Tell me about all the nerves there tests with images
Asking for Preferences
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Searching Images
Tinel sign Phalen test carpal tunnel median nerve
Searching Images
Froment sign ulnar nerve test hand
Searching Images
elbow flexion test cubital tunnel ulnar nerve
Searching Images
wrist drop radial nerve palsy Saturday night palsy
I now have everything I need to write a comprehensive, well-illustrated answer. Let me compile it.
Peripheral Nerve Injury Tests — Complete Guide
🖐️ MEDIAN NERVE TESTS
1. Tinel's Sign
Indication: Carpal tunnel syndrome (CTS) — and any median nerve compression
Technique: Gently tap (percuss) with two fingers over the carpal tunnel on the volar (palmar) surface of the wrist
Positive finding: Electric shock-like tingling shooting into the thumb, index, middle, and radial half of the ring finger
Mechanism: Percussion mechanically stimulates the irritated or regenerating median nerve fibers
Technique: Gently tap (percuss) with two fingers over the carpal tunnel on the volar (palmar) surface of the wrist
Positive finding: Electric shock-like tingling shooting into the thumb, index, middle, and radial half of the ring finger
Mechanism: Percussion mechanically stimulates the irritated or regenerating median nerve fibers

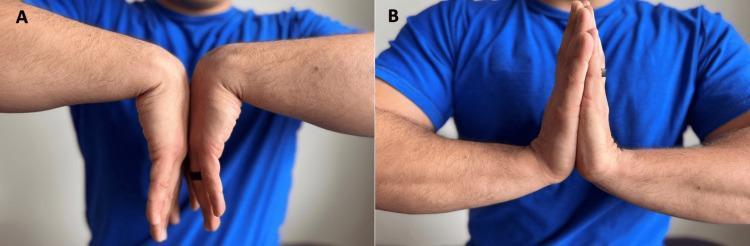
2. Phalen's Test (Phalen's Maneuver)
Indication: Carpal tunnel syndrome
Technique: Patient holds both wrists in maximal flexion (dorsal hands pressed together, fingers pointing down) for 60 seconds. This constricts the transverse carpal ligament and narrows the tunnel.
Positive finding: Reproduction of numbness, tingling, or pain in the median nerve distribution within 30–60 seconds
Technique: Patient holds both wrists in maximal flexion (dorsal hands pressed together, fingers pointing down) for 60 seconds. This constricts the transverse carpal ligament and narrows the tunnel.
Positive finding: Reproduction of numbness, tingling, or pain in the median nerve distribution within 30–60 seconds
3. Durkan Compression Test (Carpal Tunnel Compression Test)
Indication: Carpal tunnel syndrome — most sensitive provocative test for CTS
Technique: Examiner compresses the median nerve directly over the carpal tunnel (thumb on the palm, wrist in neutral) for up to 30–60 seconds
Positive finding: Reproduction of numbness, tingling, or pain in the median nerve distribution
Technique: Examiner compresses the median nerve directly over the carpal tunnel (thumb on the palm, wrist in neutral) for up to 30–60 seconds
Positive finding: Reproduction of numbness, tingling, or pain in the median nerve distribution
"Most sensitive provocative test: carpal tunnel compression test (Durkan test) with wrist in neutral position" — Miller's Review of Orthopaedics, 9th Ed.
4. "OK Sign" / Anterior Interosseous Nerve Test
Indication: Anterior interosseous nerve (AIN) entrapment (purely motor branch of median nerve)
Technique: Ask the patient to form a circle (the "OK sign") with the thumb and index finger
Positive finding: Inability to flex the thumb IP joint and index DIP simultaneously → the patient instead forms a "pinch" posture (precision sign); no sensory loss
Technique: Ask the patient to form a circle (the "OK sign") with the thumb and index finger
Positive finding: Inability to flex the thumb IP joint and index DIP simultaneously → the patient instead forms a "pinch" posture (precision sign); no sensory loss
5. Abductor Pollicis Brevis (APB) Test
Indication: Median nerve motor branch integrity at the wrist (thenar branch)
Technique: Place thumb in palmar abduction (palm up); patient resists force directed toward the palm. Palpate the APB belly to confirm contraction.
