I need a ppt on nutrition in icu o am sending 3 pdfs for references
You need to extract ALL content related to nutrition in the ICU from a large medical PDF textbook. The PDF is at: /home/daytona/workspace/attachments/b74c6eab-7398-4c51-9150-4c84a1793395/Paul Marinos The ICU Book 4e.pdf Use Python with pypdf to: 1. First, scan the table of contents / index pages to find all chapters, sections, or pages related to: nutrition, enteral nutrition, parenteral nutrition, TPN, feeding, caloric requirements, protein requirements, nitrogen balance, malnutrition, metabolic support, hyperalimentation, glucose control in ICU, energy expenditure, indirect calorimetry, micronutrients, vitamins, trace elements, glutamine, omega-3 fatty acids, immunonutrition. 2. Extract the FULL text from those relevant pages/chapters. 3. Return a detailed, structured summary of all nutrition-related content found, including: - Key principles and concepts - Specific numbers/doses/targets (calories, protein g/kg, glucose targets, etc.) - Tables or data mentioned - Enteral vs parenteral nutrition guidance - Timing of feeding - Special formulas or considerations - Any algorithms or protocols mentioned - Page numbers where found Write a Python script to do this extraction and execute it. Return the complete extracted content (as much detail as possible) as your final answer.
You need to extract ALL content related to nutrition in the ICU from a large medical PDF textbook. The PDF is at: /home/daytona/workspace/attachments/b74c6eab-7398-4c51-9150-4c84a1793395/Washington Manual Of Critical Care- V.V.I (2).pdf Use Python with pypdf to: 1. First, scan the table of contents / index pages to find all chapters, sections, or pages related to: nutrition, enteral nutrition, parenteral nutrition, TPN, feeding, caloric requirements, protein requirements, nitrogen balance, malnutrition, metabolic support, hyperalimentation, glucose control, energy expenditure, indirect calorimetry, micronutrients, vitamins, trace elements, glutamine, omega-3 fatty acids, immunonutrition. 2. Extract the FULL text from those relevant pages/chapters. 3. Return a detailed, structured summary of all nutrition-related content found, including: - Key principles and concepts - Specific numbers/doses/targets (calories, protein g/kg, glucose targets, etc.) - Tables or data mentioned - Enteral vs parenteral nutrition guidance - Timing of feeding - Special formulas or considerations - Any algorithms or protocols mentioned - Page numbers where found Write a Python script to do this extraction and execute it. Return the complete extracted content (as much detail as possible) as your final answer.
You need to extract ALL content related to nutrition in the ICU from a large medical PDF textbook. The PDF is at: /home/daytona/workspace/attachments/b74c6eab-7398-4c51-9150-4c84a1793395/Irwin_and_Rippe_s_Intensive_Care_Medicine_2Vol_Set_9E_ALGrawany 2.pdf Use Python with pypdf to: 1. First, scan the table of contents / index pages to find all chapters, sections, or pages related to: nutrition, enteral nutrition, parenteral nutrition, TPN, feeding, caloric requirements, protein requirements, nitrogen balance, malnutrition, metabolic support, hyperalimentation, glucose control, energy expenditure, indirect calorimetry, micronutrients, vitamins, trace elements, glutamine, omega-3 fatty acids, immunonutrition. 2. Extract the FULL text from those relevant pages/chapters. 3. Return a detailed, structured summary of all nutrition-related content found, including: - Key principles and concepts - Specific numbers/doses/targets (calories, protein g/kg, glucose targets, etc.) - Tables or data mentioned - Enteral vs parenteral nutrition guidance - Timing of feeding - Special formulas or considerations - Any algorithms or protocols mentioned - Page numbers where found Write a Python script to do this extraction and execute it. Return the complete extracted content (as much detail as possible) as your final answer.
~/extract_nutrition.py
#!/usr/bin/env python3
"""
Extract ALL nutrition-related content from the Washington Manual of Critical Care PDF.
"""
import re
import sys
from pypdf import PdfReader
PDF_PATH = "/home/daytona/workspace/attachments/b74c6eab-7398-4c51-9150-4c84a1793395/Washington Manual Of Critical Care- V.V.I (2).pdf"
# Keywords to search for (case-insensitive)
NUTRITION_KEYWORDS = [
"nutrition", "nutritional", "enteral", "parenteral", "tpn", "pn ",
"total parenteral", "nasogastric", "nasoenteric", "jejunal", "jejunostomy",
"gastrostomy", "feeding", "feed ", "tube feed",
"caloric", "calorie", "calories", "kcal", "energy expenditure",
"protein requirement", "protein need", "nitrogen balance", "nitrogen",
"malnutrition", "malnourish", "metabolic support", "hyperalimentation",
"glucose control", "glycemic", "insulin infusion",
"indirect calorimetry", "resting energy", "harris-benedict", "mifflin",
"micronutrient", "vitamin", "trace element", "zinc", "selenium", "copper",
"glutamine", "omega-3", "omega 3", "fish oil", "immunonutrition",
"arginine", "probiotic", "prebiotic", "synbiotic",
"refeeding", "re-feeding", "starvation",
"body weight", "ideal body weight", "adjusted body weight",
"albumin", "prealbumin", "transferrin", "visceral protein",
"resting metabolic", "basal metabolic",
"carbohydrate", "lipid emulsion", "dextrose infusion",
"nasojejunal", "post-pyloric", "gastric residual",
"motility", "prokinetic", "bowel function",
"icu nutrition", "critical illness nutrition",
"permissive underfeeding", "trophic", "hypocaloric",
]
def page_has_nutrition_content(text):
"""Return True if the page text contains any nutrition keywords."""
text_lower = text.lower()
for kw in NUTRITION_KEYWORDS:
if kw.lower() in text_lower:
return True
return False
def extract_toc_and_index(reader):
"""Try to extract table of contents and index pages."""
toc_pages = []
index_pages = []
total_pages = len(reader.pages)
# Check first 30 pages for TOC
for i in range(min(30, total_pages)):
text = reader.pages[i].extract_text() or ""
if any(word in text.lower() for word in ["contents", "table of contents", "chapter"]):
toc_pages.append((i + 1, text))
# Check last 50 pages for index
start_idx = max(0, total_pages - 60)
for i in range(start_idx, total_pages):
text = reader.pages[i].extract_text() or ""
if any(word in text.lower() for word in ["index", "nutrition", "enteral", "parenteral"]):
index_pages.append((i + 1, text))
return toc_pages, index_pages
def find_nutrition_chapters_from_toc(toc_texts):
"""Parse TOC text to find nutrition-related chapters and their page numbers."""
nutrition_entries = []
for page_num, text in toc_texts:
lines = text.split('\n')
for line in lines:
line_lower = line.lower()
if any(kw.lower() in line_lower for kw in NUTRITION_KEYWORDS[:25]):
nutrition_entries.append({
'toc_page': page_num,
'line': line.strip()
})
return nutrition_entries
def extract_page_numbers_from_toc_entries(entries):
"""Try to extract page numbers from TOC entries."""
page_numbers = []
for entry in entries:
line = entry['line']
# Look for numbers at end of line (common TOC format)
matches = re.findall(r'\b(\d{1,4})\b', line)
if matches:
# Take the last number which is usually the page number
try:
pg = int(matches[-1])
if 1 <= pg <= 2000: # Reasonable page range
page_numbers.append(pg)
except:
pass
return list(set(page_numbers))
def main():
print(f"Loading PDF: {PDF_PATH}")
reader = PdfReader(PDF_PATH)
total_pages = len(reader.pages)
print(f"Total pages: {total_pages}")
print("=" * 80)
# Step 1: Extract TOC
print("\n### STEP 1: SCANNING TABLE OF CONTENTS AND INDEX ###\n")
toc_pages, index_pages = extract_toc_and_index(reader)
print(f"Found {len(toc_pages)} potential TOC pages")
print(f"Found {len(index_pages)} potential index pages")
# Print TOC pages
print("\n--- TABLE OF CONTENTS PAGES ---")
for page_num, text in toc_pages:
print(f"\n[TOC Page {page_num}]")
print(text[:3000])
print("---")
# Step 2: Find nutrition entries in TOC
nutrition_toc_entries = find_nutrition_chapters_from_toc(toc_pages)
print(f"\n### NUTRITION-RELATED TOC ENTRIES ({len(nutrition_toc_entries)}) ###")
for entry in nutrition_toc_entries:
print(f" TOC p.{entry['toc_page']}: {entry['line']}")
# Step 3: Scan ALL pages for nutrition content
print("\n### STEP 2: SCANNING ALL PAGES FOR NUTRITION KEYWORDS ###\n")
nutrition_pages = []
page_texts = {}
for i in range(total_pages):
try:
text = reader.pages[i].extract_text() or ""
page_texts[i + 1] = text
if page_has_nutrition_content(text):
nutrition_pages.append(i + 1)
except Exception as e:
print(f"Error reading page {i+1}: {e}")
print(f"Found {len(nutrition_pages)} pages with nutrition-related content")
print(f"Pages: {nutrition_pages}")
# Step 4: Group consecutive pages into sections
def group_pages(page_list):
if not page_list:
return []
groups = []
start = page_list[0]
end = page_list[0]
for p in page_list[1:]:
if p <= end + 3: # Allow small gaps
end = p
else:
groups.append((start, end))
start = p
end = p
groups.append((start, end))
return groups
page_groups = group_pages(nutrition_pages)
print(f"\nPage groups (consecutive sections):")
for start, end in page_groups:
print(f" Pages {start}-{end} ({end - start + 1} pages)")
# Step 5: Extract and print full text from nutrition pages
print("\n" + "=" * 80)
print("### STEP 3: FULL TEXT OF ALL NUTRITION-RELATED PAGES ###")
print("=" * 80)
for page_num in nutrition_pages:
text = page_texts.get(page_num, "")
if text.strip():
print(f"\n{'='*80}")
print(f"PAGE {page_num}")
print('='*80)
print(text)
# Step 6: Print index nutrition entries
print("\n" + "=" * 80)
print("### STEP 4: NUTRITION ENTRIES IN INDEX ###")
print("=" * 80)
for page_num, text in index_pages:
lines = text.split('\n')
for line in lines:
if any(kw.lower() in line.lower() for kw in NUTRITION_KEYWORDS[:20]):
print(f" Index p.{page_num}: {line.strip()}")
print("\n" + "=" * 80)
print(f"EXTRACTION COMPLETE: {len(nutrition_pages)} nutrition-related pages found")
print("=" * 80)
if __name__ == "__main__":
main()
~/extract_nutrition.py
#!/usr/bin/env python3
"""
Extract ALL nutrition-related content from Paul Marino's The ICU Book 4th edition.
