Rediculopathy - LBP assessment , special test & management - 20 marks MPT level answer
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching PubMed
lumbar radiculopathy assessment management physiotherapy
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Loading Image
I now have comprehensive information to write a detailed MPT-level answer. Let me compile the full response.
Radiculopathy - Low Back Pain: Assessment, Special Tests & Management
(MPT Level - 20 Marks)
1. DEFINITION & PATHOPHYSIOLOGY
Radiculopathy refers to sensory or motor dysfunction caused by pathology of a spinal nerve root. In the lumbar spine, it is most commonly caused by intervertebral disc herniation, where the nucleus pulposus extrudes through a tear in the annulus fibrosus and compresses the exiting nerve root. Additional causes include lumbar spondylosis, osteophytic narrowing of the intervertebral foramina, lumbar spinal stenosis, spondylolisthesis, and rarely, neoplastic or infective processes.
L4-L5 and L5-S1 disc herniations account for approximately 90% of cases, making L5 and S1 the most commonly affected nerve roots. Lumbosacral radiculopathies are two to three times more common than cervical radiculopathies.
2. CLINICAL FEATURES
Symptoms
- Radicular pain: Sharp, burning, shooting pain radiating from the low back into the leg following the dermatomal distribution of the affected nerve root
- Paresthesias: Tingling, numbness, or pins-and-needles in a dermatomal distribution
- Motor weakness: Weakness in muscles innervated by the affected root
- Reflexes: Diminished or absent deep tendon reflexes at the corresponding level
- Symptoms aggravated by Valsalva maneuver (coughing, sneezing, straining)
Note: Due to dermatomal overlap, a clearly demarcated sensory loss from a single root lesion is unusual. Pinprick testing is more sensitive than light touch for detecting radicular sensory loss.
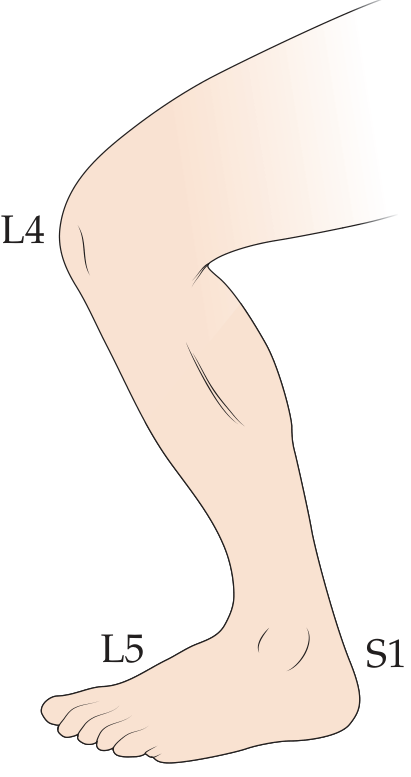
3. NERVE ROOT LEVEL CHART (L3 to S1)
| Disc Level | Root | Sensory Distribution | Reflex Affected | Key Motor Loss | Radiation Pattern | Screening Test |
|---|---|---|---|---|---|---|
| L3-L4 | L4 | Medial lower leg, medial foot, great toe (medial) | Patellar reflex | Knee extension (quadriceps), ankle dorsiflexion, inversion | Anterior thigh to anterior leg | Squat and rise |
| L4-L5 | L5 | Lateral lower leg, dorsum of foot, 1st web space | No reliable reflex | Hip abduction, knee flexion, great toe dorsiflexion (EHL), foot eversion | Buttock, lateral thigh/calf, dorsum of foot, great toe | Heel walking |
| L5-S1 | S1 | Posterior lower leg, lateral/plantar foot and ankle | Achilles reflex | Hip extension, knee flexion, plantar flexion | Posterior-lateral thigh, posterior leg, lateral/plantar foot | Toe walking |
(Rosen's Emergency Medicine; Neuroanatomy through Clinical Cases 3e)
4. ASSESSMENT
A. History Taking
- Pain history: Onset, duration, character (sharp/burning/shooting vs. dull aching), radiation pattern, aggravating and relieving factors
- Neurological symptoms: Paresthesias, numbness, weakness, bladder/bowel dysfunction
- Red flags screening:
- New urinary retention or saddle anesthesia → Cauda Equina Syndrome (emergency)
- History of cancer → metastatic disease
- Fever, significant trauma, age >70, corticosteroid use → fracture/infection
- Functional status: Activities of daily living, work capacity, gait disturbance
B. Observation & Postural Analysis
- Antalgic posture, scoliotic list
- Loss of lumbar lordosis
- Muscle wasting in thigh/calf (chronic cases)
C. Lumbar Range of Motion
- Flexion: Aggravates discogenic/radicular pain (increases intradiscal pressure)
- Extension: Aggravates facet joint pain; may relieve disc-related pain (McKenzie principle)
