Regulatory factors of heart rate
Reading File
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed to compose a thorough, well-structured answer. Here is the complete response:
Regulatory Factors of Heart Rate
Heart rate regulation can be divided into two broad categories: intrinsic (inherent) factors within the heart itself and extrinsic (systemic) factors that act on the heart from outside.
1. Intrinsic Regulation - The Conducting System
The heart can contract rhythmically without any external input. This automaticity is generated by the conducting system.
SA Node - The Dominant Pacemaker
The sinoatrial (SA) node, located near the junction of the superior vena cava and the right atrium, has the fastest intrinsic rate of depolarization: 60-100 beats/min. It is composed of two cell types:
- P cells (pacemaker cells) - generate spontaneous electrical impulses
- T cells (transitional cells) - propagate impulses into the right atrium
The SA node initiates the impulse, which spreads across the atria, reaches the AV node, travels down the Bundle of His, bundle branches, and terminates as Purkinje fibers in the ventricular myocardium.
Hierarchy of Escape Pacemakers
If the SA node fails, the next-fastest site takes over:
| Site | Intrinsic Rate |
|---|---|
| SA node | 60-100 bpm |
| AV node | ~50 bpm |
| Purkinje fibers (ventricles) | 30-40 bpm |
This hierarchy ensures the heart never completely stops due to failure of a single site.
Bainbridge (Atrial Stretch) Reflex
Stretching of the right atrial wall directly increases heart rate by 10-20%. Increased venous return stretches the atria, which stimulates stretch receptors and triggers a reflex tachycardia - a built-in feedback mechanism to match cardiac output to venous return. - Guyton and Hall Textbook of Medical Physiology
2. Extrinsic Regulation
A. Autonomic Nervous System
This is the primary extrinsic regulator of heart rate. The two divisions act antagonistically on the SA and AV nodes.
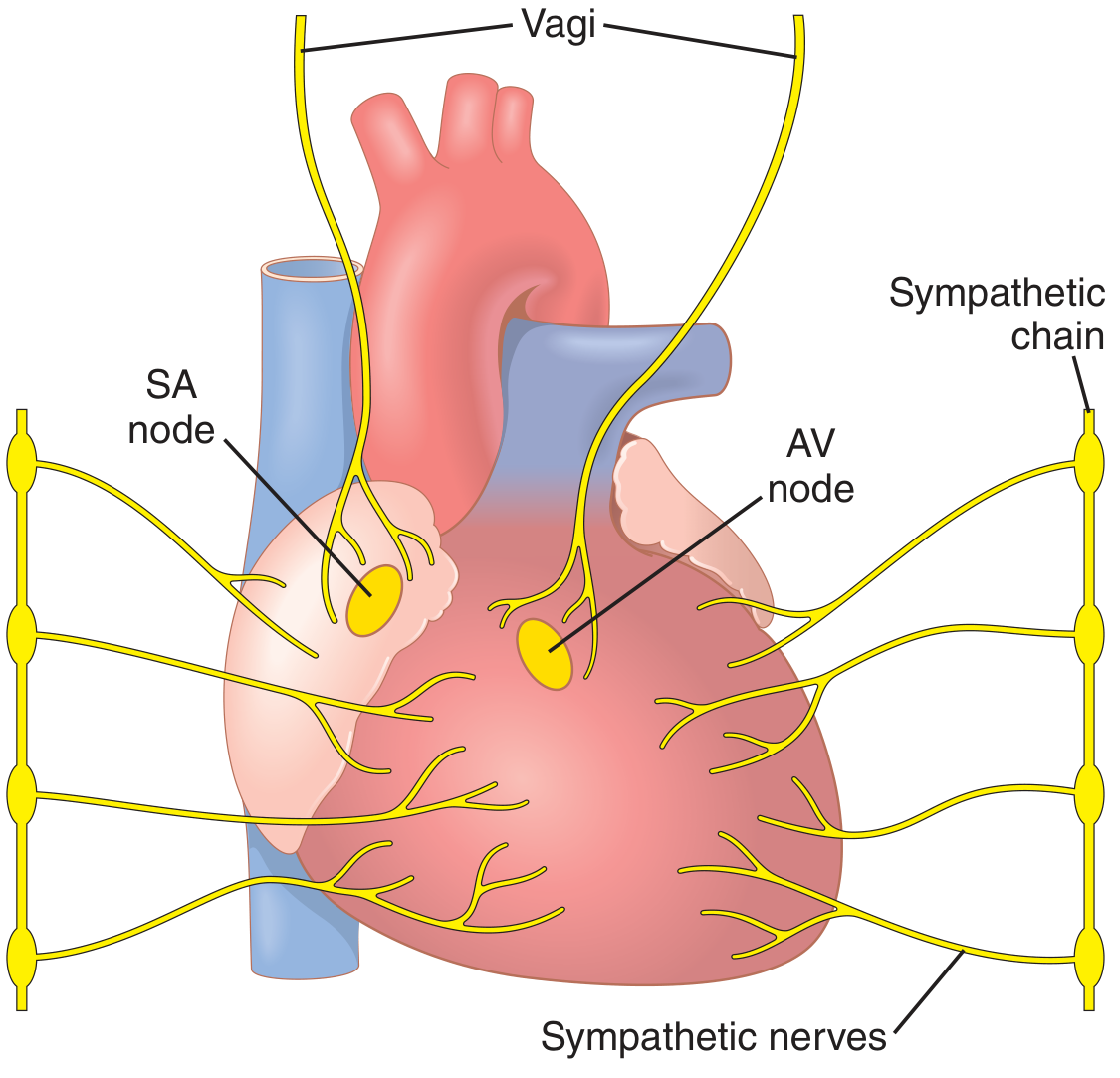
Sympathetic Stimulation (Positive Chronotropy)