Steps:
1. Scan every page for nutrition keywords to locate relevant pages.
2. Also parse the table of contents / index to find chapter page ranges.
3. Extract full text of all matching pages.
4. Write a structured summary to a text file.
"""
import re
import sys
from pypdf import PdfReader
PDF_PATH = "/home/daytona/workspace/attachments/b74c6eab-7398-4c51-9150-4c84a1793395/Paul Marinos The ICU Book 4e.pdf"
OUTPUT_PATH = "/home/daytona/workspace/nutrition_extraction.txt"
# ─── keyword lists ────────────────────────────────────────────────────────────
NUTRITION_KEYWORDS = [
"nutrition", "nutritional", "enteral", "parenteral", "tpn", "total parenteral",
"feeding", "tube feed", "nasogastric", "nasoduodenal", "nasojejunal",
"caloric", "calorie", "calories", "kcal", "kilocalorie",
"protein requirement", "protein intake", "nitrogen balance", "nitrogen loss",
"malnutrition", "malnourish", "undernutrition",
"metabolic support", "hyperalimentation",
"glucose control", "glycemic control", "insulin infusion", "blood glucose",
"energy expenditure", "resting energy", "indirect calorimetry", "calorimetry",
"harris-benedict", "harris benedict",
"micronutrient", "vitamin", "trace element", "zinc", "selenium", "copper",
"glutamine", "omega-3", "omega 3", "fish oil", "immunonutrition",
"arginine", "antioxidant",
"refeeding syndrome", "refeeding",
"bowel function", "gut function", "splanchnic",
"carbohydrate", "lipid emulsion", "fat emulsion", "dextrose infusion",
"albumin", "prealbumin", "transferrin", # nutritional markers
"energy balance", "substrate", "catabolism", "anabolism",
"kwashiorkor", "marasmus",
]
TOC_KEYWORDS = [
"nutrition", "nutritional", "enteral", "parenteral", "tpn", "feeding",
"caloric", "calorie", "nitrogen", "malnutrition", "metabolic support",
"glucose control", "energy expenditure", "calorimetry", "micronutrient",
"vitamin", "trace element", "glutamine", "immunonutrition", "hyperalimentation",
]
CHAPTER_KEYWORDS = [
"nutrition", "nutritional support", "enteral nutrition", "parenteral nutrition",
"feeding", "metabolic support", "energy", "nitrogen",
]
# ─── helpers ──────────────────────────────────────────────────────────────────
def page_contains_keyword(text: str, keywords: list) -> bool:
lower = text.lower()
return any(kw in lower for kw in keywords)
def highlight_keywords(text: str, keywords: list) -> str:
"""Return text with a simple marker before each keyword occurrence."""
return text # Return raw – we'll show full text
def extract_toc_info(reader: PdfReader, max_toc_pages: int = 30):
"""Scan first max_toc_pages pages for a table of contents."""
toc_text = []
toc_page_nums = []
for i in range(min(max_toc_pages, len(reader.pages))):
text = reader.pages[i].extract_text() or ""
lower = text.lower()
# TOC pages usually have lots of dots / numbers after section titles
if ("contents" in lower or "chapter" in lower) and re.search(r'\d{2,}', text):
toc_text.append((i + 1, text))
toc_page_nums.append(i)
return toc_text, toc_page_nums
def find_nutrition_pages(reader: PdfReader):
"""Return dict {pdf_page_index: text} for pages matching nutrition keywords."""
hits = {}
total = len(reader.pages)
print(f" Scanning {total} pages for nutrition keywords …", flush=True)
for i, page in enumerate(reader.pages):
if i % 100 == 0:
print(f" … page {i}/{total}", flush=True)
text = page.extract_text() or ""
if page_contains_keyword(text, NUTRITION_KEYWORDS):
hits[i] = text
return hits
def detect_chapter_boundaries(reader: PdfReader):
"""
Find pages that start a new chapter/section, especially nutrition-related ones.
Returns list of (page_index, heading_text).
"""
chapters = []
for i, page in enumerate(reader.pages):
text = page.extract_text() or ""
# Look for lines that look like chapter headings
lines = text.split("\n")
for line in lines[:10]: # usually at top of page
clean = line.strip()
if len(clean) > 5 and page_contains_keyword(clean, CHAPTER_KEYWORDS):
chapters.append((i, clean))
break
return chapters
def build_nutrition_ranges(hit_page_indices: list, reader_len: int, context: int = 1):
"""
Expand single hit pages by ±context pages and merge overlapping ranges.
Returns list of (start, end) inclusive page index ranges.
"""
if not hit_page_indices:
return []
indices = sorted(set(hit_page_indices))
ranges = []
start = max(0, indices[0] - context)
end = min(reader_len - 1, indices[0] + context)
for idx in indices[1:]:
new_start = max(0, idx - context)
new_end = min(reader_len - 1, idx + context)
if new_start <= end + 1:
end = max(end, new_end)
else:
ranges.append((start, end))
start, end = new_start, new_end
ranges.append((start, end))
return ranges
def keyword_density(text: str, keywords: list) -> int:
lower = text.lower()
return sum(lower.count(kw) for kw in keywords)
# ─── main ─────────────────────────────────────────────────────────────────────
def main():
print("=" * 70)
print("Nutrition Content Extractor – Paul Marino's The ICU Book 4e")
print("=" * 70)
reader = PdfReader(PDF_PATH)
total_pages = len(reader.pages)
print(f"\nTotal pages in PDF: {total_pages}\n")
# ── Step 1: Extract TOC / Index ──────────────────────────────────────────
print("Step 1: Scanning Table of Contents …")
toc_text, toc_page_nums = extract_toc_info(reader, max_toc_pages=40)
print(f" Found {len(toc_text)} TOC-like page(s): {[p+1 for p in toc_page_nums]}")
# Filter TOC entries that mention nutrition
toc_nutrition_entries = []
for pnum, text in toc_text:
for line in text.split("\n"):
if page_contains_keyword(line, TOC_KEYWORDS):
toc_nutrition_entries.append((pnum, line.strip()))
print(f"\n Nutrition-related TOC entries ({len(toc_nutrition_entries)}):")
for pnum, entry in toc_nutrition_entries:
print(f" [TOC p.{pnum}] {entry}")
# ── Step 2: Scan all pages ────────────────────────────────────────────────
print("\nStep 2: Scanning all pages for nutrition keywords …")
hit_pages = find_nutrition_pages(reader)
print(f" Found {len(hit_pages)} pages containing nutrition keywords.")
# Sort by keyword density to find the most content-rich pages
ranked = sorted(hit_pages.items(), key=lambda x: keyword_density(x[1], NUTRITION_KEYWORDS), reverse=True)
print("\n Top 30 pages by keyword density:")
for idx, text in ranked[:30]:
density = keyword_density(text, NUTRITION_KEYWORDS)
print(f" PDF page index {idx:4d} (book page ~{idx+1}) density={density}")
# ── Step 3: Build page ranges ─────────────────────────────────────────────
print("\nStep 3: Expanding ranges and identifying nutrition chapters …")
hit_indices = list(hit_pages.keys())
ranges = build_nutrition_ranges(hit_indices, total_pages, context=0)
print(f" Merged into {len(ranges)} continuous range(s).")
# Identify large contiguous blocks (likely whole chapters)
large_ranges = [(s, e) for s, e in ranges if (e - s + 1) >= 5]
print(f" Large ranges (≥5 pages): {len(large_ranges)}")
for s, e in large_ranges:
print(f" Pages {s+1}–{e+1} ({e-s+1} pages)")
# ── Step 4: Extract and write ─────────────────────────────────────────────
print("\nStep 4: Extracting full text of all nutrition pages …")
with open(OUTPUT_PATH, "w", encoding="utf-8") as out:
out.write("=" * 80 + "\n")
out.write("NUTRITION CONTENT EXTRACTED FROM: Paul Marino's The ICU Book 4th Edition\n")
out.write("=" * 80 + "\n\n")
# ── TOC section ──
out.write("=" * 80 + "\n")
out.write("SECTION A: TABLE OF CONTENTS – NUTRITION ENTRIES\n")
out.write("=" * 80 + "\n\n")
for pnum, entry in toc_nutrition_entries:
out.write(f" [TOC p.{pnum}] {entry}\n")
out.write("\n")
# ── Full TOC pages ──
out.write("=" * 80 + "\n")
out.write("SECTION B: FULL TEXT OF TABLE OF CONTENTS PAGES\n")
out.write("=" * 80 + "\n\n")
for pnum, text in toc_text:
out.write(f"\n{'─'*60}\n")
out.write(f"PDF PAGE {pnum} (TOC)\n")
out.write(f"{'─'*60}\n")
out.write(text)
out.write("\n")
# ── All nutrition pages ──
out.write("\n" + "=" * 80 + "\n")
out.write("SECTION C: FULL TEXT OF ALL NUTRITION-RELATED PAGES\n")
out.write(f"({len(hit_pages)} pages found)\n")
out.write("=" * 80 + "\n\n")
for idx in sorted(hit_pages.keys()):
text = hit_pages[idx]
density = keyword_density(text, NUTRITION_KEYWORDS)
out.write(f"\n{'═'*70}\n")
out.write(f"PDF PAGE INDEX: {idx} | BOOK PAGE ~{idx+1} | Keyword density: {density}\n")
out.write(f"{'═'*70}\n")
out.write(text)
out.write("\n")
file_size = __import__('os').path.getsize(OUTPUT_PATH)
print(f"\n Output written to: {OUTPUT_PATH}")
print(f" File size: {file_size:,} bytes ({file_size/1024:.1f} KB)")
# ── Step 5: Print a console summary ──────────────────────────────────────
print("\n" + "=" * 70)
print("STEP 5: CONSOLE PREVIEW – TOP NUTRITION PAGES")
print("=" * 70)
# Print top 15 pages fully
for idx, text in ranked[:15]:
density = keyword_density(text, NUTRITION_KEYWORDS)
print(f"\n{'═'*70}")
print(f"PDF PAGE {idx+1} (index={idx}) [density={density}]")
print(f"{'─'*70}")
print(text[:3000]) # first 3000 chars
if len(text) > 3000:
print(f"\n … [truncated, full text in output file] …")
print()
return hit_pages, toc_nutrition_entries, ranges
if __name__ == "__main__":
hit_pages, toc_entries, ranges = main()
print("\n✓ Extraction complete.")
cd /home/daytona/workspace && python extract_nutrition.py > nutrition_output.txt…
wc -l /home/daytona/workspace/nutrition_output.txt && wc -c /home/daytona/worksp…
~/extract_nutrition.py
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/extract_nutrition.py'
~/extract_nutrition_v2.py
#!/usr/bin/env python3
"""
Extract ALL nutrition-related content from Paul Marino's The ICU Book 4th edition.