Positive finding: Weakness of thumb opposition/abduction = motor branch compromise
Technique: Place thumb in palmar abduction (palm up); patient resists force directed toward the palm. Palpate the APB belly to confirm contraction.
Positive finding: Weakness of thumb opposition/abduction = motor branch compromise
"The best muscle to test in suspected carpal tunnel syndrome is the abductor pollicis brevis, which abducts the thumb perpendicular to the plane of the palm." — Neuroanatomy Through Clinical Cases, 3rd Ed.
✋ ULNAR NERVE TESTS
6. Tinel's Sign at the Elbow
Indication: Cubital tunnel syndrome (ulnar nerve at medial epicondyle)
Technique: Tap over the cubital tunnel at the medial epicondyle
Positive finding: Pain or paresthesias shooting down the ulnar border of the forearm into the 4th and 5th fingers
Technique: Tap over the cubital tunnel at the medial epicondyle
Positive finding: Pain or paresthesias shooting down the ulnar border of the forearm into the 4th and 5th fingers
7. Elbow Flexion Test
Indication: Cubital tunnel syndrome
Technique: Hyperflexion of the elbow with shoulder flexed at 90°; maintain for 3 minutes. Elbow flexion tightens the cubital tunnel retinaculum and stretches the ulnar nerve.
Positive finding: Reproduction of pain, numbness, or tingling in the ulnar nerve distribution (5th and medial 4th finger)
Technique: Hyperflexion of the elbow with shoulder flexed at 90°; maintain for 3 minutes. Elbow flexion tightens the cubital tunnel retinaculum and stretches the ulnar nerve.
Positive finding: Reproduction of pain, numbness, or tingling in the ulnar nerve distribution (5th and medial 4th finger)
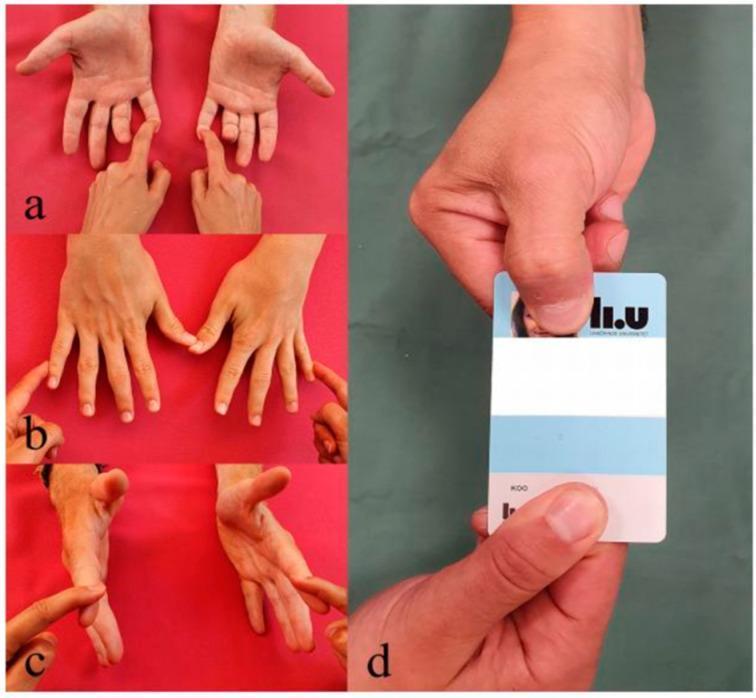
8. Froment's Sign
Indication: Ulnar nerve palsy (specifically tests adductor pollicis, which is ulnar-innervated)
Technique: Ask the patient to hold a piece of paper in a lateral (key) pinch between thumb and radial side of the index finger. Attempt to pull the paper away.
Positive finding: Patient flexes the thumb at the IP joint (using flexor pollicis longus, median-innervated) to compensate for a paralyzed adductor pollicis. IP flexion = positive Froment's sign.
Technique: Ask the patient to hold a piece of paper in a lateral (key) pinch between thumb and radial side of the index finger. Attempt to pull the paper away.
Positive finding: Patient flexes the thumb at the IP joint (using flexor pollicis longus, median-innervated) to compensate for a paralyzed adductor pollicis. IP flexion = positive Froment's sign.