- Origin: Lateral horns at T1-T6 spinal cord segments; postganglionic fibers from cervical and thoracic paravertebral ganglia
- Neurotransmitter: Norepinephrine, acting on β₁-adrenergic receptors
- Effect: Increases the rate of SA node depolarization
- Normal rate (70 bpm) can increase to 180-200 bpm, occasionally 250 bpm
- Also increases force of contraction (positive inotropy)
- Maximum cardiac output increased 2-3 fold
- Under resting conditions, sympathetic tone maintains pumping ~30% above basal
Parasympathetic Stimulation (Negative Chronotropy)
- Origin: Vagus nerve (CN X); short postganglionic fibers within the heart
- Neurotransmitter: Acetylcholine, acting on muscarinic receptors
- Targets: Primarily SA and AV nodes (vagal fibers largely spare the ventricles)
- Effect: Slows heart rate, decreasing it below 60 bpm (bradycardia)
- Strong vagal stimulation can transiently stop the heart for a few seconds, after which the heart "escapes" and beats at 20-40 bpm
- Decreases force of atrial contraction by 20-30%
- Ventricular pumping can decrease >50%
The dominant resting influence is vagal (parasympathetic) tone, which keeps resting heart rate below the SA node's intrinsic rate. - Histology: A Text and Atlas (Ross & Pawlina)
B. Baroreceptor (Reflex) Regulation
High-Pressure Baroreceptors
Located in the carotid sinus and aortic arch. When arterial pressure rises:
- Increased stretch → afferent signals → cardiovascular center in medulla
- Efferent response: increased vagal tone + decreased sympathetic tone → bradycardia
- Conversely, a fall in arterial pressure leads to reflex tachycardia
Baroreceptors regulate heart rate as part of arterial blood pressure control, not cardiac output per se. They respond when changes in cardiac output happen to change mean arterial pressure. - Medical Physiology (Boron & Boulpaep)
Low-Pressure (Volume) Receptors
Located in the pulmonary artery, atria, and ventricles. They detect venous return and cardiac fullness. Distension triggers reflex tachycardia and renal vasodilation, facilitating diuresis. These are particularly important in regulating heart rate in response to volume load.
