Anatomy of testis
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Loading Image
I now have all the information needed for a comprehensive answer. Here is the complete anatomy of the testis:
Anatomy of the Testis
1. Overview and Dimensions
The testis is a paired male gonad located in the scrotum. At sexual maturity, each testis is approximately 4 × 3 × 2.5 cm (or ~5 cm long and 3 cm wide), with an average volume of 18 mL (range 12-30 mL). The combined weight of the testis and epididymis is approximately 20-30 g. Volume can be estimated using an orchidometer or ultrasound formula: length × width × height × 0.71.
2. Coverings (Tunics)
From outside in:
| Layer | Details |
|---|---|
| Scrotal skin | Thin, rugose skin |
| Tunica dartos | Smooth muscle layer responsible for scrotal rugosity |
| External spermatic fascia | Derived from external oblique aponeurosis |
| Cremasteric fascia & Cremaster muscle | From internal oblique; responsible for cremasteric reflex (L1/L2) |
| Internal spermatic fascia | Derived from transversalis fascia |
| Tunica vaginalis (parietal layer) | Serous lining; separated from visceral layer by the serous cavity of the testis |
| Tunica vaginalis (visceral layer) | Closely adherent to the testis anteriorly and laterally |
| Tunica albuginea | Dense fibrous capsule; tough, rubbery consistency; the innermost covering directly on testicular tissue |
Between the visceral and parietal layers of the tunica vaginalis lies a small, mesothelium-lined serous cavity containing a scant amount of fluid (epididymal sinus). Abnormal fluid accumulation here is a hydrocele.
3. Internal Structure
- Tunica albuginea - the dense fibrous capsule sends fibrous septa radially inward toward the posterior aspect
- Mediastinum testis - the posterior thickening of the tunica albuginea where the septa converge; houses the rete testis and major vessels
- Lobules - the septa divide the testis into approximately 250-370 wedge-shaped lobules
- Seminiferous tubules - each lobule contains 1-4 highly convoluted seminiferous tubules, each about 60 cm long when uncoiled; this is where spermatogenesis occurs
- Rete testis - an anastomosing network of channels within the mediastinum testis that receives outflow from the seminiferous tubules
- Efferent ductules - approximately 10-15 efferent ductules pass from the rete testis to the head of the epididymis
4. Histology
The seminiferous tubule has a basement membrane supported by connective and elastic tissue, bearing two cell populations:
- Sertoli (sustentacular) cells - supporting cells; secrete Anti-Mullerian Hormone (AMH); form the blood-testis barrier
