Pain pathways
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have all the content I need. Let me compile a comprehensive, well-organized response.
Pain Pathways
Pain is conducted from the periphery to conscious perception via a three-neuron chain. The process involves four sequential steps: transduction, transmission, modulation, and perception.
1. Overview: Nociception vs. Pain
Nociception is the neural process of encoding and processing noxious stimuli that can potentially damage tissue. Pain is the subjective, personal translation of those signals - always shaped by biological, psychological, and social factors. Pain and nociception are not synonymous; pain cannot be inferred solely from nociceptor activity. - Barash Clinical Anesthesia, 9e
2. Peripheral Nociceptors and Transduction
Tissue injury triggers release of histamine, bradykinin, prostaglandins, serotonin, and nerve growth factor. These mediators activate and sensitize peripheral nociceptors - free nerve endings that detect noxious mechanical, thermal, and chemical stimuli. There are two primary types of afferent fibers:
| Fiber | Myelination | Diameter | Conduction Velocity | Pain Quality |
|---|---|---|---|---|
| Aδ | Thinly myelinated | 2-5 µm | 5-30 m/s | Sharp, localized, "first pain" |
| C | Unmyelinated | 0.2-1.5 µm | 0.5-2 m/s | Dull, burning, aching, "second pain" |
Aβ fibers (large, heavily myelinated) carry non-noxious touch and can modulate pain via gating mechanisms.