Steps:
1. Scan every page for nutrition keywords to locate relevant pages.
2. Parse the table of contents / index pages.
3. Extract full text of all matching pages.
4. Write a structured output file and print a console summary.
"""
import re
import os
import sys
from pypdf import PdfReader
PDF_PATH = "/home/daytona/workspace/attachments/b74c6eab-7398-4c51-9150-4c84a1793395/Paul Marinos The ICU Book 4e.pdf"
OUTPUT_PATH = "/home/daytona/workspace/nutrition_extraction.txt"
# ─── keyword lists ────────────────────────────────────────────────────────────
NUTRITION_KEYWORDS = [
"nutrition", "nutritional", "enteral", "parenteral", "tpn", "total parenteral",
"feeding", "tube feed", "nasogastric", "nasoduodenal", "nasojejunal",
"caloric", "calorie", "calories", "kcal", "kilocalorie",
"protein requirement", "protein intake", "nitrogen balance", "nitrogen loss",
"malnutrition", "malnourish", "undernutrition",
"metabolic support", "hyperalimentation",
"glucose control", "glycemic control", "insulin infusion", "blood glucose",
"energy expenditure", "resting energy", "indirect calorimetry", "calorimetry",
"harris-benedict", "harris benedict",
"micronutrient", "vitamin", "trace element", "zinc", "selenium", "copper",
"glutamine", "omega-3", "omega 3", "fish oil", "immunonutrition",
"arginine", "antioxidant",
"refeeding syndrome", "refeeding",
"bowel function", "gut function", "splanchnic",
"carbohydrate", "lipid emulsion", "fat emulsion", "dextrose infusion",
"albumin", "prealbumin", "transferrin",
"energy balance", "substrate", "catabolism", "anabolism",
"kwashiorkor", "marasmus",
]
TOC_KEYWORDS = [
"nutrition", "nutritional", "enteral", "parenteral", "tpn", "feeding",
"caloric", "calorie", "nitrogen", "malnutrition", "metabolic support",
"glucose control", "energy expenditure", "calorimetry", "micronutrient",
"vitamin", "trace element", "glutamine", "immunonutrition", "hyperalimentation",
]
CHAPTER_KEYWORDS = [
"nutrition", "nutritional support", "enteral nutrition", "parenteral nutrition",
"feeding", "metabolic support", "energy", "nitrogen",
]
# ─── helpers ──────────────────────────────────────────────────────────────────
def page_contains_keyword(text, keywords):
lower = text.lower()
return any(kw in lower for kw in keywords)
def keyword_density(text, keywords):
lower = text.lower()
return sum(lower.count(kw) for kw in keywords)
def extract_toc_info(reader, max_toc_pages=40):
toc_text = []
for i in range(min(max_toc_pages, len(reader.pages))):
text = reader.pages[i].extract_text() or ""
lower = text.lower()
if ("contents" in lower or "chapter" in lower) and re.search(r'\d{2,}', text):
toc_text.append((i + 1, text))
return toc_text
def find_nutrition_pages(reader):
hits = {}
total = len(reader.pages)
print(f" Scanning {total} pages for nutrition keywords ...", flush=True)
for i, page in enumerate(reader.pages):
if i % 100 == 0:
print(f" ... page {i}/{total}", flush=True)
text = page.extract_text() or ""
if page_contains_keyword(text, NUTRITION_KEYWORDS):
hits[i] = text
return hits
# ─── main ─────────────────────────────────────────────────────────────────────
def main():
print("=" * 70)
print("Nutrition Content Extractor -- Paul Marino's The ICU Book 4e")
print("=" * 70)
reader = PdfReader(PDF_PATH)
total_pages = len(reader.pages)
print(f"\nTotal pages in PDF: {total_pages}\n")
# Step 1: TOC
print("Step 1: Scanning Table of Contents ...")
toc_pages = extract_toc_info(reader, max_toc_pages=40)
print(f" Found {len(toc_pages)} TOC-like page(s).")
toc_nutrition_entries = []
for pnum, text in toc_pages:
for line in text.split("\n"):
if page_contains_keyword(line, TOC_KEYWORDS):
toc_nutrition_entries.append((pnum, line.strip()))
print(f" Nutrition-related TOC entries: {len(toc_nutrition_entries)}")
for pnum, entry in toc_nutrition_entries:
print(f" [TOC p.{pnum}] {entry}")
# Step 2: Scan all pages
print("\nStep 2: Scanning all pages ...")
hit_pages = find_nutrition_pages(reader)
print(f" Found {len(hit_pages)} pages containing nutrition keywords.")
ranked = sorted(hit_pages.items(), key=lambda x: keyword_density(x[1], NUTRITION_KEYWORDS), reverse=True)
print("\n Top 40 pages by keyword density:")
for idx, text in ranked[:40]:
density = keyword_density(text, NUTRITION_KEYWORDS)
print(f" Page index {idx:4d} (book page approx {idx+1:4d}) density={density}")
# Step 3: Write output file
print("\nStep 3: Writing extracted content to file ...")
with open(OUTPUT_PATH, "w", encoding="utf-8") as out:
out.write("=" * 80 + "\n")
out.write("NUTRITION CONTENT: Paul Marino's The ICU Book, 4th Edition\n")
out.write("=" * 80 + "\n\n")
out.write("SECTION A: TABLE OF CONTENTS -- NUTRITION ENTRIES\n")
out.write("-" * 60 + "\n")
for pnum, entry in toc_nutrition_entries:
out.write(f" [TOC p.{pnum}] {entry}\n")
out.write("\n")
out.write("SECTION B: FULL TEXT OF TABLE OF CONTENTS PAGES\n")
out.write("-" * 60 + "\n")
for pnum, text in toc_pages:
out.write(f"\n--- TOC PAGE {pnum} ---\n")
out.write(text)
out.write("\n")
out.write("\nSECTION C: ALL NUTRITION-RELATED PAGES (full text)\n")
out.write(f"Total pages: {len(hit_pages)}\n")
out.write("-" * 60 + "\n")
for idx in sorted(hit_pages.keys()):
text = hit_pages[idx]
density = keyword_density(text, NUTRITION_KEYWORDS)
out.write(f"\n{'='*70}\n")
out.write(f"PAGE INDEX {idx} | ~Book page {idx+1} | density={density}\n")
out.write(f"{'='*70}\n")
out.write(text)
out.write("\n")
sz = os.path.getsize(OUTPUT_PATH)
print(f" Written: {OUTPUT_PATH} ({sz:,} bytes, {sz/1024:.1f} KB)")
# Step 4: Console output of top pages
print("\n" + "=" * 70)
print("CONSOLE PREVIEW: TOP NUTRITION PAGES (full text, up to 5000 chars each)")
print("=" * 70)
for idx, text in ranked[:20]:
density = keyword_density(text, NUTRITION_KEYWORDS)
print(f"\n{'='*70}")
print(f" PDF PAGE INDEX {idx} (~book page {idx+1}) [keyword hits: {density}]")
print(f"{'='*70}")
print(text[:5000])
if len(text) > 5000:
print(f"\n... [page continues, {len(text)-5000} more chars in output file] ...")
return hit_pages, toc_nutrition_entries
if __name__ == "__main__":
hit_pages, toc_entries = main()
print("\nDone.")
cd /home/daytona/workspace && python extract_nutrition_v2.py 2>&1
cd /home/daytona/workspace && python3 << 'EOF' from pypdf import PdfReader impor…
mkdir -p /home/daytona/workspace/icu-nutrition-ppt && ls /home/daytona/workspace…
Where is ppt
~/icu-nutrition-ppt/nutrition_icu.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_16x9";
pres.title = "Nutrition in the ICU";
pres.author = "Critical Care Team";
// ─── COLOUR PALETTE ───────────────────────────────────────────────
const C = {
navy: "0D2B4E", // dominant dark
teal: "0E7C7B", // accent headers
gold: "E8A020", // highlight / numbers
white: "FFFFFF",
offwhite:"F4F6F9",
ltgray: "D8E3EC",
midgray: "6B7F96",
red: "C0392B",
green: "1A7A4A",
orange: "D4700A",
text: "1A2B3C",
};
// ─── HELPERS ──────────────────────────────────────────────────────
function titleSlide(title, subtitle) {
const s = pres.addSlide();
// full background
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:10, h:5.625, fill:{color:C.navy} });
// teal accent bar
s.addShape(pres.ShapeType.rect, { x:0, y:4.2, w:10, h:0.18, fill:{color:C.teal} });
s.addShape(pres.ShapeType.rect, { x:0, y:4.38, w:10, h:0.06, fill:{color:C.gold} });
s.addText(title, { x:0.5, y:1.2, w:9, h:1.6, fontSize:40, bold:true, color:C.white, align:"center", fontFace:"Calibri" });
if (subtitle) s.addText(subtitle, { x:0.5, y:2.9, w:9, h:0.7, fontSize:20, color:C.ltgray, align:"center", fontFace:"Calibri", italic:true });
s.addText("References: Marino's ICU Book 4e • Washington Manual of Critical Care • Irwin & Rippe's Intensive Care Medicine 9e",
{ x:0.3, y:4.9, w:9.4, h:0.5, fontSize:9, color:C.midgray, align:"center", fontFace:"Calibri" });
return s;
}
function sectionDivider(label) {
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:10, h:5.625, fill:{color:C.teal} });
s.addShape(pres.ShapeType.rect, { x:0, y:2.55, w:10, h:0.08, fill:{color:C.gold} });
s.addText(label, { x:0.6, y:1.7, w:8.8, h:1.6, fontSize:36, bold:true, color:C.white, align:"center", fontFace:"Calibri" });
return s;
}
function contentSlide(title, bullets, opts={}) {
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:10, h:5.625, fill:{color:C.offwhite} });
// header bar
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:10, h:0.82, fill:{color:C.navy} });
s.addShape(pres.ShapeType.rect, { x:0, y:0.82, w:10, h:0.07, fill:{color:C.teal} });
s.addText(title, { x:0.35, y:0.08, w:9.3, h:0.66, fontSize:22, bold:true, color:C.white, valign:"middle", fontFace:"Calibri", margin:0 });
const txtItems = bullets.map((b, i) => {
if (b.startsWith("##")) {
return [
{ text: b.replace("##","").trim(), options:{ bold:true, color:C.teal, fontSize: opts.fs||15, breakLine: i<bullets.length-1 } }
];
}
if (b.startsWith("!")) {
return [
{ text: "⚠ " + b.replace("!","").trim(), options:{ bold:true, color:C.red, fontSize: opts.fs||14, breakLine: i<bullets.length-1 } }
];
}
if (b.startsWith(">")) {
return [