- Spermatogenic cells - the precursors of mature spermatozoa (spermatogonia → primary spermatocyte → secondary spermatocyte → spermatid → spermatozoon)
The stroma between seminiferous tubules contains connective tissue with interstitial Leydig cells, which synthesize testosterone in response to LH.
5. Relations
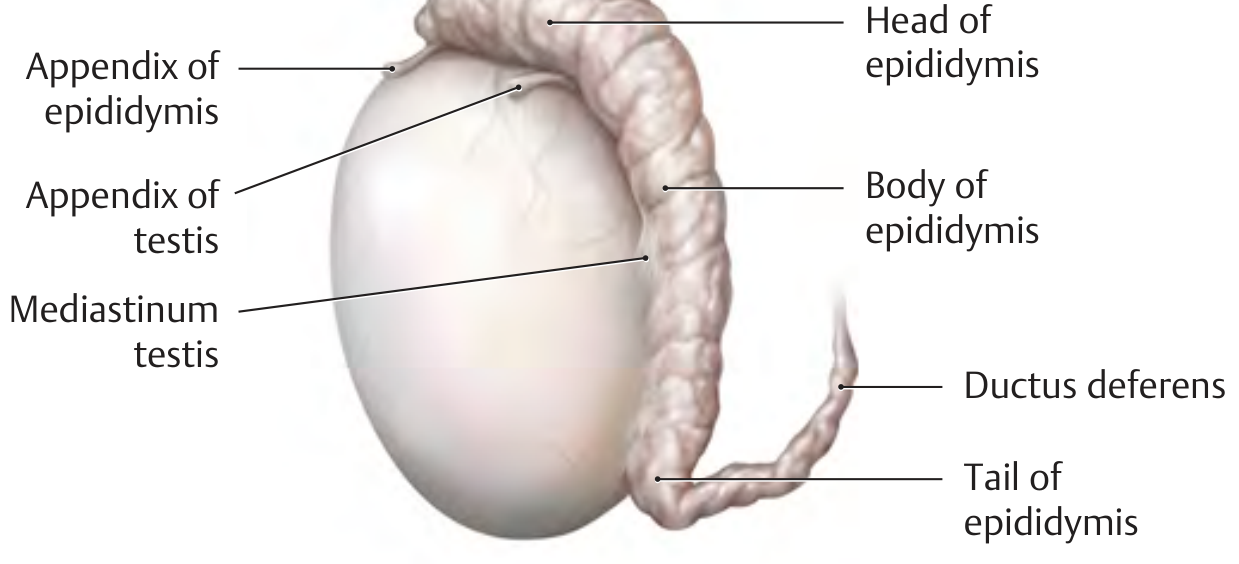
- The testis is closely attached posterolaterally to the epididymis, particularly at its upper and lower poles
- The appendix testis (a small pedunculated/sessile remnant of the paramesonephric duct) is located at the upper pole - it can undergo torsion
- The epididymis runs along the posterior surface: head (caput) at the upper pole → body (corpus) → tail (cauda) at the lower pole, which is continuous with the ductus deferens
6. Blood Supply
Arterial (3 arteries anastomose with each other)
| Artery | Origin |
|---|---|
| Testicular artery (internal spermatic artery) | Directly from the abdominal aorta, just below the renal arteries |
| Artery of the ductus deferens | Internal iliac (hypogastric) artery |
| Cremasteric artery | Inferior epigastric artery |
The testicular artery arises at the level of L2, reflecting the gonadal embryological origin near the kidneys.
Venous
Blood drains into the pampiniform plexus - an elongated venous network surrounding the testicular artery within the spermatic cord. This plexus acts as a counter-current heat exchanger, cooling arterial blood to keep the testis slightly below body temperature (essential for spermatogenesis).
At the internal inguinal ring, the pampiniform plexus converges to form the spermatic vein (testicular vein):
- Right testicular vein → enters the inferior vena cava (IVC) just below the right renal vein (oblique angle)
- Left testicular vein → enters the left renal vein at a right angle - this creates a physiologically significant constriction prone to obstruction, explaining why varicocele is far more common on the left side
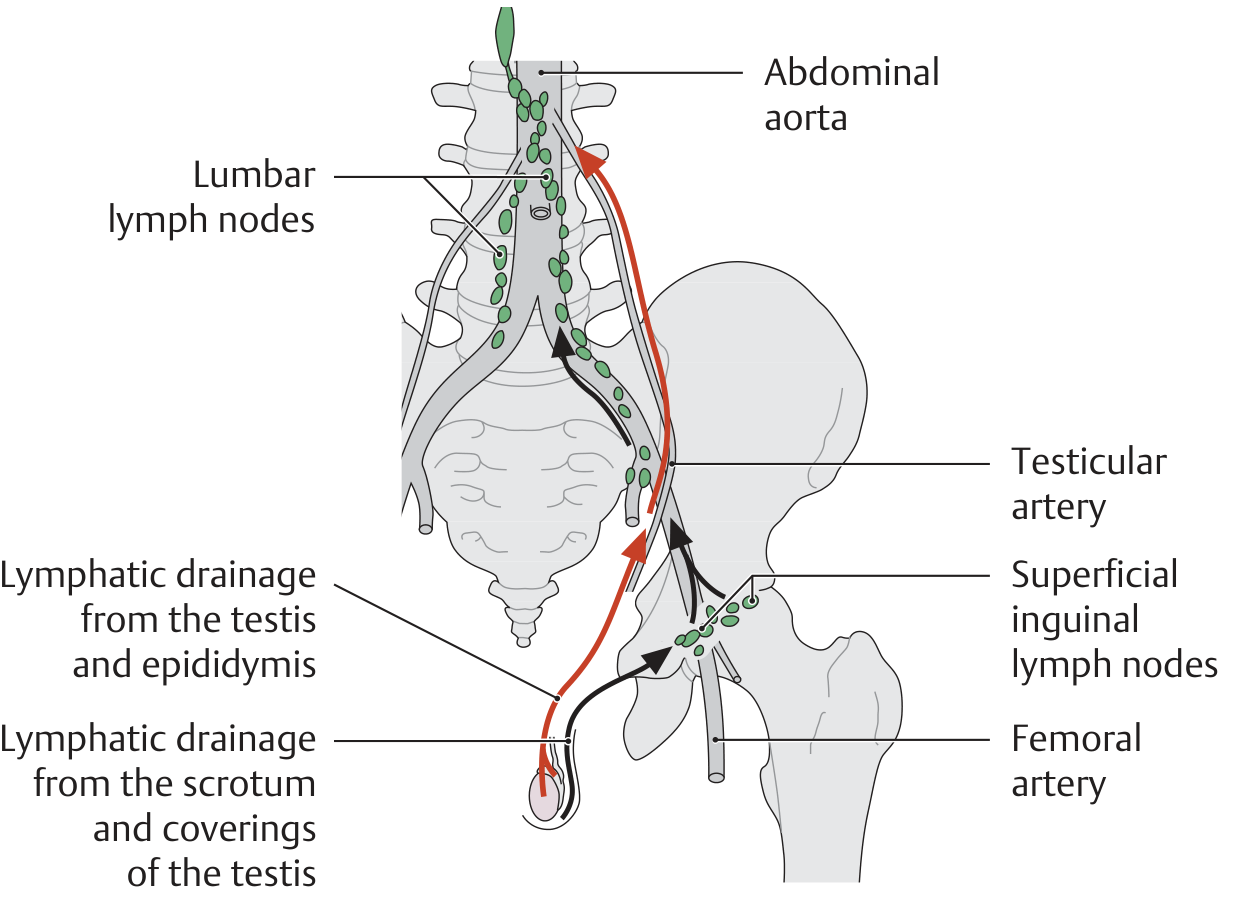
7. Lymphatic Drainage
- Testis and epididymis → lymphatics follow the testicular vessels → drain to lumbar (para-aortic) lymph nodes (at L1-L2 level)
- Scrotum and coverings → drain to superficial inguinal lymph nodes
Clinical note: This distinction is vital - testicular tumors metastasize to retroperitoneal para-aortic nodes, NOT to inguinal nodes (unless the scrotal skin is invaded or prior inguinal surgery has disrupted lymphatics).
8. Nerve Supply
| Component | Nerve |
|---|---|