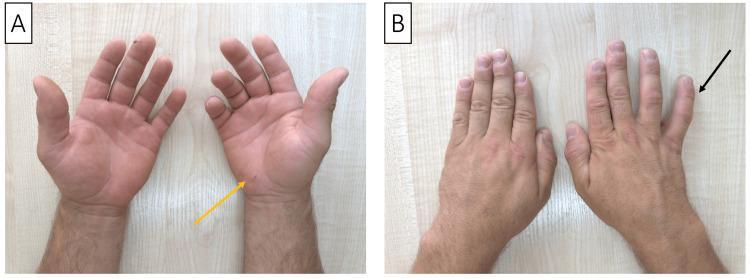
9. Wartenberg's Sign
Indication: Ulnar neuropathy
Technique: Observe the patient's small (5th) finger at rest
Positive finding: Persistent abduction/extension of the small finger during attempted adduction — due to weakness of the 3rd palmar interosseous (ulnar) and unopposed pull of the extensor digiti quinti (radial nerve)
Technique: Observe the patient's small (5th) finger at rest
Positive finding: Persistent abduction/extension of the small finger during attempted adduction — due to weakness of the 3rd palmar interosseous (ulnar) and unopposed pull of the extensor digiti quinti (radial nerve)
10. Jeanne's Sign
Indication: Ulnar neuropathy
Technique: Observe thumb posture during key pinch
Positive finding: Thumb MCP hyperextension during key pinch — due to weak adductor pollicis (ulnar-innervated). Often accompanies Froment's sign.
Technique: Observe thumb posture during key pinch
Positive finding: Thumb MCP hyperextension during key pinch — due to weak adductor pollicis (ulnar-innervated). Often accompanies Froment's sign.
"Froment: thumb IP flexion during key pinch. Jeanne: thumb MCP hyperextension during key pinch. Wartenberg: abduction/extension of small digit during attempted adduction." — Miller's Review of Orthopaedics, 9th Ed.
11. Finger Abduction/Spread Test
Indication: Ulnar intrinsic weakness
Technique: Ask patient to spread fingers apart or cross middle over index finger; resist force pushing them to midline
Positive finding: Weakness confirms ulnar nerve motor branch deficit at or above the wrist level
Technique: Ask patient to spread fingers apart or cross middle over index finger; resist force pushing them to midline
Positive finding: Weakness confirms ulnar nerve motor branch deficit at or above the wrist level
🦾 RADIAL NERVE TESTS
12. Wrist/Finger Extension Test
Indication: Radial nerve palsy or posterior interosseous nerve (PIN) injury
Technique: Place patient's palm flat on a table; ask them to lift each finger straight up (hyperextend MCP joints) against resistance
Positive finding: Inability to hyperextend the finger MCP joints = radial nerve or PIN injury. If the patient can weakly extend the wrist in a radial direction (ECRL/ECRB spared) but not extend fingers → PIN palsy (radial nerve proper is intact)
Classic sign: "Wrist drop" — inability to extend the wrist against gravity
Technique: Place patient's palm flat on a table; ask them to lift each finger straight up (hyperextend MCP joints) against resistance
Positive finding: Inability to hyperextend the finger MCP joints = radial nerve or PIN injury. If the patient can weakly extend the wrist in a radial direction (ECRL/ECRB spared) but not extend fingers → PIN palsy (radial nerve proper is intact)
Classic sign: "Wrist drop" — inability to extend the wrist against gravity

13. Extensor Pollicis Longus (EPL) Test
Indication: Radial nerve / PIN integrity
Technique: Ask patient to extend the thumb against resistance
Positive finding: Weakness or absence = PIN injury (EPL is innervated by the posterior interosseous nerve)
Technique: Ask patient to extend the thumb against resistance
Positive finding: Weakness or absence = PIN injury (EPL is innervated by the posterior interosseous nerve)
MEDIAN NERVE — Proximal Tests
14. Pronator Syndrome Provocative Tests
Indication: Median nerve compression in the proximal forearm (pronator teres level)
Three separate maneuvers isolate the compression site:
Three separate maneuvers isolate the compression site:
| Maneuver | Compression site |
|---|---|
| Resisted elbow flexion with forearm supinated | Bicipital aponeurosis (lacertus fibrosis) |
| Resisted forearm pronation with elbow extended | Between heads of pronator teres |
| Resisted long finger PIP flexion | FDS arch |
Key differentiator from CTS: Pronator syndrome causes sensory disturbances over the thenar eminence (palmar cutaneous branch, exits proximal to carpal tunnel); CTS spares thenar sensation.