{ text: b.replace(">","").trim(), options:{ color:C.green, fontSize: opts.fs||14, italic:true, breakLine: i<bullets.length-1 } }
];
}
const isIndent = b.startsWith(" ");
return [
{ text: (isIndent ? " • " : "• ") + b.trim(),
options:{ color: C.text, fontSize: opts.fs||(isIndent?13:14), breakLine: i<bullets.length-1 } }
];
});
const flat = txtItems.flat();
s.addText(flat, { x:0.35, y:1.05, w:9.3, h:4.4, valign:"top", fontFace:"Calibri", lineSpacingMultiple:1.25 });
return s;
}
function twoColSlide(title, leftItems, rightItems, leftHead="", rightHead="") {
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:10, h:5.625, fill:{color:C.offwhite} });
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:10, h:0.82, fill:{color:C.navy} });
s.addShape(pres.ShapeType.rect, { x:0, y:0.82, w:10, h:0.07, fill:{color:C.teal} });
s.addText(title, { x:0.35, y:0.08, w:9.3, h:0.66, fontSize:22, bold:true, color:C.white, valign:"middle", fontFace:"Calibri", margin:0 });
// divider
s.addShape(pres.ShapeType.line, { x:5.05, y:1.0, w:0, h:4.4, line:{color:C.ltgray, width:1.5} });
function col(items, x, head) {
let arr = [];
if (head) arr.push({ text: head+"\n", options:{ bold:true, color:C.teal, fontSize:15 } });
items.forEach((b,i) => {
if (b.startsWith("##")) {
arr.push({ text: b.replace("##","").trim()+"\n", options:{ bold:true, color:C.teal, fontSize:14 } });
} else if (b.startsWith("!")) {
arr.push({ text: "⚠ "+b.replace("!","").trim()+"\n", options:{ bold:true, color:C.red, fontSize:13 } });
} else if (b.startsWith(">")) {
arr.push({ text: b.replace(">","").trim()+"\n", options:{ color:C.green, italic:true, fontSize:13 } });
} else {
const ind = b.startsWith(" ");
arr.push({ text: (ind?" – ":"• ")+b.trim()+"\n", options:{ color:C.text, fontSize: ind?12:13 } });
}
});
s.addText(arr, { x, y:1.05, w:4.55, h:4.4, valign:"top", fontFace:"Calibri", lineSpacingMultiple:1.3 });
}
col(leftItems, 0.3, leftHead);
col(rightItems, 5.15, rightHead);
return s;
}
function tableSlide(title, headers, rows, colW) {
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:10, h:5.625, fill:{color:C.offwhite} });
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:10, h:0.82, fill:{color:C.navy} });
s.addShape(pres.ShapeType.rect, { x:0, y:0.82, w:10, h:0.07, fill:{color:C.teal} });
s.addText(title, { x:0.35, y:0.08, w:9.3, h:0.66, fontSize:22, bold:true, color:C.white, valign:"middle", fontFace:"Calibri", margin:0 });
const tableData = [
headers.map(h => ({ text: h, options:{ bold:true, color:C.white, fill:{color:C.teal}, fontSize:13, fontFace:"Calibri", align:"center" } })),
...rows.map((r,ri) => r.map(cell => ({
text: cell,
options:{ fontSize:12, fontFace:"Calibri", color:C.text, fill:{color: ri%2===0 ? C.white : C.ltgray }, align:"center" }
})))
];
s.addTable(tableData, { x:0.25, y:1.05, w:9.5, colW: colW||headers.map(()=>9.5/headers.length), border:{color:C.ltgray}, autoPage:false });
return s;
}
// ══════════════════════════════════════════════════════════════════
// SLIDE 1 – TITLE
// ══════════════════════════════════════════════════════════════════
titleSlide("NUTRITION IN THE ICU", "Evidence-Based Approach for Critical Care Physicians");
// ══════════════════════════════════════════════════════════════════
// SLIDE 2 – OUTLINE
// ══════════════════════════════════════════════════════════════════
contentSlide("Presentation Outline", [
"##1. Metabolic Response to Critical Illness",
"##2. Nutrition Risk Assessment & Screening Tools",
"##3. Energy Requirements & Caloric Targets",
"##4. Protein Requirements",
"##5. Enteral Nutrition – Principles, Timing & Access",
"##6. Enteral Feeding Formulas",
"##7. Parenteral Nutrition – Indications & Composition",
"##8. Monitoring & Complications",
"##9. Special Populations",
"##10. Immunonutrition & Conditionally Essential Nutrients",
"##11. Glucose Management in the ICU",
"##12. Refeeding Syndrome",
"##13. Key Clinical Protocols & Take-Home Points",
], {fs:15});
// ══════════════════════════════════════════════════════════════════
// SECTION 1
// ══════════════════════════════════════════════════════════════════
sectionDivider("1. Metabolic Response to\nCritical Illness");
contentSlide("Why Nutrition Matters: The Metabolic Storm", [
"Critical illness triggers a shift from anabolic → catabolic state",
"Rapid protein breakdown occurs within the first 10 days of ICU admission",
"Consequences of ICU malnutrition:",
" Muscle weakness & neuromuscular dysfunction",
" Prolonged mechanical ventilation",
" Increased infectious complications",
" Longer ICU/hospital length of stay",
" Higher mortality & reduced quality of life",
"##Key Insight (Marino's ICU Book):",
"> ICU malnutrition is caused by METABOLIC DERANGEMENTS — not nutrient depletion.",
"> Providing nutrients will not correct malnutrition until metabolic derangements resolve.",
"Prevalence of adult malnutrition in ICU patients: 15–60%",
"Cumulative caloric deficit ≥10,000 kcal during acute illness worsens outcomes",
]);
contentSlide("Phases of Metabolic Response to Injury", [
"##Phase 1 – Ebb Phase (0–24 hrs post-injury)",
" Hypometabolism, reduced cardiac output, hypothermia",
" Primary goal: resuscitation, not aggressive feeding",
"##Phase 2 – Flow Phase (Hypermetabolic, days 1–7+)",
" Increased O₂ consumption, CO₂ production, REE",
" Accelerated proteolysis, gluconeogenesis, lipolysis",
" Counter-regulatory hormones: glucagon, cortisol, growth hormone",
" Insulin resistance → hyperglycemia universal",
"##Phase 3 – Recovery / Anabolic Phase",
" Gradual normalization of metabolism",
" Window for aggressive nutritional rehabilitation",
"2019 ESPEN guidelines emphasize: recognize and adjust nutrition regimens across ALL phases",
"ASPEN/SCCM 2016 guidelines: nutrition support now a standard of care, not optional",
]);
// ══════════════════════════════════════════════════════════════════
// SECTION 2
// ══════════════════════════════════════════════════════════════════
sectionDivider("2. Nutrition Risk Assessment");
contentSlide("Nutrition Risk Screening in the ICU", [
"All ICU patients should be screened within 48 hours of admission",
"##Two validated tools for ICU risk stratification:",
"##NRS-2002 (Nutritional Risk Screening 2002)",
" Score ≥5 = High nutritional risk",
" Factors: % energy intake for 7 days + weight loss + disease severity",
"##NUTRIC Score (Nutrition Risk in Critically Ill)",
" Score ≥5 (without IL-6) = High risk",
" Factors: Age, APACHE II, SOFA score, comorbidities, days hospital → ICU",
"High-risk patients benefit most from early, aggressive nutrition intervention",
"##Important Caveat:",
"! Albumin & pre-albumin are NOT reliable nutrition markers in critical illness",
"> They reflect inflammatory state (acute-phase reactants), NOT nutritional status",
"Bedside muscle ultrasound (quadriceps layer thickness) shows promise for serial monitoring",
]);
tableSlide("NUTRIC Score — Quick Reference",
["Variable", "Range", "Score"],
[
["Age (years)", "< 50", "0"],
["", "50–74", "1"],
["", "≥ 75", "2"],
["APACHE II", "< 15", "0"],
["", "15–19", "1"],
["", "20–27", "2"],
["", "≥ 28", "3"],
["SOFA score", "< 6", "0"],
["", "6–9", "1"],
["", "≥ 10", "2"],
["No. of comorbidities", "0–1", "0"],
["", "≥ 2", "1"],
["Days hosp → ICU", "0–1", "0"],
["", "≥ 1", "1"],
],
[3.5, 3.5, 2.5]
);
// ══════════════════════════════════════════════════════════════════
// SECTION 3
// ══════════════════════════════════════════════════════════════════
sectionDivider("3. Energy Requirements");
contentSlide("Estimating Caloric Requirements", [
"##Gold Standard: Indirect Calorimetry",
" Measures REE from VO₂ and VCO₂ at bedside",
" Requires steady-state measurement × 15–30 min → extrapolate to 24 hrs",
"! Unreliable at FiO₂ ≥ 60% (O₂ sensor limitation)",
" Requires expensive equipment & trained personnel",
"##Practical: Weight-Based Formulas (preferred in most ICUs)",
"> Simple rule: 25 kcal/kg/day — remarkably accurate for most ICU patients (Marino)",
" Adjust for BMI (see table on next slide)",
" Harris-Benedict and Ireton-Jones equations are validated but cumbersome",
"##Body Weight Rules:",
" Actual body weight — for most patients",
" Adjusted body weight — if actual weight >125% of IBW",
" IBW — for morbid obesity (BMI ≥40)",
" Estimated dry weight — for patients with significant edema/ascites",
"##Propofol — Hidden Calories!",
"! Propofol in 10% lipid = 1.1 kcal/mL — MUST subtract from daily caloric target",
]);
tableSlide("Weight-Based Energy Targets by BMI (Washington Manual)",
["BMI (kg/m²)", "Energy Target", "Special Notes"],
[
["< 15", "35–45 kcal/kg/day", "Severe underweight — aggressive repletion"],
["15–19", "30–35 kcal/kg/day", "Underweight — high-risk"],
["20–24", "25–30 kcal/kg/day", "Normal — standard target"],
["25–29", "20–25 kcal/kg/day", "Overweight"],
["30–50", "11–14 kcal/kg/day", "Obese — use actual weight; hypocaloric"],
["> 50", "22–25 kcal/kg IBW/day", "Morbidly obese — use IBW"],
],
[3, 3.5, 3]
);
contentSlide("Substrate Fuel Values & Respiratory Quotient", [
"##Energy Yield of Macronutrients:",
" Lipids: 9.1 kcal/gram (highest)",
" Protein: ~4.0 kcal/gram",
