Calcification.
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
Finding Sources
The psammoma body image is just a placeholder graphic (concentric rings icon). I have all the core content needed. Now I'll compile the comprehensive answer.
Pathologic Calcification
Pathologic calcification is the abnormal tissue deposition of calcium salts (primarily calcium phosphate/hydroxyapatite), together with smaller amounts of iron, magnesium, and other mineral salts. There are two major forms - dystrophic and metastatic - plus a third special category of ectopic ossification.
- Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 76
1. Dystrophic Calcification
Definition: Deposition of calcium in necrotic or dying tissue, occurring despite normal serum calcium levels and no systemic disturbance of calcium metabolism.
Sites
- Areas of coagulative, caseous, or liquefactive necrosis
- Enzymatic fat necrosis (e.g., pancreatitis)
- Atheromatous plaques of advanced atherosclerosis (almost invariably present)
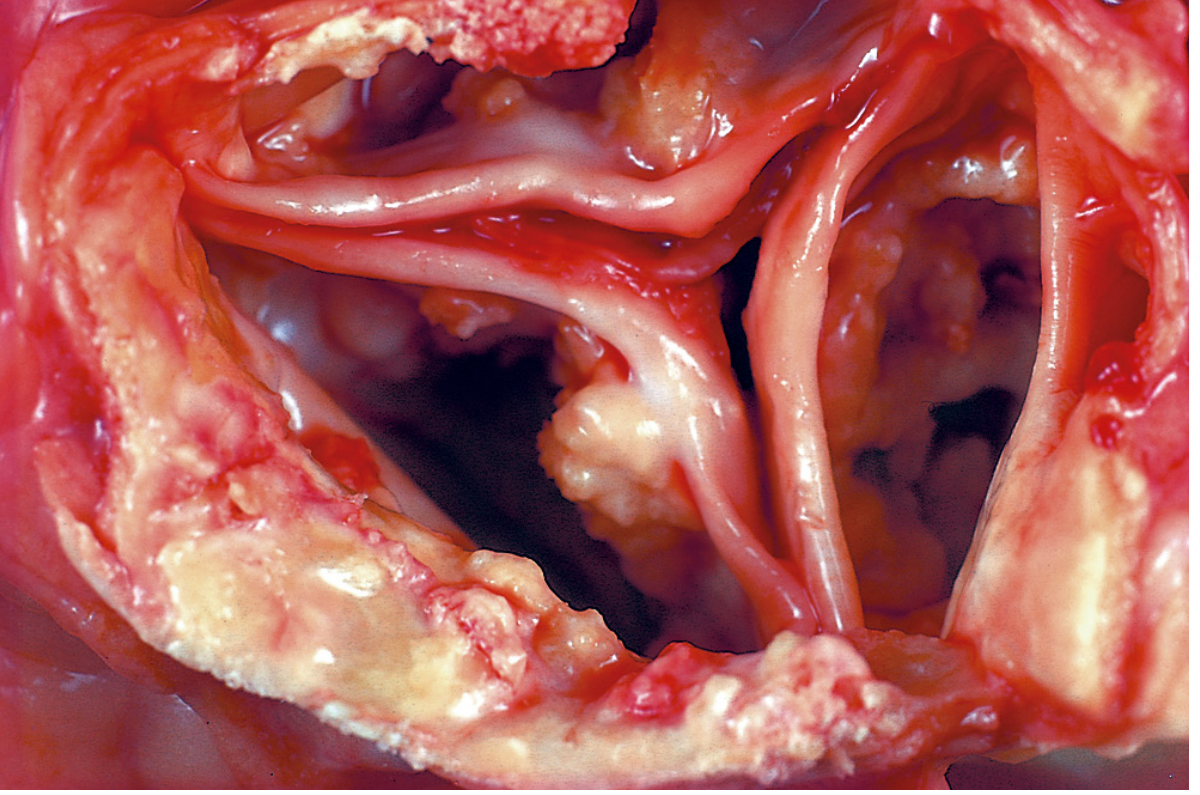
- Aging or damaged heart valves (e.g., calcific aortic stenosis - see image below)
- Tuberculous lymph nodes (may be virtually converted to stone)
Morphology (Histology)
- On H&E stain: basophilic, amorphous granular (sometimes clumped) deposits
- Can be intracellular, extracellular, or both
- Psammoma bodies: Lamellated (concentric ring) configurations formed when single necrotic cells act as seed crystals that become progressively encrusted. Named for resemblance to grains of sand (psammos = sand). Seen in:
- Papillary thyroid carcinoma
- Meningioma
- Papillary serous ovarian carcinoma
- Asbestos bodies: In asbestosis, calcium and iron salts gather around long slender asbestos spicules in the lung, creating beaded dumbbell forms
- Heterotopic bone may eventually form at the focus of calcification
- Serum calcium is normal
Clinical significance
- May simply mark previous injury - or may cause significant organ dysfunction:
- Calcific valvular disease (aortic stenosis)
- Atherosclerotic plaque instability/stenosis
2. Metastatic Calcification
Definition: Deposition of calcium salts in otherwise normal tissues, almost always due to hypercalcemia from systemic calcium/phosphate metabolic disturbance.