Nociceptors also release substance P and calcitonin gene-related peptide (CGRP) in the periphery, triggering neurogenic inflammation (vasodilation, plasma extravasation). - Miller's Anesthesia, 10e
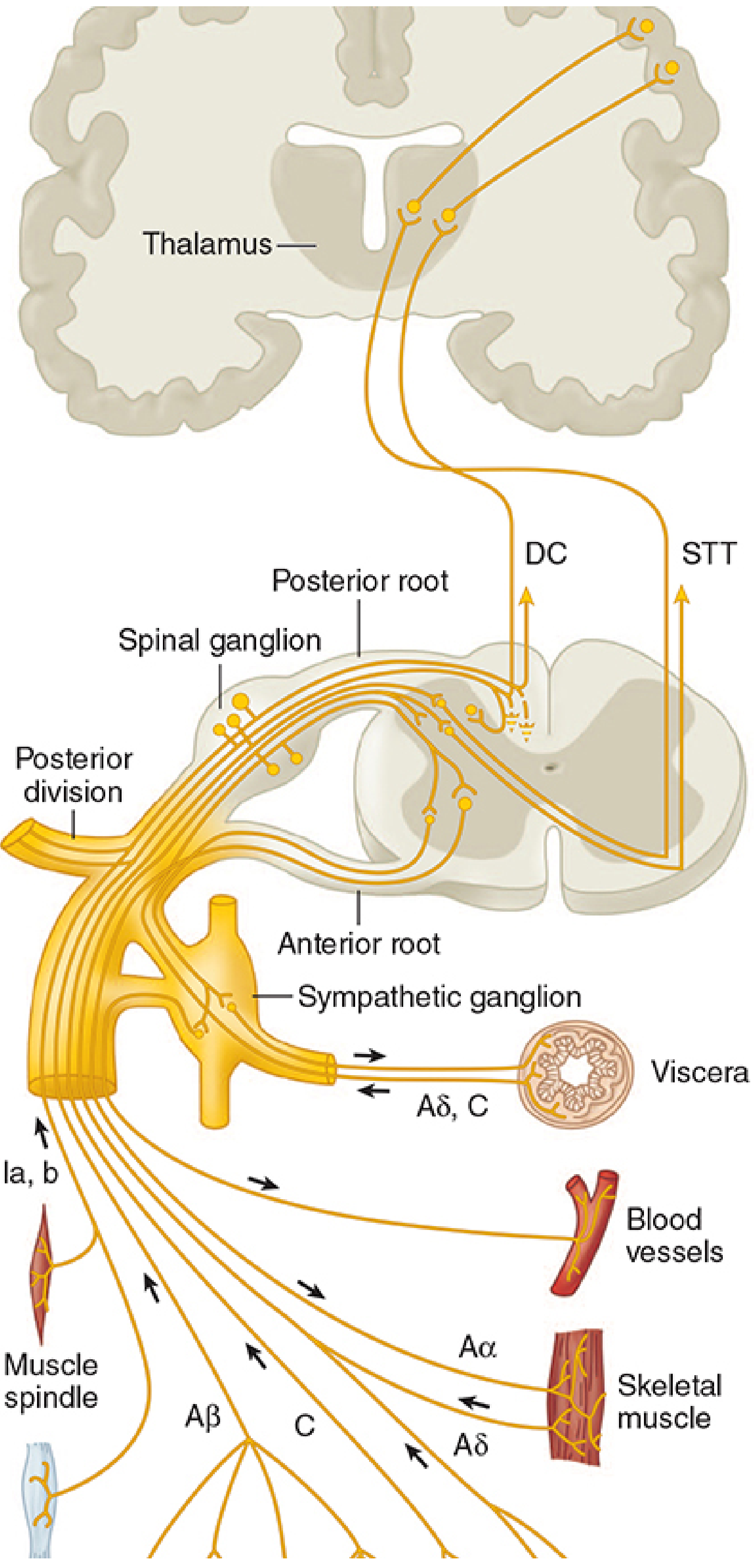
3. First-Order Neurons: Dorsal Root Ganglion to Dorsal Horn
Cell bodies of primary afferent neurons lie in the dorsal root ganglia (DRG) at each spinal level. The peripheral axon innervates tissues; the central axon enters the spinal cord via the dorsal root.
- Pain fibers enter laterally and may ascend or descend 1-3 segments in Lissauer's tract before synapsing.
- Fibers from the head travel via cranial nerves V (trigeminal), VII, IX, and X to brainstem nuclei.
Dorsal Horn - Rexed Laminae (the first processing station):
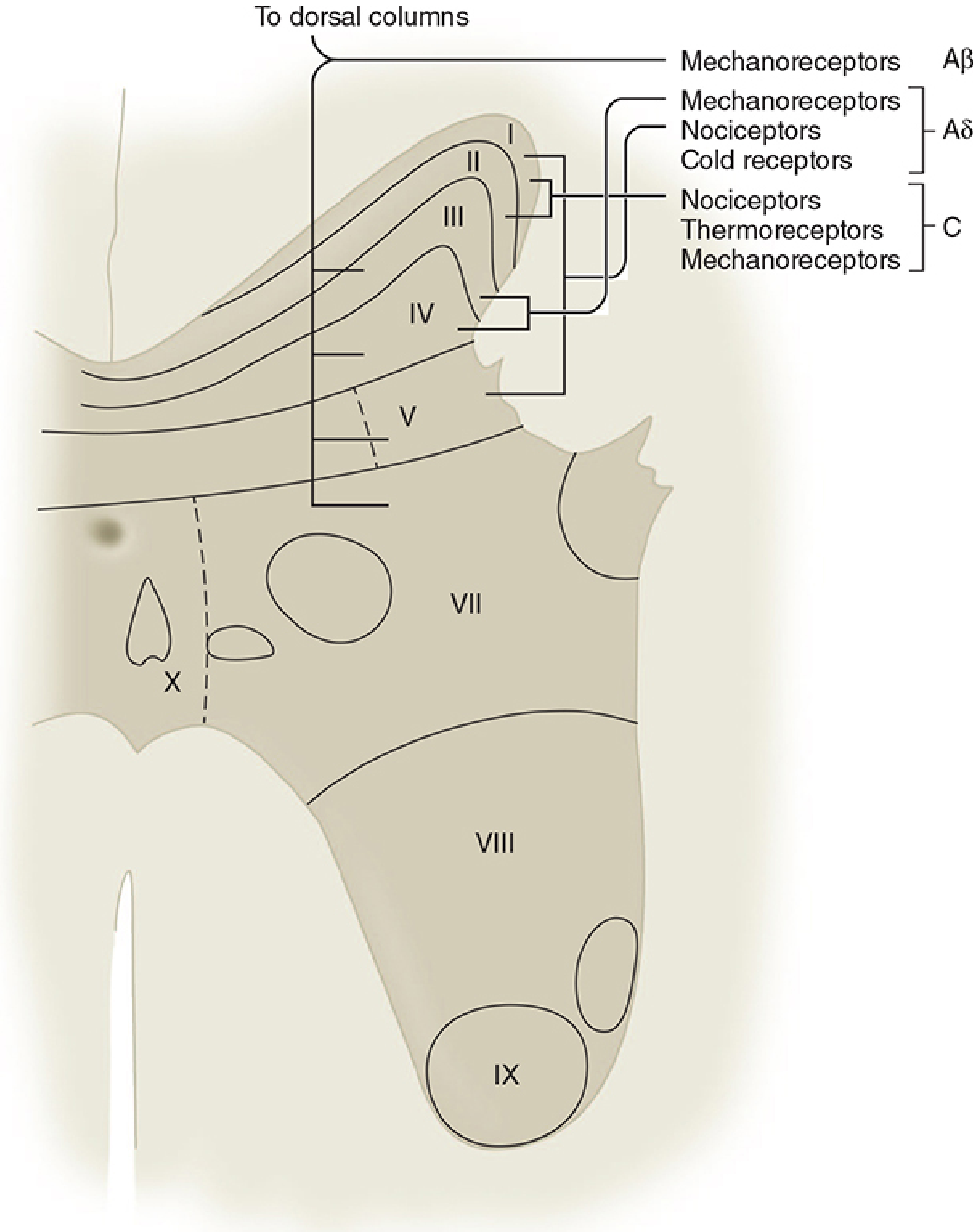
| Lamina | Name | Key Inputs | Function |
|---|---|---|---|
| I | Marginal layer | Aδ, C | Somatic nociception, thermoreception |
| II | Substantia gelatinosa | C, Aδ | Modulation of nociceptive input; major opioid action site |
| III-IV | Nucleus proprius | Aβ, Aδ | Non-nociceptive mechanoreception |
| V | Nucleus proprius (WDR) | Aβ, Aδ, C | Visceral and somatic nociception; referred pain convergence |
| VII | Intermediolateral column | - | Preganglionic sympathetic neurons |
Two types of second-order neurons exist in the dorsal horn:
- Nociceptive-specific (NS) neurons - respond only to noxious stimuli; found mainly in lamina I; somatotopically organized.