" Glucose: 3.7 kcal/gram",
" Dextrose (IV): 3.4 kcal/gram (used in TPN calculations)",
"##Nonprotein Calorie Split (Standard):",
" ~70% carbohydrate + ~30% lipid",
" In standard EN formulas: nonprotein calories ≈ 85% of total calories",
"##Respiratory Quotient (RQ = VCO₂ / VO₂):",
" Fat oxidation RQ = 0.7",
" Protein oxidation RQ = 0.8",
" Carbohydrate oxidation RQ = 1.0",
" RQ > 1.0 → lipogenesis (OVERFEEDING) → ↑CO₂ → respiratory failure",
" RQ < 0.7 → fat mobilization (underfeeding / ketosis)",
"! Overfeeding with carbohydrates → hypercapnia — dangerous in ventilator-dependent patients",
]);
// ══════════════════════════════════════════════════════════════════
// SECTION 4
// ══════════════════════════════════════════════════════════════════
sectionDivider("4. Protein Requirements");
contentSlide("Protein — The Most Critical Macronutrient in the ICU", [
"##Why Protein is Paramount:",
" Maintains muscle mass and functional reserve",
" Supports enzymatic and structural protein synthesis",
" Higher protein delivery → associated with decreased ICU mortality",
" Protein (not just calories) is the primary driver of lean tissue preservation",
"##General ICU Protein Targets:",
" Standard ICU patients: 1.2–2.0 g/kg/day",
" Trauma / Burns: 1.5–2.0 g/kg/day",
" Traumatic Brain Injury (TBI): 1.5–2.5 g/kg/day",
" Sepsis: 1.2–2.0 g/kg/day",
" BMI 30–40 (obese): 2.0–2.5 g/kg IBW/day",
" BMI >40 (morbidly obese): 2.5 g/kg IBW/day",
"! Providing protein >1.75 g/kg/day exceeds metabolic capacity in some patients — excess converted to urea",
"Use actual body weight for most; IBW for morbid obesity; dry weight for ascites",
]);
tableSlide("Protein Requirements by Clinical Condition",
["Clinical Condition", "Protein (g/kg/day)", "Weight Basis"],
[
["Medical / Surgical ICU", "1.2–2.0", "Actual BW"],
["Sepsis", "1.2–2.0", "Actual BW"],
["Trauma (general)", "1.5–2.0", "Actual BW"],
["Traumatic Brain Injury", "1.5–2.5", "Actual BW"],
["Burns", "1.5–2.0", "Actual BW"],
["Open Abdomen", "1.5–2.0 + 15 g/L exudate", "Actual BW"],
["AKI — No dialysis", "1.0–1.5", "Actual BW"],
["AKI — HD / SLED", "1.5–2.0", "Actual BW"],
["AKI — CRRT", "2.0–2.5", "Actual BW"],
["Hepatic Failure", "1.2–2.0", "Dry Weight"],
["Obesity BMI 30–40", "2.0–2.5", "IBW"],
["Obesity BMI >40", "2.5", "IBW"],
],
[4, 3.5, 2]
);
contentSlide("Nitrogen Balance — Assessing Adequacy", [
"##Nitrogen Balance Formula:",
"> N Balance = Nitrogen Intake − Nitrogen Excretion",
" Nitrogen intake (g/day) = Protein intake (g/day) ÷ 6.25",
" (Protein is 16% nitrogen by weight)",
"##Nitrogen Excretion:",
" Measure Urinary Urea Nitrogen (UUN) over 24 hours",
" ~85% of urinary nitrogen is urea",
" Add 4–6 g/day for non-urinary losses (stool, skin, fistula)",
" If UUN > 30 g/24h → use 6 g for non-urinary losses",
"##Target:",
"> Positive nitrogen balance of +4 to +6 grams/day",
"! Positive nitrogen balance REQUIRES adequate nonprotein calories — not protein alone",
" Increasing protein without meeting caloric targets will NOT achieve positive N balance",
"! Nitrogen balance UNRELIABLE in the setting of diarrhea (unmeasurable enteric losses)",
"##Example: 70 kg patient, 105 g protein intake, UUN = 20 g/24h:",
" N balance = (105 ÷ 6.25) − (20 + 4) = 16.8 − 24 = −7.2 g/day (negative = catabolic)",
]);
// ══════════════════════════════════════════════════════════════════
// SECTION 5
// ══════════════════════════════════════════════════════════════════
sectionDivider("5. Enteral Nutrition — Principles,\nTiming & Access");
contentSlide("Why Enteral Nutrition is Preferred", [
"##Non-Nutritional Benefits of Enteral Feeding:",
" Preserves gut mucosal integrity (maintains villous height)",
" Prevents gut mucosal atrophy & bacterial translocation",
" Maintains gut-associated lymphoid tissue (GALT) → IgA production",
" Blocks pathogen attachment to bowel mucosa",
" Attenuates hypermetabolic stress response",
" Reduces risk of MODS (multi-organ dysfunction syndrome)",
"##Compared to PN, Enteral Nutrition:",
" Associated with fewer infections (especially pneumonias)",
" Lower cost",
" Fewer metabolic complications",
" Better long-term outcomes",
"! Parenteral nutrition does NOT prevent the deleterious effects of prolonged bowel rest",
"> Key principle: 'Feed the gut to protect the gut'",
]);
contentSlide("When to Start: Timing of Enteral Nutrition", [
"##Early EN — Start Within 24–48 Hours of ICU Admission:",
"> 'Initiate EN as soon as the patient is hemodynamically stable'",
" Early EN → fewer septic complications, shorter hospital stay",
" Benefits greatest in high-risk / malnourished patients",
"##Contraindications to Enteral Nutrition:",
"##Absolute:",
" Complete bowel obstruction",
" Bowel ischemia",
" Uncontrolled hemodynamic instability / high-dose vasopressors",
" Active GI hemorrhage",
"##Relative (proceed cautiously):",
" Patients on stable, low-dose vasopressors → attempt trophic/gastric feeds",
" Severe acute pancreatitis → start EN (small bowel access preferred)",
" Do NOT wait for bowel sounds before initiating EN",
"##Trophic / Permissive Underfeeding:",
" ≤20 mL/hr or 50 mL bolus every 4 hours",
" Used during hemodynamic instability or escalating pressors",
]);
twoColSlide("Enteral Access — Short-Term vs. Long-Term",
[
"##Short-Term Access (<4 weeks)",
"Salem Sump NG/OG tube",
" Nurse-placed; decompression + feeding",
" Risk: sinusitis, nasal necrosis",
"Nasoenteric tube (softer/flexible)",
" Less sinusitis risk; can be oral",
" Small bowel tube for poor gastric emptying",
"##Feeding Tube Placement:",
" Distance nose → earlobe → xiphoid: ~50–60 cm",
"! CXR REQUIRED to verify position before feeding",
"! Auscultation ('air bolus') is NOT reliable",
" Tracheal misplacement: ~1% of insertions",
" Intubated patients may NOT cough on tracheal misplacement",
],
[
"##Long-Term Access (>4 weeks)",
"G-tube (PEG / surgical gastrostomy)",
" Functioning GI tract + adequate gastric emptying",
" Lower aspiration risk",
"J-tube (PEJ / jejunostomy)",
" Poor gastric emptying / high reflux risk",
" Severe pancreatitis, gastric dysmotility",
"G-J tube",
" Feeds distally; gastric port for decompression",
" Placed percutaneously or at laparotomy",
"##Gastric vs. Small Bowel Feeding:",
" Gastric: most ICU patients",
" Small bowel: gastroparesis, GERD, pancreatitis, proven intolerance to gastric feeds",
" No proven aspiration reduction with post-pyloric vs. gastric (most studies)",
],
"Short-Term", "Long-Term"
);
// ══════════════════════════════════════════════════════════════════
// SECTION 6
// ══════════════════════════════════════════════════════════════════
sectionDivider("6. Enteral Feeding Formulas");
tableSlide("Enteral Formula Selection Guide",
["Clinical Scenario", "Formula Type", "Examples"],
[
["Most ICU patients", "Standard polymeric (1–1.5 kcal/mL)", "Jevity, Osmolite"],
["Volume restriction / high caloric need", "High-caloric density (2 kcal/mL)", "TwoCal HN, Nutren 2.0"],
["Malabsorption / diarrhea", "Semi-elemental (peptide-based)", "Peptamen, Vital HN, Optimental"],
["Severe malabsorption", "Elemental (free amino acids)", "Vivonex T.E.N."],
["Diabetes / hyperglycemia", "Low-carbohydrate formula", "Glucerna (30–40% carbs)"],
["Trauma / post-operative", "Immune-modulating formula", "Impact, Immune-Aid"],
["Severe acute pancreatitis", "Polymeric + small bowel access", "Standard formula, jejunal route"],
["Severe sepsis", "Standard formula (no immune mod.)", "Avoid arginine formulas"],
["ARDS", "Standard formula (fish oil not mandated)", "No specific recommendation"],
["Renal failure (no dialysis)", "Renal formula (lower K/Phos/fluid)", "Nepro, Novasource Renal"],
],
[3.8, 3.2, 3.0]
);
contentSlide("Understanding Formula Composition", [
"##Protein Types in EN Formulas:",
" Polymeric: intact proteins → digested in upper GI (standard)",
" Semi-elemental: small peptides → faster absorption, better in diarrhea",
" Elemental: free amino acids → maximal absorption, highest osmolarity",
" Clinical benefit of elemental > polymeric is UNPROVEN",
"##Standard Formula Protein Content:",
" Standard formulas: 35–40 g protein per liter",
" High-nitrogen (HN) formulas: ~42–48 g protein per liter",
" If protein target not met → add powdered protein modulars",
"##Carbohydrate Content:",
" Standard formulas: 40–70% of total calories",
" Low-carb formulas (Glucerna): 30–40% calories from carbs",
"##Fiber:",
" Soluble (fermentable): → short-chain fatty acids → gut mucosal health, reduces diarrhea",
" Insoluble: draws water into bowel → increases stool water — AVOID in critically ill",
" Soluble fiber 10–20 g/day only in fully resuscitated, hemodynamically stable patients",
"! AVOID ALL fiber in: bowel ischemia risk, severe dysmotility, first week post-GI surgery",
]);
// ══════════════════════════════════════════════════════════════════
// SECTION 7
// ══════════════════════════════════════════════════════════════════
sectionDivider("7. Parenteral Nutrition");
contentSlide("Indications & Principles of Parenteral Nutrition", [
"##When to Use TPN:",