🦿 THORACIC OUTLET / LOWER LIMB NERVES
15. Adson Test
Indication: Thoracic outlet syndrome (vascular — subclavian vein/artery compression)
Technique: Patient hyperextends the neck and rotates it to the affected side; decreased radial pulse during inhalation
Positive finding: Diminished or absent radial pulse = positive
Technique: Patient hyperextends the neck and rotates it to the affected side; decreased radial pulse during inhalation
Positive finding: Diminished or absent radial pulse = positive
16. Peroneal Nerve Assessment
Indication: Deep peroneal nerve entrapment (fibular head, anterior tarsal tunnel)
Clinical sign: Foot drop (inability to dorsiflex the foot) + numbness in the web space between the 1st and 2nd toes
Causes: Proximal fibular fracture, habitual leg crossing, prolonged squatting
Clinical sign: Foot drop (inability to dorsiflex the foot) + numbness in the web space between the 1st and 2nd toes
Causes: Proximal fibular fracture, habitual leg crossing, prolonged squatting
Summary Table
| Test | Nerve | Site Tested | Positive Finding |
|---|---|---|---|
| Tinel's sign (wrist) | Median | Carpal tunnel | Tingling in digits 1–3.5 |
| Phalen's test | Median | Carpal tunnel | Tingling in digits 1–3.5 after 60 s wrist flexion |
| Durkan compression test | Median | Carpal tunnel | Tingling in digits 1–3.5 (most sensitive) |
| "OK sign" / AIN test | Median (AIN) | Forearm | Can't form circle — motor loss, no sensory loss |
| Tinel's sign (elbow) | Ulnar | Cubital tunnel | Tingling in digits 4–5 |
| Elbow flexion test | Ulnar | Cubital tunnel | Tingling in digits 4–5 within 3 min |
| Froment's sign | Ulnar | Adductor pollicis | Thumb IP flexion during key pinch |
| Wartenberg's sign | Ulnar | 3rd palmar interosseous | Small finger abduction at rest |
| Jeanne's sign | Ulnar | Adductor pollicis | Thumb MCP hyperextension during key pinch |
| Wrist drop / MCP extension | Radial | Spiral groove / PIN | No wrist/finger extension |
| Adson test | Brachial plexus | Thoracic outlet | Reduced radial pulse |
| Foot drop exam | Deep peroneal | Fibular head | Cannot dorsiflex foot |
Sources:
- Sabiston Textbook of Surgery, 21st Ed. — Table 119.3
- Miller's Review of Orthopaedics, 9th Ed. — Tables 7.8 and Compression Neuropathy section
- Tintinalli's Emergency Medicine, 9th Ed. — Focal Mononeuropathies chapter
- Neuroanatomy Through Clinical Cases, 3rd Ed. — Upper Extremity Nerve Injuries
- Thieme Atlas of Anatomy — General Anatomy and Musculoskeletal System
Scorpion bite black Indian variant management
Checking Date & Time
Reading File
Finding Sources
Finding Sources
Searching PubMed
scorpion envenomation India management prazosin
Reading File
Reading File
Finding Sources
Searching PubMed
"scorpion sting" AND India
Reading File
Reading File
Reading File
Reading Article
PMID: 36505581
Reading File
Finding Sources
Searching the Web
Indian black scorpion Heterometrus Palamneus sting management treatment
Searching Images
Indian scorpion envenomation pulmonary edema catecholamine storm prazosin treatment
I now have comprehensive data from multiple authoritative sources. Let me compile the full answer.