- Wide dynamic range (WDR) neurons - respond to noxious AND non-noxious input from Aβ, Aδ, and C fibers; most abundant in lamina V; exhibit wind-up (exponentially increasing firing with repeated stimulation). - Morgan & Mikhail's Clinical Anesthesiology, 7e
Visceral afferents converge on laminae I and V alongside somatic fibers - the anatomical basis of referred pain (e.g., cardiac pain felt in the left arm).
4. Second-Order Neurons: Ascending Tracts
The Anterolateral System consists of three main tracts:
A. Spinothalamic Tract (STT) - the dominant pain pathway
- Second-order axons cross the midline at the anterior commissure (taking 2-3 segments to decussate) and ascend in the contralateral anterolateral white matter.
- Somatotopic organization: sacral fibers are most lateral, cervical fibers most medial. This is why an expanding lateral cord lesion affects contralateral pain starting several segments below the lesion.
- The STT relays in the ventral posterior lateral (VPL) nucleus of the thalamus, then projects via thalamic radiations to the primary somatosensory cortex (postcentral gyrus, areas 3, 1, 2).
- Mediates discriminative aspects of pain: location and intensity.
B. Spinoreticular Tract
- Terminates on the medullary-pontine reticular formation, then projects to intralaminar thalamic nuclei (centromedian nucleus).
- Projects diffusely to the cortex (no somatotopy).
- Mediates the emotional and arousal aspects of pain ("suffering") - phylogenetically older pathway.
C. Spinomesencephalic Tract
-
Terminates in the periaqueductal gray (PAG) and midbrain reticular formation.