" EN is contraindicated or not feasible",
" EN is insufficient to meet ≥60% of energy goals",
" Low-risk patients: start PN within 5–7 days if EN fails",
" High-risk / severe malnutrition: start PN as soon as possible",
"##Route of Administration:",
" Hyperosmolar solutions → MUST use central vein (CVC or PICC)",
" Preferred: subclavian line (lower infection rate, occlusive dressing easy)",
" Least preferred: femoral line (highest infection & thrombosis risk)",
"! Peripheral IV PN is NOT appropriate for critically ill patients",
"##Peripheral Parenteral Nutrition (PPN):",
" Only protein-sparing — NOT full nutritional support",
" Osmolarity MUST be <900 mosm/L",
" Standard solution: 3% amino acids + 20% dextrose (osmolarity ~500 mosm/L)",
" Provides ~1,350 kcal/day max — appropriate only for unstressed patients",
"> Final principle: 'Avoid parenteral nutrition whenever possible' (Marino, ICU Book)",
]);
contentSlide("TPN Composition — Macronutrients", [
"##Dextrose (Carbohydrate Source):",
" Standard solution: 50% dextrose (D50)",
" Caloric yield: 3.4 kcal/gram of dextrose",
" Provides ~70% of nonprotein calories in TPN",
" Standard TPN at 1,800 kcal → ~350 g glucose load",
"##Amino Acid Solutions:",
" Available as 3.5%–10% concentrations; 7% solutions (70 g/L) used most often",
" Standard mix (A10-D50): 5% amino acids + 25% dextrose per liter",
" Specialty solutions: branched-chain AAs (trauma/liver), essential AAs (renal failure)",
"! Specialty amino acid solutions have NOT been proven to improve outcomes",
"##Lipid Emulsions:",
" 10% emulsion: ~1 kcal/mL (isotonic — can infuse peripherally)",
" 20% emulsion: ~2 kcal/mL (isotonic — can infuse peripherally)",
" Max infusion rate: 50 mL/hour",
" Triglycerides take 8–10 hours to clear from bloodstream",
" Source: safflower or soybean oil — rich in linoleic acid (essential FA)",
" Provide ≥4% of daily calories as linoleic acid to prevent EFA deficiency",
]);
tableSlide("TPN Electrolyte Dosing Guide (per liter)",
["Electrolyte", "Suggested Dose", "Alter When..."],
[
["Sodium", "60–150 mEq/L", "Renal function, fluid status, GI losses, TBI"],
["Potassium", "40–120 mEq/L", "Renal function, GI losses, refeeding syndrome"],
["Phosphate", "10–30 mM/L", "Renal function, refeeding, hypercalcemia"],
["Chloride", "60–120 mEq/L", "GI losses (gastric), acid-base status"],
["Acetate", "10–40 mEq/L", "Renal failure, metabolic acidosis"],
["Calcium", "4.5–9.2 mEq/L", "Hyperparathyroidism, pancreatitis, malignancy"],
["Magnesium", "8.1–24.3 mEq/L", "Refeeding syndrome, hypokalemia"],
],
[2.5, 3.5, 3.5]
);
contentSlide("Creating a TPN Regimen — 5-Step Method (70 kg example)", [
"##Step 1: Calculate daily requirements",
" Caloric need: 70 kg × 25 kcal = 1,750 kcal/day",
" Protein need: 70 kg × 1.4 g/kg = 98 g/day",
" Subtract propofol calories if running (1.1 kcal/mL × rate)",
"##Step 2: Calculate volume of A10-D50 to meet protein needs",
" A10-D50 = 50 g protein/L; Volume = 98 g ÷ 50 g/L = 1.9 L/day",
" Infusion rate: 1.9 L ÷ 24h = ~80 mL/hr",
"##Step 3: Calculate dextrose calories from Step 2 volume",
" Dextrose: 1.9 L × 250 g/L × 3.4 kcal/g = 1,615 kcal",
"##Step 4: Add lipid to meet caloric deficit",
" Deficit: 1,750 − 1,615 = 135 kcal → 10% Intralipid 150 mL over 3 hrs",
"##Step 5: Add micronutrients and write daily orders",
" Add: standard electrolytes + multivitamins (1 MVI vial/day) + trace elements",
" Selenium 200 µg/day (especially in sepsis)",
" Rewrite TPN orders DAILY — adjust based on labs",
]);
// ══════════════════════════════════════════════════════════════════
// SECTION 8
// ══════════════════════════════════════════════════════════════════
sectionDivider("8. Monitoring & Complications");
contentSlide("Gastric Residual Volume (GRV) — Modern Approach", [
"##Traditional vs. Current Practice:",
" Old threshold: hold feeds at GRV >150–250 mL",
" Clinical reality: frequent feed interruptions → 60% of prescribed calories delivered",
" Half of patients had feeds held for GRV <200 mL (below the guideline threshold!)",
"##Current Evidence & Guidelines:",
"> Daily GRV surveillance is NO LONGER RECOMMENDED as routine practice",
" GRV does NOT correlate reliably with aspiration risk or clinical outcomes",
" GRV up to 500 mL does NOT increase aspiration pneumonia risk (Poulard et al.)",
" Not monitoring GRV → no adverse consequences on VAP or clinical outcomes",
"##If GRV is Still Used:",
" GRV 200–500 mL → raise concern but DO NOT stop feeds unless other signs of intolerance",
" GRV ≥500 mL + clinical signs (distension, vomiting) → hold; reassess",
"##Measures to Reduce Aspiration Risk:",
" Elevate head of bed to 45°",
" Prokinetic therapy (see next slide)",
" Consider post-pyloric feeding tube",
]);
contentSlide("Managing EN Complications", [
"##Prokinetic Agents for Gastroparesis / High GRV:",
" Erythromycin 200 mg IV q12h → ↓GRV by 60% at 24h (motilin receptor agonist)",
" Metoclopramide 10 mg IV q6h → ↓GRV by 30% (dopamine antagonist; max 72 hrs)",
" Enteral Naloxone 8 mg via NGT q6h → opioid-induced gastroparesis (no systemic reversal)",
" Combination (erythromycin + metoclopramide) is more effective than either alone",
"##Diarrhea (~30% of patients on EN):",
"! Principal offender: LIQUID DRUG PREPARATIONS — not the feeding formula",
" Sorbitol in liquid medications → osmotic diarrhea",
" C. difficile — always rule out",
" Soluble fiber 10–20 g/day if fully resuscitated",
" Loperamide 2–4 mg q6h for symptomatic treatment",
"> KEEP FEEDING — do not stop EN for diarrhea without cause",
"##Tube Occlusion:",
" Flush with 30 mL water q4h + 10 mL after medications",
" If occluded: Viokase (pancreatic enzyme) + sodium carbonate tablet in 5 mL water → clamp 5 min → warm water flush (75% success rate)",
]);
contentSlide("TPN Complications — Metabolic", [
"##Hyperglycemia (Most Common):",
" Blood glucose >300 mg/dL in 20% of post-op patients on TPN",
" Standard TPN (1,800 kcal) delivers ~350 g glucose vs. 230 g in standard EN",
"! Tight glycemic control (80–110) → NOT recommended → hypoglycemia risk",
"> Target blood glucose: 140–180 mg/dL (ACCM/SCCM guidelines)",
" Insulin: continuous IV infusion of regular insulin (preferred for type 1 DM / unstable)",
" Can add insulin directly to TPN bags; prime tubing with 20 mL of 1 unit/mL solution",
"##Hypophosphatemia:",
" Glucose uptake → intracellular phosphate shift → most common cause in hospitalized patients",
" Plasma phosphate falls steadily after TPN initiation → monitor closely",
"##Hypokalemia:",
" Glucose loading → intracellular K⁺ shift — transient but can persist",
"##Hypercapnia:",
" Excessive carbohydrate/caloric intake → ↑CO₂ production → respiratory failure in ventilator-dependent patients",
" RQ > 1.0 signals overfeeding",
]);
contentSlide("TPN Complications — Organ / Infectious", [
"##Hepatic Steatosis:",
" Fat accumulation in liver — common in long-term TPN",
" Caused by chronic carbohydrate and lipid overfeeding",
" Associated with elevated liver enzymes (AST, ALT, GGT)",
"##Cholestasis / Acalculous Cholecystitis:",
" Absence of lipids in proximal small bowel → no CCK release → gallbladder stasis",
" Bile sludge → acalculous cholecystitis",
" Provide minimal EN alongside TPN whenever possible to prevent this",
"##Bowel Sepsis / Bacterial Translocation:",
" Absence of luminal nutrition → bowel mucosal atrophy → gut barrier failure",
" Systemic spread of enteric pathogens → MODS",
"##Lipid-Associated Lung Injury:",
" TPN lipid emulsions are rich in oxidizable lipids",
" Infusion of oleic acid = standard model for ARDS in animals",
" Lipid infusions can impair oxygenation → monitor pulmonary function",
"##Catheter-Related Bloodstream Infection (CLABSI):",
" Dedicated TPN port on CVC — strict aseptic technique mandatory",
" No new catheter required if designated port available and no bacteremia signs",
]);
// ══════════════════════════════════════════════════════════════════
// SECTION 9
// ══════════════════════════════════════════════════════════════════
sectionDivider("9. Special Populations");
tableSlide("Nutrition in Special ICU Populations",
["Population", "Caloric Target", "Protein Target", "Key Considerations"],
[
["Obese (BMI 30–50)", "11–14 kcal/kg ABW", "2.0–2.5 g/kg IBW", "Hypocaloric + high-protein strategy"],
["Morbidly Obese (BMI >50)", "22–25 kcal/kg IBW", "2.5 g/kg IBW", "IBW for all calculations"],
["AKI — No RRT", "25–30 kcal/kg", "1.0–1.5 g/kg", "Restrict to avoid azotemia if no RRT"],
["AKI — CRRT", "25–30 kcal/kg", "2.0–2.5 g/kg", "CRRT loses amino acids; increase protein"],
["TBI", "25–30 kcal/kg", "1.5–2.5 g/kg", "High protein; sodium management critical"],
["Burns", "25–35 kcal/kg", "1.5–2.0 g/kg", "Hypermetabolic; rapid phosphate turnover"],
["Open Abdomen", "25–30 kcal/kg", "1.5–2.0 + 15 g/L exudate", "Protein losses via exudate; replace aggressively"],
["Liver Failure", "25–30 kcal/kg dry wt", "1.2–2.0 g/kg dry wt", "Do NOT restrict protein — worsens outcomes"],
["Severe Pancreatitis", "25–30 kcal/kg", "1.2–2.0 g/kg", "EN via nasojejunal tube preferred; start early"],