| Sensory (and autonomic) | Testicular plexus (T10-T11) via branches from the renal and aortic plexuses accompanying the testicular artery |
| Cremasteric reflex (motor) | Genitofemoral nerve (L1-L2) - the genital branch |
| Referred pain | Because testicular nerves arise at T10, pain from the testis is referred to the umbilical region (T10 dermatome) |
9. Spermatic Cord Contents
The spermatic cord suspends the testis and runs from the deep (internal) inguinal ring to the posterior border of the testis. Its contents include:
- Vas deferens (ductus deferens)
- Testicular artery
- Pampiniform plexus (testicular veins)
- Cremasteric artery and artery of vas deferens
- Genital branch of genitofemoral nerve
- Sympathetic nerve fibers
- Lymphatic vessels
Sources:
- General Anatomy and Musculoskeletal System, THIEME Atlas of Anatomy, pp. 247-248
- Smith and Tanagho's General Urology, 19th Edition, p. 27
- Campbell-Walsh-Wein Urology, 3-Volume Set
Also add source BDC
Finding Sources
Finding Sources
Finding Sources
Unfortunately, BD Chaurasia's Human Anatomy is not available in the medical textbook library. The anatomy books currently in the library are:
- THIEME Atlas of Anatomy - General Anatomy and Musculoskeletal System
- Gray's Anatomy for Students
- Netter's Atlas of Human Anatomy
- Color Atlas of Human Anatomy (Vols 1, 2, 3 - Sobotta/Schiebler)
- Imaging Anatomy: Bones, Joints, Vessels and Nerves
BD Chaurasia (BDC) is not among them. Would you like me to:
- Pull testis anatomy from Gray's Anatomy for Students - a very commonly used and authoritative reference that covers similar ground to BDC
- Pull from Netter's Atlas - excellent for visual/diagram-based anatomy
- Both - combine Gray's and Netter's to supplement the existing answer
Go for Both
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Loading Image
All four Netter diagrams retrieved. Here is the updated comprehensive answer incorporating Gray's Anatomy for Students and Netter's Atlas:
Anatomy of the Testis
Sources: THIEME Atlas | Smith & Tanagho's Urology | Campbell-Walsh-Wein | Gray's Anatomy for Students | Netter's Atlas of Human Anatomy
1. Overview and Dimensions
The testis is a paired male gonad that originally develops high on the posterior abdominal wall and then descends - normally before birth - through the inguinal canal into the scrotum. During this descent it carries its vessels, lymphatics, nerves, and ductus deferens with it. At sexual maturity, each testis measures approximately 4 × 3 × 2.5 cm (length ~5 cm, width ~3 cm), with an average volume of 18 mL (range 12-30 mL) and combined weight with epididymis of approximately 20-30 g.