- Lateral flexion and rotation
D. Palpation
- Paraspinal muscle tenderness and spasm
- Spinous process percussion tenderness (suggests fracture/infection/metastasis)
- Facet joint tenderness on deep palpation
E. Neurological Examination
| Component | Method | Significance |
|---|---|---|
| Sensory | Pinprick (preferred over light touch) in dermatomal distribution | Identifies root level |
| Motor | Manual muscle testing (MMT) of myotomal key muscles | Identifies root level; grades 0-5 |
| Reflexes | Patellar (L4), Achilles (S1) | Absent/diminished = lower motor neuron lesion |
| Upper motor neuron | Babinski, clonus, hyperreflexia | Distinguishes myelopathy |
| Saddle sensation | Perianal/perineal sensation (S2-S5) | Cauda equina screening |
| Bladder | Post-void residual (>100 mL = denervated bladder) | Cauda equina screening |
| Gait | Heel walk (L5), toe walk (S1) | Quick myotomal screen |
F. Outcome Measures (MPT Relevant)
- Oswestry Disability Index (ODI) - gold standard for LBP functional disability
- Visual Analogue Scale (VAS) / Numeric Pain Rating Scale (NPRS)
- Roland-Morris Disability Questionnaire
- Fear-Avoidance Beliefs Questionnaire (FABQ) - psychosocial assessment
- Tampa Scale of Kinesiophobia
- Patient-Specific Functional Scale (PSFS)
5. SPECIAL TESTS
A. Tests for Nerve Root Tension (Dural Tension Signs)
1. Straight Leg Raise (SLR) / Lasegue's Test
- Position: Supine, legs fully extended
- Procedure: Examiner lifts the leg (hand under ankle, other hand maintains knee extension) passively, with the ankle in neutral or slight dorsiflexion
- Positive: Reproduction of the patient's typical radicular pain and paresthesias (not just posterior thigh tightness) at 30-70° of elevation
- Below 10° or above 70° is generally not caused by root compression
- Sensitivity: 72-97% | Specificity: 11-66%
- Positive predictive value: 67-89% in high-risk patients with sciatica
2. Crossed SLR (Well Leg SLR)
- Procedure: Elevating the asymptomatic leg produces typical radicular symptoms in the symptomatic leg
- Specificity: >90% for lumbosacral nerve root compression
- Highly specific - when positive, almost certainly indicates a disc herniation compressing a nerve root
3. Bragard's Test (Sensitization of SLR)
- At the point of SLR reproduction, ankle is dorsiflexed to add further neural tension
- Increases sensitivity of SLR
4. Slump Test
- Position: Patient sitting at the edge of the table
- Procedure: Sequential slumping (thoracic and lumbar flexion), then cervical flexion, then knee extension, then ankle dorsiflexion - each step added only if the previous is symptom-free
- Positive if symptoms reproduced, and relieved by cervical extension (differentiates neural from musculoskeletal)
- More sensitive than SLR for assessing neural tension in seated positions
5. Femoral Nerve Stretch Test (Prone Knee Bend)
- Indications: L2, L3, L4 radiculopathy
- Position: Prone
- Procedure: Hip extended with knee flexed to 90°; further hip extension is applied
- Positive: Reproduction of anterior thigh/groin pain
- Complements SLR for upper lumbar root testing
6. Bowstring Sign (Popliteal Pressure Test)
- During SLR, when pain is produced, the knee is slightly flexed to relieve it; then direct pressure is applied to the popliteal fossa (sciatic nerve)
- Positive: Reproduction of radicular pain confirms neural origin
B. Tests for Lumbar Instability / Segmental Dysfunction
7. Prone Instability Test
- Prone with legs dangling off table; examiner applies posterior-anterior pressure to a painful segment
- If pain decreases when the patient lifts legs (activating back extensors), segmental instability is suspected
8. Passive Lumbar Extension Test
