Lepra reaction
Reading File
Finding Sources
Finding Sources
Searching PubMed
"leprosy reactions" AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information from multiple authoritative sources. Let me compile a thorough, well-organized response.
Lepra Reaction
Lepra reactions are immunologically mediated episodes of acute or subacute inflammation that occur during the course of leprosy. They are distinct from the underlying infection itself and represent a sudden change in the immune balance between the host and Mycobacterium leprae. Because peripheral nerve trunks are often involved, prompt treatment is essential to prevent permanent deformity.
Pathogenesis
The key trigger is an abrupt alteration of immune response - either following multi-drug therapy (MDT) or spontaneous improvement in immunological status - which causes acute inflammation of skin, nerves, and other tissues.
-
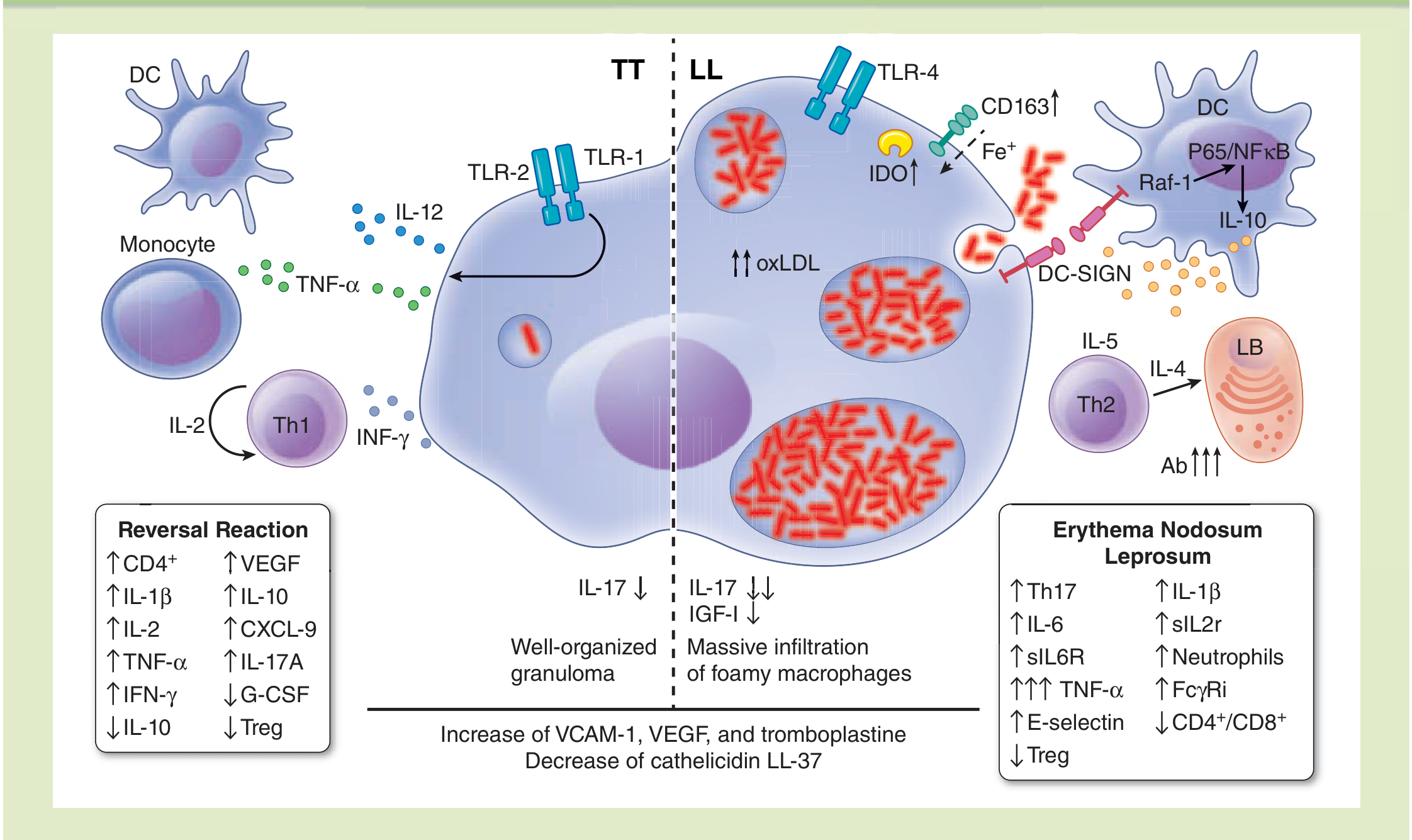
Type 1 / Reversal Reaction: Caused by a sudden increase in cell-mediated immunity (CMI) against M. leprae. It is a Type IV (delayed-type) hypersensitivity reaction. There is upregulation of CD4+ T cells, IL-1β, IL-2, TNF-α, IFN-γ, VEGF, CXCL-9, IL-17A, with downregulation of IL-10 and Treg subsets.
-
Type 2 / ENL: An immune-complex mediated (Type III) hypersensitivity reaction. It involves anti-PGL-I and anti-monocyte chemoattractant protein antibodies, upregulation of Th17, IL-6, IL-1β, TNF-α (markedly elevated), E-selectin, FcγRI, and neutrophil influx into lesions. Treg response is decreased.