["On Pressors (stable)", "Trophic (≤20 mL/hr)", "Start when tolerating", "Escalating pressors → hold EN; reassess daily"],
],
[2.5, 2.5, 2.5, 2.5]
);
// ══════════════════════════════════════════════════════════════════
// SECTION 10
// ══════════════════════════════════════════════════════════════════
sectionDivider("10. Immunonutrition &\nConditionally Essential Nutrients");
contentSlide("Glutamine — Benefits, Risks & Current Evidence", [
"##Why Glutamine Matters:",
" Principal metabolic fuel for rapidly dividing cells (intestinal epithelium, endothelium)",
" Critical for bowel mucosal integrity and barrier function",
" Supports GALT immune function and IgA production",
" Conditionally essential — becomes depleted during critical illness",
"##Historical Recommendation:",
" EN: 0.2–0.4 g/kg/day as supplement",
" TPN: must be pharmacy-added (not in commercial amino acid solutions)",
"##CRITICAL UPDATE — REDOX Trial (Heyland et al., NEJM 2013):",
"! Glutamine supplementation → INCREASED MORTALITY in ICU patients with multi-organ failure",
"! Current recommendation: DO NOT give high-dose IV glutamine to patients with MOF",
" Enteral glutamine in burns and trauma may still be considered",
" Evidence in these subgroups is more favorable",
"> Bottom line: Patient selection is critical — avoid in hemodynamically unstable patients with MOF",
]);
contentSlide("Arginine, Omega-3 Fatty Acids & Antioxidants", [
"##Arginine:",
" Preferred substrate for injured muscle; promotes wound healing",
" Precursor of nitric oxide; stimulates T-cell function",
" Present in immune-modulating formulas at 8–19 g/L",
"! CONTRAINDICATED in severe sepsis — arginine → nitric oxide → vasodilation → worsened hypotension",
" Benefit shown in post-operative, elective surgical, and trauma patients",
"##Omega-3 Fatty Acids (Fish Oil):",
" Anti-inflammatory (do not serve as precursors for pro-inflammatory eicosanoids)",
" Benefit in trauma and post-operative patients",
" NOT mandated for ARDS or severe ALI (evidence insufficient)",
" Standard vegetable-oil-based formulas can promote inflammation via omega-6 pathway",
"##Antioxidants (Vitamin E, Vitamin C, Selenium, Zinc):",
" Benefit in trauma and post-operative patients when given in combination",
" Selenium 200 µg/day → associated with lower mortality in severe sepsis",
" NOT routinely mandated for ARDS or general medical ICU",
"##Probiotics:",
" No recommendation for general ICU use (inconsistent outcomes, strain heterogeneity)",
]);
contentSlide("Vitamins & Trace Elements in the ICU", [
"##Vitamins — Key ICU Points:",
" 13 vitamins considered essential",
" ICU requirements likely HIGHER than standard RDA (unknown exactly)",
" Deficiencies common even with standard supplementation",
" Add 1 MVI vial/day to TPN; adjust for specific deficiencies",
"##Thiamine (Vitamin B1) — Critical:",
" Co-enzyme for pyruvate dehydrogenase → cellular energy production",
" Deficiency: Wernicke's encephalopathy, lactic acidosis, wet beriberi (cardiomyopathy), peripheral neuropathy",
" Risk factors: alcoholism, furosemide use, hypermetabolism, Mg depletion",
"! Thiamine is DESTROYED by sulfites in TPN bags — add as separate MVI, NOT mixed directly",
" Functional test: erythrocyte transketolase assay (>25% increase with TPP = deficient)",
"##Selenium — Most Important Trace Element:",
" Co-factor for glutathione peroxidase (key antioxidant enzyme)",
" Plasma selenium reduced in severe sepsis",
"> Recommended: 200 µg/day; safe up to 400 µg/day",
" Normal trace element mixtures often lack selenium — add separately in sepsis",
"! Iron supplementation NOT advised in critically ill — free iron promotes hydroxyl radical formation",
]);
// ══════════════════════════════════════════════════════════════════
// SECTION 11
// ══════════════════════════════════════════════════════════════════
sectionDivider("11. Glucose Management\nin the ICU");
contentSlide("Glucose Control — The Evidence & Current Targets", [
"##Why Glucose Management Is Critical in ICU Nutrition:",
" Hyperglycemia → impaired neutrophil function → increased nosocomial infection",
" Hyperglycemia universal in critically ill due to insulin resistance and glucose loading from TPN/EN",
"##Historical Background:",
" Van den Berghe 2001 (surgical ICU): tight control (80–110 mg/dL) → 50% mortality reduction",
" Follow-up studies (NICE-SUGAR trial, 2009): tight control → INCREASED mortality",
" Hypoglycemia (≤40 mg/dL) more dangerous than moderate hyperglycemia",
"##Current Target:",
"> Blood glucose: 140–180 mg/dL (ACCM/SCCM & ASPEN/SCCM guidelines)",
"! Tight glycemic control (80–110 mg/dL) is NOT recommended — risk of fatal hypoglycemia",
"##Management Strategy:",
" Continuous IV regular insulin infusion for type 1 DM or unstable patients",
" Can add insulin directly to TPN bags (prime tubing first)",
" Permissive underfeeding (50–75% of target) → easier glucose control",
" Reduce glucose load from TPN by limiting dextrose concentration",
" Propofol calories must be counted (1.1 kcal/mL) to avoid inadvertent overfeeding",
]);
// ══════════════════════════════════════════════════════════════════
// SECTION 12
// ══════════════════════════════════════════════════════════════════
sectionDivider("12. Refeeding Syndrome");
contentSlide("Refeeding Syndrome — Recognition & Management", [
"##Definition:",
" Life-threatening electrolyte shifts upon reintroduction of nutrition in severely malnourished patients",
"##Mechanism:",
" Glucose infusion → insulin surge → intracellular shift of P, K, Mg",
" Simultaneously: thiamine rapidly consumed by glucose metabolism",
" Results in severe hypophosphatemia, hypokalemia, hypomagnesemia",
"##High-Risk Patients:",
" >30% below ideal body weight",
" Minimal or no oral intake for >5–10 days",
" Chronic alcoholism, malabsorption syndromes, anorexia nervosa",
" BMI <16 kg/m² or weight loss >15% in prior 3–6 months",
"##Clinical Manifestations:",
" Cardiac arrhythmias, heart failure (from hypophosphatemia)",
" Respiratory failure (from phosphate depletion of diaphragm)",
" Encephalopathy, seizures (thiamine deficiency + hypomagnesemia)",
"##Management Protocol:",
" Electrolytes BEFORE and DURING refeeding: baseline P, K, Mg, Ca",
" Supplement deficiencies before starting nutrition",
" Start at 25–50% of caloric goal → advance slowly over 5–7 days",
" Thiamine 100–300 mg IV × 3 days before and during refeeding",
" Monitor electrolytes daily for first 2 weeks",
]);
// ══════════════════════════════════════════════════════════════════
// SECTION 13
// ══════════════════════════════════════════════════════════════════
sectionDivider("13. Key Protocols &\nTake-Home Points");
contentSlide("Enteral Feeding Protocol — 4-Step Approach", [
"##Step 1: Calculate Requirements",
" Energy: 25 kcal/kg/day (adjust for BMI; subtract propofol if running)",
" Protein: 1.2–2.0 g/kg/day (adjust per clinical condition)",
" Use actual BW unless >125% IBW (then use adjusted BW)",
"##Step 2: Select Formula",
" Standard polymeric 1–1.5 kcal/mL for most patients",
" 2 kcal/mL if volume restriction needed",
" Elemental/semi-elemental for malabsorption",
"##Step 3: Calculate Infusion Rate",
" Volume (mL/day) = Caloric target ÷ Caloric density",
" Rate (mL/hr) = Volume ÷ Hours of feeding",
" Nonprotein calories = 85% of total calories (standard formulas)",
"##Step 4: Adjust Protein",
" Check: Formula volume × g protein/L = daily protein delivered",
" If insufficient → add powdered protein modulars to tube feeds",
"##Initiation:",
" Start at target rate immediately (current evidence — no need for slow ramp-up for gastric feeds)",
" Slow advancement reserved for small bowel/jejunal feeds",
]);
tableSlide("Quick Reference: Key Numbers in ICU Nutrition",
["Parameter", "Value", "Source / Notes"],
[
["Energy target (normal BMI)", "25–30 kcal/kg/day", "All 3 references"],
["Protein target (general ICU)", "1.2–2.0 g/kg/day", "Washington Manual / Irwin & Rippe"],
["Protein target (TBI)", "1.5–2.5 g/kg/day", "Washington Manual"],
["Protein target (CRRT)", "2.0–2.5 g/kg/day", "Washington Manual"],
["Glucose target (ICU)", "140–180 mg/dL", "ACCM/SCCM guidelines"],
["EN start timing", "Within 24–48 hours", "ASPEN/SCCM 2016"],
["GRV threshold (if monitored)", "≥500 mL + clinical signs", "Current guidelines"],
["Propofol calories", "1.1 kcal/mL", "Marino ICU Book"],
["Dextrose energy yield (TPN)", "3.4 kcal/g", "Marino ICU Book"],
["Selenium dose (sepsis)", "200 µg/day", "Marino / Irwin & Rippe"],
["Nitrogen balance target", "+4 to +6 g/day", "Marino ICU Book"],
["Erythromycin (prokinetic)", "200 mg IV q12h", "Marino ICU Book"],
["Metoclopramide (prokinetic)", "10 mg IV q6h (max 72h)", "Washington Manual"],
["Trophic feed rate", "≤20 mL/hr or 50 mL q4h bolus", "Washington Manual"],
["PPN osmolarity limit", "<900 mosm/L", "Marino ICU Book"],
],
[4, 3.2, 2.3]
);
contentSlide("The 10 Commandments of ICU Nutrition", [
"##1. Assess nutrition risk on admission (NRS-2002 or NUTRIC score)",
"##2. Start enteral nutrition within 24–48 hours — do not wait for bowel sounds",
