 weeks): acceptable when experienced specialist unavailable and wound is clean
- Secondary repair / tendon grafting: required if > 14 days have passed and tendon retraction/scarring have occurred; may need silicone rod spacer placement as a first stage
- Repairs in Zone 2 are hardest and most prone to adhesion formation; require early protected mobilization therapy post-op
A 2025 systematic review (PMID 41187290) confirms ultrasound and MRI are both useful for pre- and post-operative assessment of flexor tendon injuries.
Complications if Untreated or Poorly Managed
- Permanent loss of finger flexion
- Tendon retraction making repair impossible without grafting
- Tendon adhesions (commonest complication)
- Extensor lag or joint contracture
- In zone 1 avulsions: avascular necrosis of the tendon end
Key Takeaway
Any palmar-side laceration over a finger or hand that produces loss of active finger flexion = flexor tendon laceration until proven otherwise. The patient needs hand surgery referral urgently, proper splinting, antibiotics, and should not be reassured that the wound is "just a cut." Partial lacerations can look deceptively minor but still propagate or cause triggering.
- Roberts and Hedges' Clinical Procedures in Emergency Medicine
- Rosen's Emergency Medicine, Chapter 42
- Sabiston Textbook of Surgery, Chapter 119
- Campbell's Operative Orthopaedics, 15th Ed 2026
This is a shared conversation. Sign in to Orris to start your own chat.