Types of Lepra Reactions
Type 1 - Reversal Reaction (RR)
| Feature | Details |
|---|---|
| Leprosy type | Borderline-tuberculoid (BT), Borderline-borderline (BB), and lepromatous leprosy |
| Mechanism | Type IV hypersensitivity - CMI upregulation |
| Skin | Existing leprosy lesions become acutely inflamed - red, swollen, and raised |
| Nerves | Acute neuritis with rapid loss of nerve function; this is the primary danger |
| Systemic symptoms | Minimal to absent |
| Timing | Before, during, or after MDT |
| Onset | Can appear at any time during treatment; related to shift toward tuberculoid end of spectrum |
- New granuloma formation occurs with increased release of TNF-α, IFN-γ, and IL-2
- The exacerbation of rash, neuropathy, and new lesions is characteristic
- Urgency: Must be diagnosed and treated as soon as possible to prevent permanent nerve damage
Type 2 - Erythema Nodosum Leprosum (ENL)
| Feature | Details |
|---|---|
| Leprosy type | Lepromatous leprosy (LL) and Borderline-lepromatous (BL) |
| Mechanism | Type III hypersensitivity - immune complex deposition |
| Skin | New erythematous, tender subcutaneous nodules (1-2 cm) on limbs and trunk; original patches unchanged |
| Nerves | Neuritis (acute/subacute) |
| Systemic | Fever, malaise, edema - prominent |
| Extracutaneous | Panniculitis, glomerulonephritis, arthralgia, epididymitis/orchitis, eye inflammation (iritis, iridocyclitis), osteitis, lymphadenitis |
| Bacillary load | High bacillary index - important risk factor |
| Recurrence | 65% of cases have more than one episode |
Lucio Phenomenon (Type 3 / Rare)
A rare but severe form, seen in diffuse lepromatous leprosy. Characterized by bluish/violaceous hemorrhagic plaques followed by large recurrent ulcerations predominantly in the lower extremities. It represents severe cutaneous necrotizing vasculitis and can be fatal.

Distinguishing Type 1 vs Type 2 Reactions
| Feature | Type 1 (Reversal) | Type 2 (ENL) |
|---|---|---|
| Leprosy subtype | BT, BB, BL, LL | LL, BL |
| Skin change | Existing lesions inflame (red, swollen) | New red nodules appear; old patches unchanged |
| Systemic symptoms | Absent/mild | Fever, malaise, edema - prominent |
| Neuritis | Common, rapidly progressive | Can occur |
| Extracutaneous | Mainly neuritis | Multisystem: joints, kidneys, eyes, testes, lymph nodes |
| Mechanism | Type IV (CMI) | Type III (immune complex) |
| Predominant cells | CD4+ T cells | Neutrophils, Th17 |
Timing of Reactions
Both Type 1 and Type 2 reactions can occur:
- Before the start of MDT
- During MDT treatment
- After completion of treatment
Treatment
General Principle
Do NOT stop MDT if a reaction occurs during treatment. Continue and complete the full course. For reactions after treatment completion, MDT should not be restarted.
Type 1 (Reversal Reaction)
- Drug of choice: Prednisolone (1-2 mg/kg/day with slow taper over ~3 months)
- Standard WHO 12-week regimen:
| Week | Prednisolone Dose |
|---|---|
| 1-2 | 40 mg/day |
| 3-4 | 30 mg/day |
| 5-6 | 20 mg/day |
| 7-8 | 15 mg/day |
| 9-10 | 10 mg/day |
| 11-12 | 5 mg/day |
- For neuritis: extend treatment with prednisolone from 20 mg onwards for 4 additional weeks
- Bed rest + splinting for affected nerve trunks + analgesics
- High-dose glucocorticoids may also be used prophylactically at treatment onset in high-risk patients (Harrison's)
Type 2 (ENL)
Mild ENL: Analgesics/antipyretics (aspirin)
Severe ENL:
- Thalidomide 100-400 mg/day - drug of choice for severe/recurrent ENL (inhibits TNF-α, reduces neutrophil recruitment and FcγRI expression)
- Prednisolone 1-2 mg/kg/day (as per reversal reaction regimen)
- Clofazimine 100 mg TID × 4 weeks → 100 mg BD × 4 weeks → 100 mg OD × 4 weeks (add-on in ENL; less potent than steroids, takes 4-6 weeks for full effect - never use as the sole agent in severe ENL)
- Pentoxifylline 400 mg three times a day (alternative)
- Total clofazimine therapy should not exceed 12 months
Note: Rifampin is generally not started during an active reversal reaction or ENL because its high kill rate causes massive bacterial antigen release (Goodman & Gilman's).
High-Risk Groups for Lepra Reaction
People more likely to develop reactions and nerve damage include:
- Multi-bacillary leprosy
- Past or present thickened/tender nerve trunks
- Pre-existing nerve function impairment
- Skin lesions on the face
Complications
- Permanent nerve damage - the most feared complication of reversal reaction
- Renal involvement (proteinuria, nephrotic syndrome, RPGN) - especially in ENL
- Musculoskeletal: acute polyarthritis, Charcot joints
- Acral osteolysis, saddle-nose deformity, vertebral kyphosis (in advanced lepromatous disease with reactions)
- Social stigmatization and disability
Important Notes on Steroid Therapy
Prolonged steroid therapy risks include: weight gain, peptic ulcer, diabetes, hypertension, reactivation of tuberculosis, osteoporosis, and psychiatric disorders.
Before starting steroids, assess for:
- Epigastric pain/diarrhea (peptic disease)
- Fungal infection, scabies, worm infestations (worsened by steroids)
Sources: Park's Textbook of Preventive and Social Medicine | Fitzpatrick's Dermatology (5th ed.) | Harrison's Principles of Internal Medicine (22nd ed., 2025) | Goodman & Gilman's Pharmacological Basis of Therapeutics | Rheumatology 2-Volume Set (Elsevier 2022)
Recent literature (PMID 39912169): A 2025 review in Indian J Dermatol Venereol Leprol covers new knowledge on pathophysiology, diagnosis, treatment and prevention of leprosy reactions - consistent with the above framework.
This is a shared conversation. Sign in to Orris to start your own chat.