Indian Black Scorpion (Heterometrus spp. / Palamneus spp.) — Management
Species Clarification: Red vs. Black
India has two medically important scorpion groups, which must be distinguished since their toxidromes and management differ significantly:
| Feature | Indian Red Scorpion (Hottentotta tamulus, formerly Mesobuthus tamulus) | Indian Black Scorpion (Heterometrus spp. / Palamneus spp.) |
|---|---|---|
| Family | Buthidae | Scorpionidae |
| Color | Red-orange/brown | Glossy black, large body |
| Toxin type | Neurotoxins + massive catecholamine storm | Primarily cytotoxic, milder systemic toxicity |
| Distribution | Maharashtra, Gujarat, Karnataka, Tamil Nadu | Northeast India, Kerala, Eastern states |
| Mortality | High (especially children) | Low — rarely life-threatening |
| Key danger | Acute pulmonary edema, cardiogenic shock | Local pain, swelling; mild systemic effects |
The Indian black scorpion (Heterometrus bengalensis, H. swammerdami, Palamneus gravimanus) belongs to Scorpionidae — NOT Buthidae. Its venom is predominantly cytotoxic/local rather than neurotoxic, and it rarely causes the catecholamine storm that makes red scorpion envenomation so dangerous. — [Indian Black Scorpion Venom Action, Avens Online]
🦂 Pathophysiology of Black Scorpion Venom
- Venom contains cytotoxic proteins, phospholipases, hyaluronidases, and weak sodium channel toxins
- Causes local tissue damage, pain, and edema — systemic toxicity is uncommon
- Rarely triggers cardiovascular effects (contrast with Buthidae)
- Large volume of venom can be injected due to larger body size, occasionally causing more severe local reactions
Clinical Features
Grade 1 (Local only — most common)
- Immediate sharp pain at sting site
- Local erythema, edema, tenderness
- Paresthesias spreading proximally
- No systemic features
Grade 2 (Mild systemic)
- Profuse sweating, nausea, vomiting
- Mild tachycardia
- Anxiety, restlessness
- No hemodynamic compromise
Grade 3 (Severe — rare with black scorpion)
- Significant cardiovascular or neurological involvement
- Pulmonary edema (rare but documented)
- Severe autonomic disturbance
Local and systemic symptoms are typically out of proportion to cutaneous signs — erythema and edema at the sting site are not usually prominent. — Fitzpatrick's Dermatology, 9th Ed.
(The above — VT + pulmonary edema — represents Buthidae envenomation. Black scorpion stings rarely cause this degree of cardiovascular toxicity.)
Management
Immediate / Prehospital
- Calm the patient — anxiety worsens symptoms; reassure that black scorpion stings are rarely fatal
- Identify the scorpion if possible — this determines the treatment pathway
- Do NOT apply tourniquets, incise the wound, or apply electric shock (no evidence of benefit)
- Apply a cold pack / ice pack to the sting site — reduces local pain and venom absorption
- Immobilize the affected limb
- Transport to hospital in all children and any patient with systemic features
Emergency Department Management
Step 1 — Assess grade of envenomation
- Full vital signs, ECG, pulse oximetry
- Neuro exam (cranial nerve function, muscle activity)
- Labs if systemic features: CBC, RFT, LFT, serum electrolytes, troponin, CXR
Step 2 — Pain Control (Grade 1 and all patients)
| Agent | Dose | Route |
|---|---|---|
| Paracetamol | 10–15 mg/kg (child); 500–1000 mg (adult) | Oral/IV |
| NSAIDs (ibuprofen, ketorolac) | Standard doses | Oral/IV |
| Local infiltration of lidocaine (without epinephrine) | 1–2 mL of 1–2% | At sting site |
| Opioids (fentanyl/morphine) | For severe pain | IV |
Acetaminophen, NSAIDs, and local lidocaine (without epinephrine) at the sting site are first-line for local pain. Opioid analgesia may be necessary for more severe symptoms. — Tintinalli's Emergency Medicine, 9th Ed.
Step 3 — Sedation for Agitation / Neuromuscular Hyperactivity
- Benzodiazepines (midazolam, diazepam) for anxiety, muscle hyperactivity, restlessness
- Continuous IV midazolam infusion reduces agitation and involuntary movements
"A continuous IV infusion of midazolam reduces the agitation and involuntary movements produced by scorpion stings." — Harrison's Principles of Internal Medicine, 22nd Ed.