C. Chemoreceptor Regulation
Peripheral chemoreceptors (carotid and aortic bodies) detect:
- ↓ PO₂ (hypoxia)
- ↑ PCO₂ (hypercapnia)
- ↓ pH (acidosis)
These stimuli produce reflex tachycardia, which is adaptive - reduced cardiac output causes low PO₂ and high PCO₂, and the chemoreceptor-driven tachycardia helps restore cardiac output. This is a particularly helpful feedback mechanism since chemoreceptors detect the metabolic consequences of reduced cardiac output. - Medical Physiology (Boron & Boulpaep)
D. Hormonal / Humoral Factors
| Substance | Receptor | Effect on Heart Rate |
|---|---|---|
| Epinephrine (adrenal medulla) | β₁-adrenergic | Positive chronotropy (tachycardia) |
| Norepinephrine (adrenal medulla) | β₁-adrenergic | Positive chronotropy (lesser than Epi) |
| Thyroid hormones (T₃/T₄) | Nuclear receptors | Increase HR; upregulate β-receptors |
| Glucagon | Specific receptors | Positive chronotropy |
| Acetylcholine | Muscarinic (M₂) | Negative chronotropy |
These hormones reach the cardiac myocytes via the coronary circulation and act independently of neural input. - Histology: A Text and Atlas (Ross & Pawlina)
E. Electrolyte Effects
Potassium (K⁺)
- Hyperkalemia: Decreases resting membrane potential (partial depolarization) → slows the heart rate, weakens contraction, and can cause fatal arrhythmia at 8-12 mEq/L
- Hypokalemia: Increases automaticity and predisposes to tachyarrhythmias
Calcium (Ca²⁺)
- Hypercalcemia: Moves the heart toward spastic contraction; increases force and rate
- Hypocalcemia: Cardiac weakness, effects similar to hyperkalemia
- Ca²⁺ directly initiates the cardiac contractile process and modulates pacemaker activity
F. Temperature
- Fever / hyperthermia: Markedly increases heart rate (may double at high fevers) - increased membrane permeability to pacemaker ions accelerates SA node depolarization
- Hypothermia: Severely slows heart rate; near hypothermic death (15-21°C), heart rate falls to just a few beats per minute
This is why surgeons can cool the body during cardiac surgery to allow a bloodless field with very slow or arrested heart rate. - Guyton and Hall Textbook of Medical Physiology
G. CNS Higher Centers
- Hypothalamus: Cardiovascular regulation center; stimulation of different hypothalamic areas can produce both tachycardia and bradycardia depending on the region
- Cerebral cortex: Emotional states (fear, anxiety, excitement) increase heart rate via sympathetic activation
- Medullary cardiovascular center: Integrates baroreceptor, chemoreceptor, and higher center inputs; sends final efferent output via sympathetic and vagal pathways
Summary Table
| Category | Factor | Effect |
|---|---|---|
| Intrinsic | SA node automaticity | Sets baseline rate (60-100 bpm) |
| Intrinsic | Bainbridge reflex (atrial stretch) | +10-20% rate |
| Autonomic | Sympathetic (NE/β₁) | ↑ HR (tachycardia) |
| Autonomic | Parasympathetic/vagal (ACh/M₂) | ↓ HR (bradycardia) |
| Reflex | High-pressure baroreceptors | Tachycardia or bradycardia (homeostatic) |
| Reflex | Low-pressure/volume receptors | Reflex tachycardia with volume load |
| Reflex | Chemoreceptors (hypoxia, acidosis) | Tachycardia |
| Hormonal | Epinephrine, T₃/T₄ | ↑ HR |
| Electrolyte | Hyperkalemia | ↓ HR (bradycardia, arrest) |
| Electrolyte | Hypercalcemia | ↑ HR / spasm |
| Physical | Hyperthermia | ↑ HR |
| Physical | Hypothermia | ↓ HR |
| CNS | Hypothalamus, cortex | Modulate via ANS |
Sources:
- Guyton and Hall Textbook of Medical Physiology, 14th ed.
- Medical Physiology - Boron & Boulpaep
- Histology: A Text and Atlas with Correlated Cell and Molecular Biology - Ross & Pawlina
This is a shared conversation. Sign in to Orris to start your own chat.