- Examiner lifts both legs off table to approximately 30°
- Pain in low back = positive for lumbar instability
C. Tests for Facet Joint / Sacroiliac Involvement
9. Kemp's Test (Quadrant Test)
- Extension + ipsilateral lateral flexion + rotation = positive for facet joint pain or foraminal stenosis
10. Patrick Test (FABER)
- For sacroiliac joint or hip pathology
- Hip in Flexion, ABduction, External Rotation; positive if SI joint or groin pain reproduced
11. Gaenslen's Test
- Patient supine at edge of table; ipsilateral hip hyperextended while contralateral hip maximally flexed
- Positive for SI joint dysfunction
D. Non-Organic Signs (Waddell's Signs)
For identifying psychosocial components in LBP:
- Superficial/non-anatomic tenderness
- Simulation tests (axial loading, rotation)
- Distraction test (inconsistency between distracted and non-distracted SLR)
- Regional disturbances (non-dermatomal sensory/motor changes)
- Over-reaction
Three or more positive signs = significant non-organic component
6. INVESTIGATIONS
| Investigation | Purpose |
|---|---|
| MRI Lumbar Spine | Gold standard - disc herniation, nerve root compression, stenosis |
| CT Scan | Bony detail - osteophytes, foraminal stenosis, fracture |
| X-ray Lumbar | Alignment, spondylolisthesis, disc space narrowing |
| EMG/NCV | Confirms radiculopathy, differentiates from peripheral neuropathy; lower false-positive rate than MRI in asymptomatic patients |
| SPECT | Facet joint arthropathy (more specific than CT/MRI) |
| Vascular Doppler | Differentiates vascular claudication from neurogenic claudication |
7. MANAGEMENT
A. Physiotherapy Management (MPT Focus)
Phase 1 - Acute Phase (0-2 weeks)
Goals: Pain control, reduce neural sensitization, patient education
- Rest: Short-term (not exceeding 2 days); prolonged bed rest is counterproductive
- Pain relief modalities:
- TENS (Transcutaneous Electrical Nerve Stimulation)
- Interferential current therapy (IFT)
- Ultrasound therapy
- Hot/cold packs
- Positioning: Flexed lumbar posture for disc-related pain (side-lying with pillow between knees, or knee-chest position)
- Neural Mobilization (Neurodynamic Techniques):
- Gentle sciatic nerve sliders and tensioners
- Reduces neural mechanosensitivity and improves intraneural circulation
- Education: Posture advice, activity modification, ergonomics
Phase 2 - Subacute Phase (2-6 weeks)
Goals: Restore mobility, begin active rehabilitation
- McKenzie Method (Mechanical Diagnosis & Therapy):
- Centralization phenomenon: Exercises that shift peripheral pain centrally toward the spine are prognostically favorable
- Extension-based exercises for posterolateral disc herniations (most common)
- Flexion-based exercises for extension-related pain (facet/stenosis)
- Lumbar Stabilization Exercises (Core Stabilization):
- Transversus abdominis (TrA) activation - drawing-in maneuver
- Multifidus strengthening
- Dead bugs, bird dogs
- Progressed to dynamic stabilization
- Stretching: Hamstrings, hip flexors, piriformis (care with neural tension)
- Manual Therapy:
- Lumbar mobilization (Maitland Grade I-II initially; Grade III-IV as tolerated)
- Soft tissue techniques for paraspinal spasm
- Joint manipulation (if no red flags or instability)
Phase 3 - Chronic/Functional Phase (6 weeks+)
Goals: Full functional restoration, return to work/sport, prevention of recurrence
- Progressive strengthening: Open-chain and closed-chain exercises
- Aerobic conditioning: Walking, swimming, cycling (flexion posture on bike helpful for stenosis)
- Functional training and work hardening
- Aquatic therapy
B. Medical Management
| Category | Examples |
|---|---|
| Analgesics | Acetaminophen (paracetamol) |