Step 4 — Cardiovascular Management (if systemic features develop)
| Condition | Drug | Notes |
|---|---|---|
| Hypertension + tachycardia (catecholamine excess) | Prazosin (α1-blocker) | Key drug in India — 250–500 mcg (child) or 500 mcg–1 mg (adult) sublingual/oral, can repeat 3-hourly |
| Pulmonary edema | Prazosin + nitroglycerin or nitroprusside | Reduces preload/afterload |
| Cardiogenic shock | Dobutamine | Inotropic support |
| Bradycardia + cholinergic symptoms (Tityus/Parabuthus pattern — rare in India) | Atropine | Only if vagal-dominant picture |
"Prazosin reverses the autonomic storm characteristic of Indian red scorpion (Hottentotta tamulus) envenomation, resulting in accelerated recovery and preserved myocardial function." — Fitzpatrick's Dermatology, 9th Ed.
"Prazosin has been effective, especially in addition to antivenom, for treatment of catecholamine excess and cardiovascular compromise in Mesobuthus tamulus stings." — Rosen's Emergency Medicine, 9th Ed.
Note: For the black scorpion (Heterometrus), cardiovascular crisis is uncommon — but prazosin should be used if hypertension or pulmonary edema appears.
Step 5 — Antivenom
- Indian polyvalent scorpion antivenom (CSL Ltd / Central Research Institute, Kasauli) is available in India
- Produced against Hottentotta tamulus (red scorpion) — its efficacy against Heterometrus (black scorpion) is limited
- Antivenom is not routinely indicated for black scorpion envenomation
- Indicated when: severe systemic features, cardiovascular instability, neuromuscular dysfunction
- If administered: IV, diluted in NS, given slowly with resuscitation available
- Risk of anaphylaxis and serum sickness (equine-derived)
"Antivenin is available in endemic areas and, along with supportive care, has been shown to reduce morbidity and mortality from severe scorpion envenomation." — Fitzpatrick's Dermatology, 9th Ed.
"Role of antivenom not clear once systemic toxicity established, as antivenom binds toxin but does not reverse established injury." — Tintinalli's Emergency Medicine, 9th Ed.
Supportive Care
- Airway management if hypersalivation + cranial nerve dysfunction compromise airway (more relevant in red scorpion)
- IV fluids for hemodynamic support — cautiously (pulmonary edema risk)
- Tetanus prophylaxis if not up-to-date
- Antihistamines for local allergic component
- Monitor for secondary complications: rhabdomyolysis, pancreatitis, renal failure (rare with black scorpion)
Disposition
| Grade | Disposition |
|---|---|
| Grade 1 (local only) | Observe 2–4 hours; discharge with analgesia and return precautions |
| Grade 2 (mild systemic) | Admit for 12–24 hours monitoring, prazosin if needed |
| Grade 3 (severe) | ICU admission, consider antivenom, intensive monitoring |
| All children | Admit for at least 12–24 hours (children have more severe course) |
Quick Summary: Black Scorpion vs. Red Scorpion Management Differences
| Aspect | Black Scorpion (Heterometrus) | Red Scorpion (Hottentotta tamulus) |
|---|---|---|
| Prazosin | Only if cardiovascular features | Cornerstone drug — use early |
| Antivenom | Rarely needed; limited species-specific efficacy | Indicated for systemic toxicity |
| ICU | Rarely needed | Frequently needed in children |
| Mortality | Very low | Significant (especially children <10 yrs) |
| Main concern | Local pain, rarely systemic | Pulmonary edema, cardiogenic shock |
Sources:
- Harrison's Principles of Internal Medicine, 22nd Ed. — Scorpion Stings
- Rosen's Emergency Medicine, 9th Ed. — Scorpions chapter
- Tintinalli's Emergency Medicine, 9th Ed. — Table 211-2
- Fitzpatrick's Dermatology, 9th Ed. — Selected Scorpion Species
- Kumar R. An update on epidemiology and management of scorpion envenomation in India. J Fam Med Prim Care 2022 [PMID: 36505581]
Oseltamivir in feeding mothers
Checking Date & Time
Your credits are exhausted. Your daily credits reset tomorrow, or you can purchase a top-up for more.
This is a shared conversation. Sign in to Orris to start your own chat.