"##3. Prefer enteral over parenteral — 'Feed the gut to protect the gut'",
"##4. Target 25–30 kcal/kg/day adjusted for BMI; use indirect calorimetry if available",
"##5. Prioritize protein — 1.2–2.0 g/kg/day is more important than calories",
"##6. Monitor and target blood glucose 140–180 mg/dL — tight control is HARMFUL",
"##7. Do NOT use albumin/prealbumin to assess nutritional status in ICU",
"##8. Count all caloric sources — especially propofol (1.1 kcal/mL)",
"##9. Screen for and prevent refeeding syndrome in malnourished patients",
"##10. Reassess and adjust nutrition plan DAILY — critically ill patients are dynamic",
], {fs:14});
// ══════════════════════════════════════════════════════════════════
// CLOSING SLIDE
// ══════════════════════════════════════════════════════════════════
{
const s = pres.addSlide();
s.addShape(pres.ShapeType.rect, { x:0, y:0, w:10, h:5.625, fill:{color:C.navy} });
s.addShape(pres.ShapeType.rect, { x:0, y:1.4, w:10, h:0.12, fill:{color:C.teal} });
s.addShape(pres.ShapeType.rect, { x:0, y:1.52, w:10, h:0.05, fill:{color:C.gold} });
s.addText("References", { x:0.5, y:0.3, w:9, h:0.9, fontSize:28, bold:true, color:C.white, align:"center", fontFace:"Calibri" });
s.addText([
{ text: "1. Marino PL. ", options:{bold:true, color:C.ltgray} },
{ text: "The ICU Book, 4th Edition. ", options:{italic:true, color:C.ltgray} },
{ text: "Wolters Kluwer, 2014. Chapters 47–49 (Nutritional Requirements, Enteral Tube Feeding, Parenteral Nutrition).\n\n", options:{color:C.ltgray} },
{ text: "2. Taylor BE, Dean JS. ", options:{bold:true, color:C.ltgray} },
{ text: "Chapter 73: Nutrition in the ICU. In: ", options:{italic:true, color:C.ltgray} },
{ text: "Washington Manual of Critical Care, 3rd Ed.", options:{italic:true, color:C.ltgray} },
{ text: " Wolters Kluwer, 2016.\n\n", options:{color:C.ltgray} },
{ text: "3. Bistrian BR, McCowen KC. ", options:{bold:true, color:C.ltgray} },
{ text: "Nutritional and Metabolic Support in the Adult ICU. In: Irwin & Rippe's Intensive Care Medicine, 9th Ed.", options:{italic:true, color:C.ltgray} },
{ text: " Wolters Kluwer, 2022.\n\n", options:{color:C.ltgray} },
{ text: "4. McClave SA et al. ", options:{bold:true, color:C.ltgray} },
{ text: "SCCM/ASPEN Guidelines for Provision and Assessment of Nutrition Support Therapy in the Adult Critically Ill Patient. ", options:{italic:true, color:C.ltgray} },
{ text: "JPEN 2016;40:159–211.\n\n", options:{color:C.ltgray} },
{ text: "5. Heyland D et al. ", options:{bold:true, color:C.ltgray} },
{ text: "A Randomized Trial of Glutamine and Antioxidants in Critically Ill Patients (REDOX). ", options:{italic:true, color:C.ltgray} },
{ text: "NEJM 2013;368:1489–1497.", options:{color:C.ltgray} },
], { x:0.5, y:1.75, w:9, h:3.6, fontSize:12, fontFace:"Calibri", valign:"top", lineSpacingMultiple:1.3 });
}
// ── WRITE FILE ──────────────────────────────────────────────────
pres.writeFile({ fileName: "/home/daytona/workspace/icu-nutrition-ppt/Nutrition_in_ICU.pptx" })
.then(() => console.log("SUCCESS: Nutrition_in_ICU.pptx created"))
.catch(e => { console.error("ERROR:", e); process.exit(1); });
cd /home/daytona/workspace/icu-nutrition-ppt && node nutrition_icu.js 2>&1
ls -lh /home/daytona/workspace/icu-nutrition-ppt/Nutrition_in_ICU.pptx
Nutrition in ICU
Presentation · PPTX
| Section | Slides |
|---|---|
| Title + Outline | 2 |
| Metabolic Response to Critical Illness | 2 |
| Nutrition Risk Assessment (NRS-2002, NUTRIC) | 2 |
| Energy Requirements & Caloric Targets | 3 |
| Protein Requirements + Nitrogen Balance | 3 |
| Enteral Nutrition — Timing, Access, Complications | 4 |
| Enteral Formulas & Selection Guide | 2 |
| Parenteral Nutrition — Composition, TPN Protocol | 3 |
| Monitoring & Complications (GRV, prokinetics, metabolic) | 3 |
| Special Populations (table) | 1 |
| Immunonutrition (glutamine/arginine/omega-3/selenium) | 2 |
| Glucose Management | 1 |
| Refeeding Syndrome | 1 |
| Key Numbers Table + "10 Commandments" + References | 3 |
Can you expand this ppt a little more please
~/icu-nutrition-ppt/nutrition_icu.js
Successfully replaced 1 instance(s) of the string in '/home/daytona/workspace/icu-nutrition-ppt/nutrition_icu.js'
cd /home/daytona/workspace/icu-nutrition-ppt && node nutrition_icu.js 2>&1
ls -lh /home/daytona/workspace/icu-nutrition-ppt/Nutrition_in_ICU.pptx
Nutrition in ICU
Presentation · PPTX
| New Section | Slides Added |
|---|---|
| A. Indirect Calorimetry Deep Dive | Weir equation, RQ interpretation, limitations |
| B. Overfeeding vs. Underfeeding | Side-by-side consequences + permissive underfeeding evidence (EDEN trial, CALORIES trial) |
| C. Nutrition-Focused Physical Exam | Muscle wasting signs, micronutrient deficiency signs, ICUAW, diaphragm ultrasound |
| D. Micronutrients — Comprehensive | Full vitamins table (B1–K, A, D, E) + full trace elements table (Se, Zn, Cu, Mn, Fe, Cr, I, Mo) |
| E. Practical EN Protocols | Volume-based feeding (PEP uP protocol), starter regimens, medication via tube |
| F. Condition-Specific Nutrition | Pancreatitis, post-surgery/trauma, ARDS/prone ventilation, liver failure, AKI/CRRT (5 slides) |
| G. Monitoring Framework | Full monitoring table (13 parameters with frequency + targets) + dietitian's role in ICU |
| H. Transition & Recovery Nutrition | Swallowing assessment, oral reintroduction, post-ICU rehabilitation, discharge planning |
| Expanded Quick Reference Table | 19-row comprehensive numbers table (updated) |
Did you make expanded ppt
Nutrition in ICU
Presentation · PPTX
| # | New Content Added |
|---|---|
| A | Indirect Calorimetry deep dive (Weir equation, RQ, limitations) |
| B | Overfeeding vs. Underfeeding comparison + permissive underfeeding evidence |
| C | Nutrition-focused physical examination (muscle wasting, micronutrient signs) |
| D | Full vitamin table (B1→K, A, D, E) + full trace element table (Se, Zn, Cu, Fe, Mn, Cr, I) |
| E | Volume-based feeding protocols (PEP uP), tube medication safety |
| F | Condition-specific nutrition — pancreatitis, trauma/surgery, ARDS/prone, liver failure, AKI/CRRT |
| G | Monitoring framework table (13 parameters) + role of ICU dietitian |
| H | Transition to oral feeding, swallowing assessment, post-ICU rehabilitation |
Make a comparison poster (EN vs. PN flowchart)
A professional clinical reference poster titled "Enteral Nutrition vs. Parenteral Nutrition in the ICU" with a decision flowchart and side-by-side comparison. Academic medical style, navy blue and teal color scheme with gold accents on white background. Layout: TOP SECTION - Bold title bar: "ENTERAL vs. PARENTERAL NUTRITION IN THE ICU" Subtitle: "Evidence-Based Decision Guide | ASPEN/SCCM 2016 Guidelines" MIDDLE SECTION - FLOWCHART (center of poster): Start box (gold): "Patient unable to maintain adequate oral intake?" ↓ YES arrow Diamond decision box (navy): "Is the GI tract functional and accessible?" Two branches: → LEFT branch (YES → green): "ENTERAL NUTRITION (EN) — PREFERRED ROUTE" → RIGHT branch (NO → red): "Consider PARENTERAL NUTRITION (PN)" Under EN (left column, teal background): • Start within 24–48 hours of ICU admission • Nasogastric / Nasojejunal tube • Standard polymeric formula 1–1.5 kcal/mL • HOB elevation 30–45° • Target: 25–30 kcal/kg/day • Protein: 1.2–2.0 g/kg/day • Monitor GRV (threshold ≥500 mL) CONTRAINDICATIONS box (red): Bowel obstruction | Bowel ischemia | Uncontrolled shock | Active GI bleed Under PN (right column, navy background white text): • Low-risk: start PN if EN fails at day 5–7 • High-risk / malnourished: start PN sooner • Central venous access required (CVC/PICC) • Peripheral PN only if osmolarity <900 mosm/L • Target: 25–30 kcal/kg/day • Protein: 1.2–2.0 g/kg/day • Monitor glucose, LFTs, triglycerides, electrolytes daily CAUTION box (orange): Hyperglycemia | CLABSI | Hepatic steatosis | Bowel atrophy BOTTOM SECTION - Side-by-side comparison table with 6 rows: Headers: FEATURE | ENTERAL NUTRITION | PARENTERAL NUTRITION Rows: Cost | Lower | Higher Infection risk | Lower | Higher (CLABSI) Gut protection | Yes — preserves mucosa | No — gut atrophy Time to goal | Slower (hours–days) | Fast (<24 hours) Preferred in | Most ICU patients | EN contraindicated / insufficient Key complication | Aspiration / diarrhea | Hyperglycemia / sepsis Footer: "References: Marino's ICU Book 4e • Washington Manual of Critical Care • Irwin & Rippe's ICM 9e" Clean, clinical, professional poster design suitable for ICU ward display. Clear readable fonts, good contrast, well-organized layout.
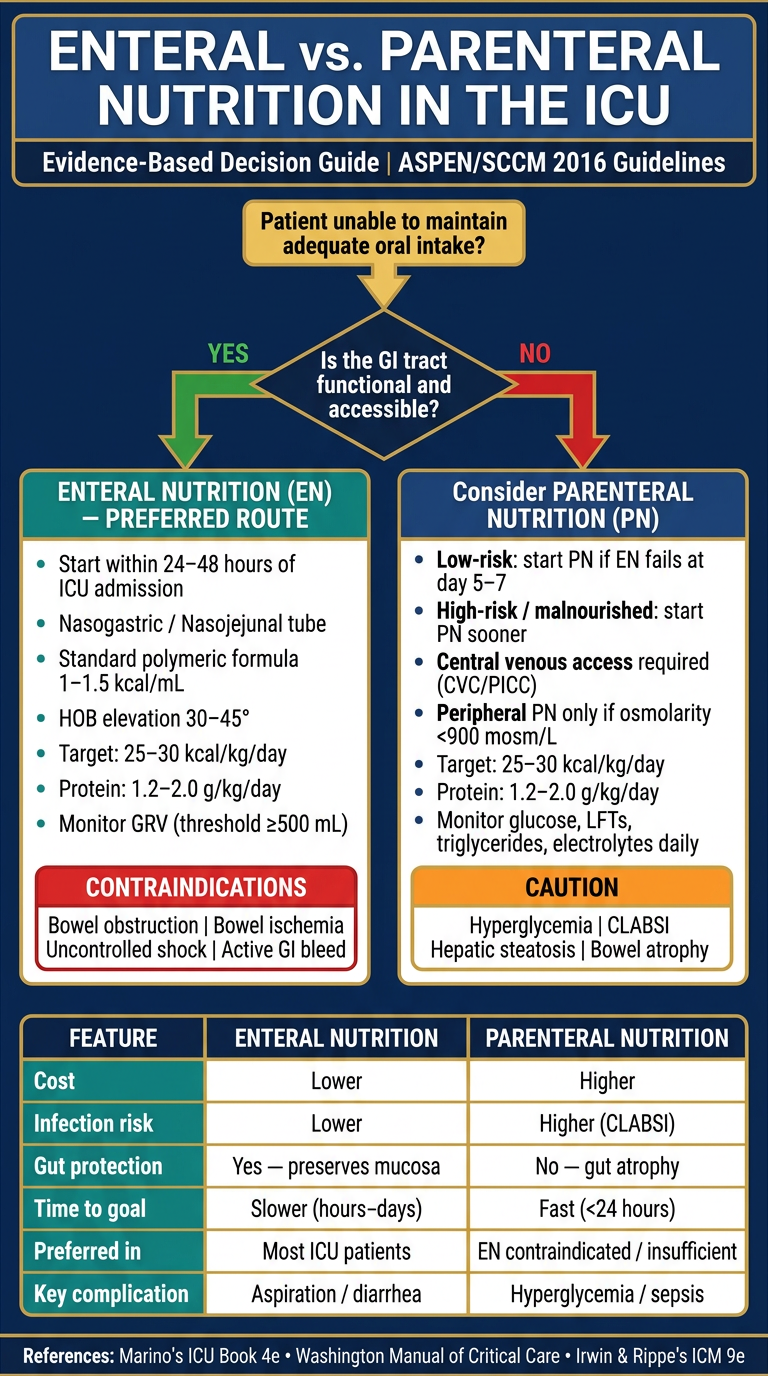
- Decision flowchart at the top — starts with GI tract assessment and branches to EN or PN
- EN column (teal) — timing, route, formula, targets, and absolute contraindications
- PN column (navy) — when to start, access requirements, targets, and key cautions
- Side-by-side comparison table at the bottom covering cost, infection risk, gut protection, time to goal, indications, and key complications
- Reference footer from all 3 of your textbooks