| NSAIDs | Ibuprofen, naproxen, diclofenac - first-line anti-inflammatory |
| Muscle Relaxants | Cyclobenzaprine, methocarbamol - for muscle spasm |
| Neuropathic agents | Gabapentin, pregabalin - for radicular burning/lancinating pain |
| Oral corticosteroids | Short course for severe radiculopathy |
(Note: 2024 systematic review [PMID: 38629664] of clinical practice guidelines found NSAIDs, gabapentinoids, and short-course steroids are consistently recommended for lumbosacral radiculopathy)
C. Interventional Management
-
Lumbar Epidural Steroid Injection (LESI):
- Indicated for unremitting radiculopathy not responding to conservative care
- Provides significant short-term symptomatic relief
- Allows better participation in physiotherapy
- No proven long-term efficacy in controlled studies
-
Medial Branch Blocks / Facet Injections: For confirmed facet joint syndrome
-
Sacroiliac Joint Injection: For SI joint syndrome
-
Radiofrequency Ablation: For chronic facet or SI joint pain
-
Pulsed Radiofrequency of Dorsal Root Ganglion: Emerging evidence for refractory radicular pain (PMID: 40707353, 2026 systematic review)
D. Surgical Management
Indications:
- Absolute: Cauda equina syndrome (bowel/bladder dysfunction, saddle anesthesia) - surgical emergency
- Relative:
- Moderate to severe focal neurological deficit (weakness, significant sensory loss)
- Severe pain lasting >3 months not responding to aggressive conservative management with confirmed disc herniation on MRI
- Progressive neurological deficit
Procedures:
- Microdiscectomy / discectomy (L4-5 or L5-S1 herniation)
- Laminectomy (for spinal stenosis)
- Laminotomy with foraminotomy
- Spinal fusion (for instability/spondylolisthesis)
8. DIFFERENTIAL DIAGNOSIS
| Condition | Key Differentiating Feature |
|---|---|
| Lumbar disc herniation | SLR positive; MRI confirms; acute onset |
| Lumbar spinal stenosis | Neurogenic claudication; relieved by flexion; bilateral |
| Facet joint syndrome | Extension/rotation aggravates; SLR negative; no neural signs |
| Sacroiliac joint dysfunction | FABER/Gaenslen positive; no radiculopathy |
| Vascular claudication | Walking aggravates; absent distal pulses; Doppler positive |
| Piriformis syndrome | Tenderness at sciatic notch; FAIR test positive |
| Tumor/metastasis | Night pain; constitutional symptoms; unrelenting |
9. CAUDA EQUINA SYNDROME - RED FLAG EMERGENCY
Must be excluded in any LBP presentation:
- Bilateral leg weakness or numbness
- Saddle anesthesia (perianal/perineal)
- New urinary retention or overflow incontinence (PVR >100 mL)
- Fecal incontinence
Immediate MRI and surgical referral are indicated.
10. PROGNOSIS
- The majority of patients (60-90%) with lumbar radiculopathy improve significantly with conservative management within 6-12 weeks
- Centralization of pain (McKenzie) during assessment is a favorable prognostic indicator
- Patients with scoliosis and radiculopathy tend to have worse conservative outcomes
- Surgical outcomes for microdiscectomy are excellent for radicular leg pain, though back pain may persist
Key References:
- Neuroanatomy through Clinical Cases, 3rd ed. - Blumenfeld (KCC 8.3)
- Rosen's Emergency Medicine, 10e - Table 31.2 (Nerve root levels)
- Bradley and Daroff's Neurology in Clinical Practice - Low Back Pain chapter
- Adams and Victor's Principles of Neurology, 12e - Lumbar Stenosis/Radiculopathy
- Campbell's Operative Orthopaedics, 15e (2026) - Nonoperative Treatment
- Price MR et al. (2024) PM&R [PMID: 38629664] - Medication guidelines for lumbosacral radiculopathy
- Park JH et al. (2026) Reg Anesth Pain Med [PMID: 40707353] - Interventional options for radicular pain
This is a shared conversation. Sign in to Orris to start your own chat.