-
Important for descending pain modulation and behavioral responses.
-
Neuroanatomy through Clinical Cases, 3e
5. Trigeminal Pain Pathway (Face and Head)
Small-diameter fibers in the trigeminal nerve (CN V) synapse in the spinal trigeminal nucleus of the brainstem (an extension of the dorsal horn substantia gelatinosa). Second-order axons cross the midline and ascend to the thalamus via the trigeminal lemniscus (trigeminothalamic tract). The pathway is otherwise analogous to the spinal STT. - Neuroscience: Exploring the Brain, 5e
6. Thalamus and Cortex (Perception)
Nociceptive axons from the STT synapse in the VP (ventral posterior) nucleus AND the intralaminar nuclei of the thalamus - a wider territory than the touch pathway.
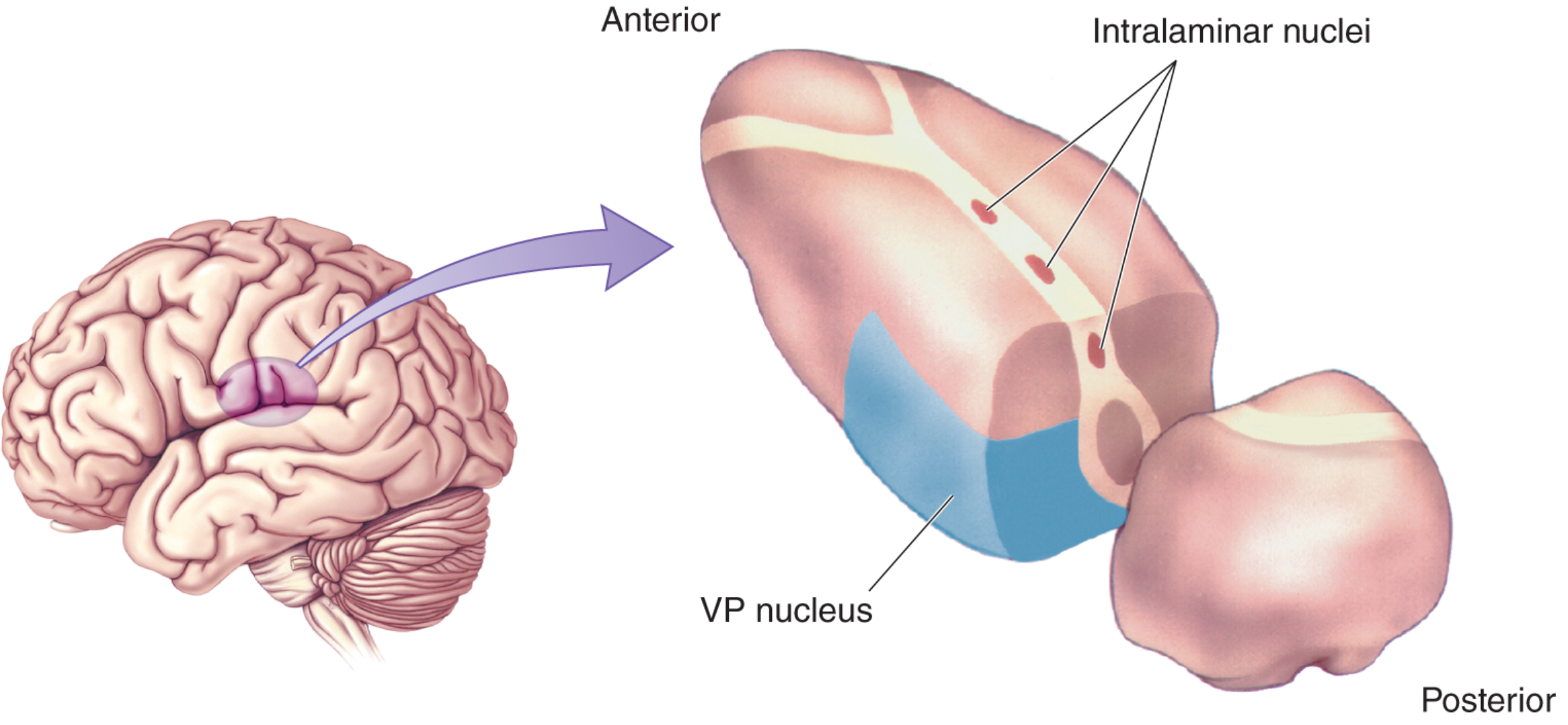
From the thalamus, pain projects to:
- Primary somatosensory cortex (S1) - the sensory-discriminative aspect (location, quality, intensity)
- Anterior cingulate cortex and insular cortex - the affective-motivational aspect (unpleasantness, suffering)
- Prefrontal cortex - the cognitive-evaluative aspect
7. Spinal Cord Integration and Segmental Reflexes
Some nociceptive impulses travel to ventral and ventrolateral horns and initiate segmental reflex responses:
- Increased skeletal muscle tone
- Inhibition of phrenic nerve function (splinting)
- Decreased gastrointestinal motility
These reflexes can persist even under anesthesia and do not require supraspinal involvement. - Miller's Anesthesia, 10e