Four Principal Causes of Hypercalcemia (Robbins)
- Increased PTH secretion - primary hyperparathyroidism (parathyroid tumors), or ectopic PTH-related protein (PTHrP) secretion by malignant tumors
- Bone resorption - multiple myeloma, diffuse skeletal metastases (e.g., breast cancer), Paget disease, immobilization
- Vitamin D-related disorders - vitamin D intoxication; sarcoidosis (macrophages activate vitamin D precursor); Williams syndrome (idiopathic hypercalcemia of infancy)
- Renal failure - phosphate retention leads to secondary hyperparathyroidism; also aluminum intoxication (chronic dialysis), milk-alkali syndrome (excessive calcium + absorbable antacids)
Sites Predominantly Affected
Tissues that excrete acid have an internal alkaline compartment that predisposes them:
- Gastric mucosa (parietal cells pump H⁺ → alkaline interstitium)
- Kidneys (nephrocalcinosis)
- Lungs (may cause respiratory compromise)
- Systemic arteries and pulmonary veins
Key rule from Harrison's: Calcifications in hypercalcemic states with normal or low phosphate preferentially affect kidney, lungs, and gastric mucosa. Hyperphosphatemia with normal/low calcium preferentially affects kidney and arteries.
Calcium-phosphate precipitation is especially likely when serum Ca × PO₄ concentration product >75.
Morphology
- Morphologically similar to dystrophic calcification - amorphous noncrystalline deposits or hydroxyapatite crystals
- Usually causes no clinical dysfunction, but massive pulmonary involvement can cause respiratory compromise; massive renal deposits (nephrocalcinosis) can cause renal damage
3. Mixed Calcification
A combination of metastatic and dystrophic mechanisms. Calcium dysregulation initiates the process (metastatic component), and trauma then propagates it (dystrophic component). Seen in disorders like dermatomyositis.
- Dermatology 2-Volume Set 5e
4. Ectopic Ossification / Tumoral Calcinosis
A third mechanism described in Harrison's: true bone formation in soft tissues (as opposed to calcium salt deposition). Examples:
- Myositis ossificans - heterotopic bone in muscle after trauma
- Fibrodysplasia ossificans progressiva (FOP) - rare genetic disorder
- Tumoral calcinosis - rare, caused by FGF23/GALNT3/α-Klotho gene mutations → reduced FGF23 activity → increased renal phosphate reabsorption → hyperphosphatemia → periarticular calcium phosphate masses (shoulders, hips, ankles). Labs show elevated serum phosphate and 1,25-(OH)₂ vitamin D; PTH and calcium are normal.
Summary Table
| Feature | Dystrophic | Metastatic |
|---|---|---|
| Site | Necrotic/injured tissue | Normal tissue |
| Serum calcium | Normal | Elevated (usually) |
| Serum phosphate | Normal | Often elevated |
| Mechanism | Local cell death → phosphatase release → nucleation | Systemic hypercalcemia/hyperphosphatemia |
| Examples | Atherosclerosis, calcific aortic stenosis, TB node, fat necrosis | Hyperparathyroidism, renal failure, sarcoidosis, vitamin D toxicity |
| Preferred sites | Anywhere necrosis occurs | Gastric mucosa, lungs, kidneys, arteries |
| Clinical significance | May cause valve dysfunction, atherosclerosis | Usually asymptomatic; nephrocalcinosis, pulmonary calcification if severe |
Sources:
- Robbins, Cotran & Kumar Pathologic Basis of Disease, pp. 76-77 (Pathologic Calcification)
- Harrison's Principles of Internal Medicine, 22E (2025), p. 3362 (Extraskeletal Calcification and Ossification)
- Dermatology 2-Volume Set 5e (Mixed Calcification)
This is a shared conversation. Sign in to Orris to start your own chat.