8. Gate Control Theory (Spinal Modulation)
Proposed by Melzack and Wall (1965): the firing of STT projection neurons in the dorsal horn is determined by the balance of input from large (Aβ) and small (C) fibers.
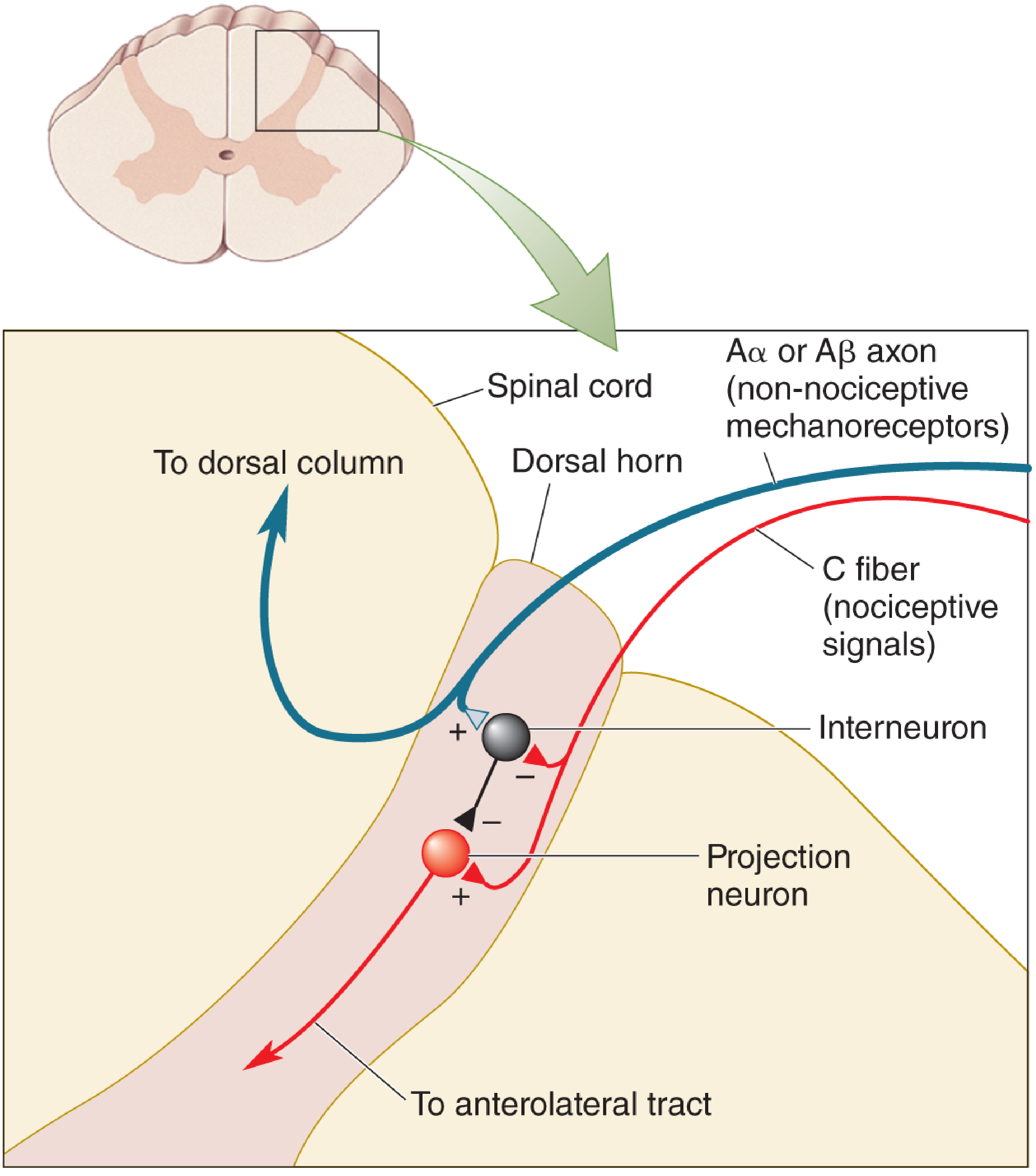
- When Aβ fibers fire (non-noxious touch): inhibitory interneurons are activated → "gate closes" → reduced pain transmission.
- When C fibers dominate: inhibitory interneurons are suppressed → "gate opens" → pain signals pass through.
- This is the rationale for TENS therapy and explains why rubbing a bruise provides relief. - Neuroscience: Exploring the Brain, 5e
9. Descending Modulation (Endogenous Analgesia)
The brain modulates pain from above via descending pathways:
- Periaqueductal gray (PAG) - midbrain; activated by opioids and stress. Projects to the rostral ventromedial medulla (RVM).
- Nucleus raphe magnus (RVM) - serotonergic; projects down to dorsal horn via the dorsolateral funiculus.
- Locus coeruleus - noradrenergic; sends norepinephrine to dorsal horn inhibitory interneurons.
These pathways release serotonin, norepinephrine, GABA, and enkephalins in the dorsal horn to inhibit further pain transmission. Drugs like SNRIs (duloxetine), tricyclic antidepressants, and tramadol exploit these descending systems for analgesia.
10. Central Sensitization and Neuroplasticity
With persistent noxious input, the dorsal horn can undergo central sensitization:
- Decreased activation threshold
- Wind-up of WDR neurons (NMDA receptor activation is key)
- Spontaneous activity and expansion of receptive fields
- Expressed as allodynia (pain from non-noxious stimuli) and hyperalgesia (exaggerated pain from noxious stimuli)
This transition from acute to chronic pain can occur within 1 hour of intense noxious input. The NMDA receptor, substance P, and protein kinase C are central to this process. NMDA antagonists (ketamine) can prevent or reverse central sensitization. - Miller's Anesthesia, 10e
Summary Flowchart
TISSUE INJURY / NOXIOUS STIMULUS
↓
Peripheral nociceptors (free nerve endings)
↓
Aδ / C fibers → Dorsal Root Ganglion (1st-order neuron)
↓
Dorsal Horn (laminae I, II, V) → synapses with 2nd-order neurons
↓ Crosses midline at anterior commissure
Spinothalamic Tract (contralateral) → ascends to thalamus
↓
VPL thalamus (3rd-order neuron) + Intralaminar nuclei
↓
Somatosensory cortex (S1) + Cingulate + Insula
↓
PAIN PERCEPTION (sensory-discriminative + affective-motivational)
↑ ↑ Descending modulation from PAG → RVM → dorsal horn
↑ ↑ Gate control: Aβ input inhibits projection neurons
Sources: Morgan & Mikhail's Clinical Anesthesiology, 7e | Miller's Anesthesia, 10e | Neuroanatomy through Clinical Cases, 3e | Neuroscience: Exploring the Brain, 5e | Barash Clinical Anesthesia, 9e
This is a shared conversation. Sign in to Orris to start your own chat.