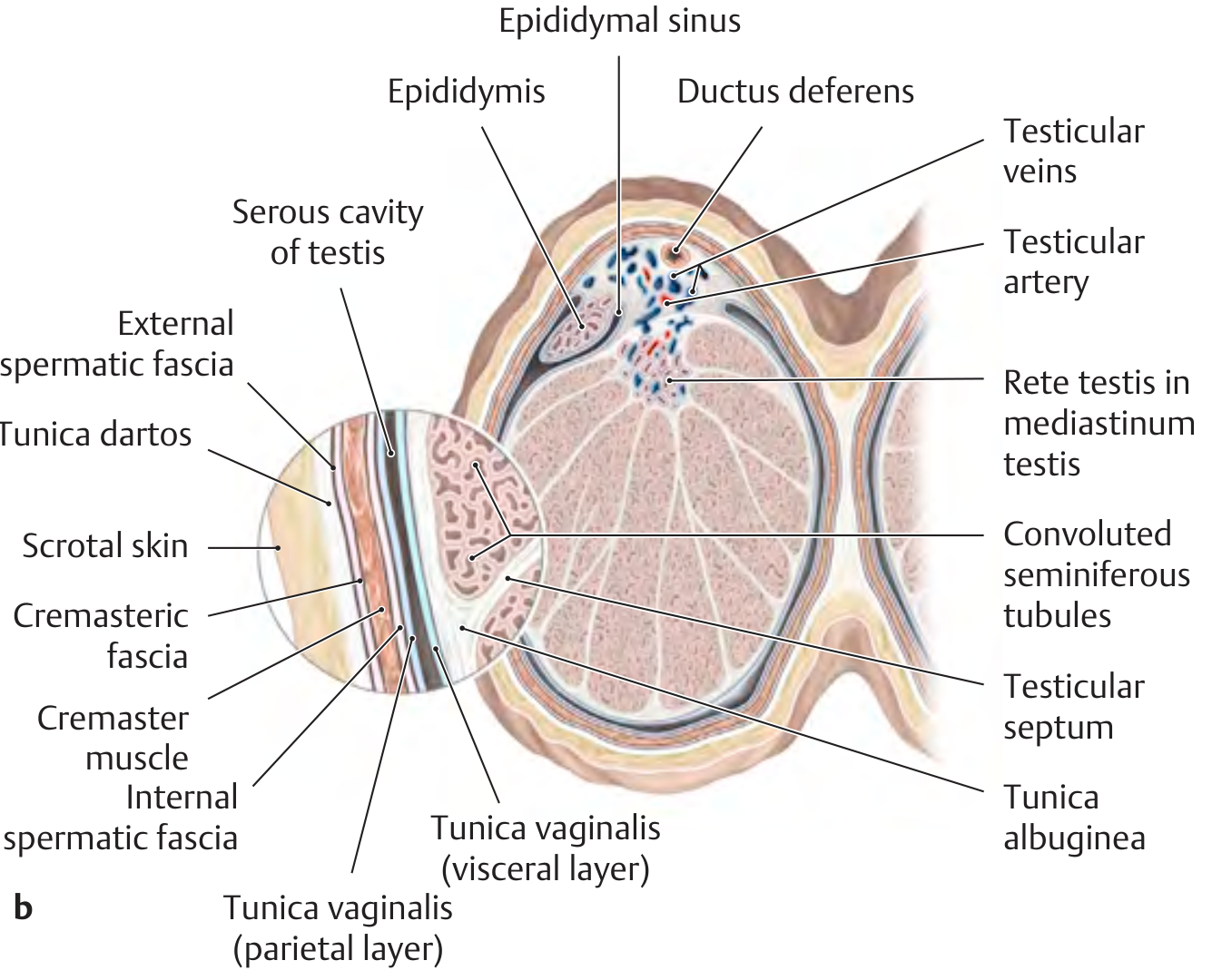
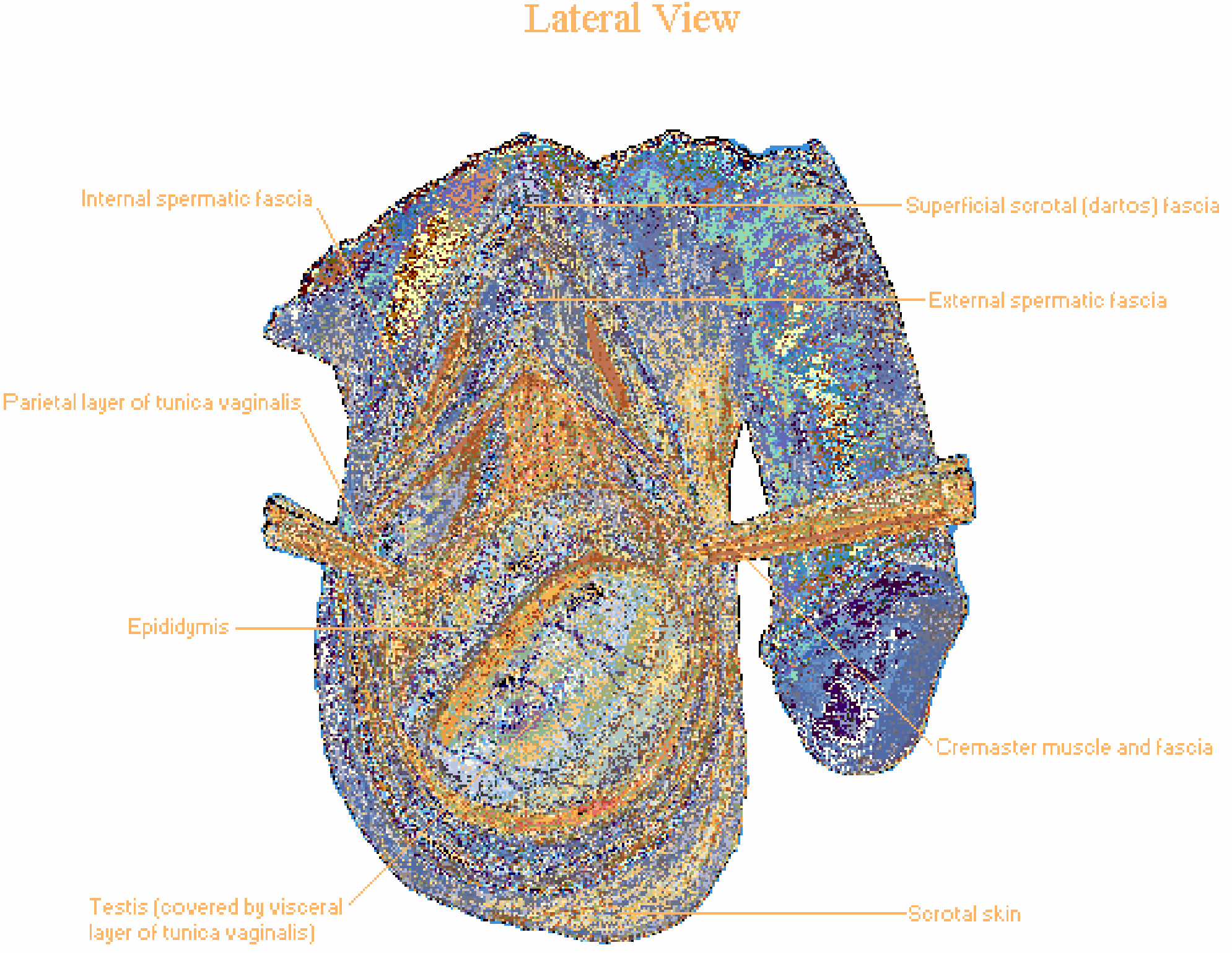
2. Coverings of the Testis (from outside in)
Each testis is enclosed within the end of an elongated musculofascial pouch continuous with the anterior abdominal wall. The layers, from outermost to innermost, are:
| Layer | Embryological Derivation |
|---|---|
| Scrotal skin | Labioscrotal swellings |
| Superficial (dartos) fascia | Superficial fascia of abdomen (Scarpa's fascia) - contains smooth muscle |
| External spermatic fascia | External oblique aponeurosis |
| Cremaster muscle and fascia | Internal oblique muscle - responsible for cremasteric reflex |
| Internal spermatic fascia | Transversalis fascia |
| Parietal layer of tunica vaginalis | Peritoneum (processus vaginalis) |
| Visceral layer of tunica vaginalis | Peritoneum - covers anterior and lateral surfaces of testis |
| Tunica albuginea | Dense fibrous capsule directly enclosing testicular tissue |
The visceral and parietal layers of the tunica vaginalis are separated by a small serous cavity (sinus/cavity of testis). Abnormal accumulation of fluid here = hydrocele.
Netter's Lateral View showing the layers of the testis within the scrotum:
THIEME cross-section showing all coverings and internal structure:
Netter's cross-section for comparison:
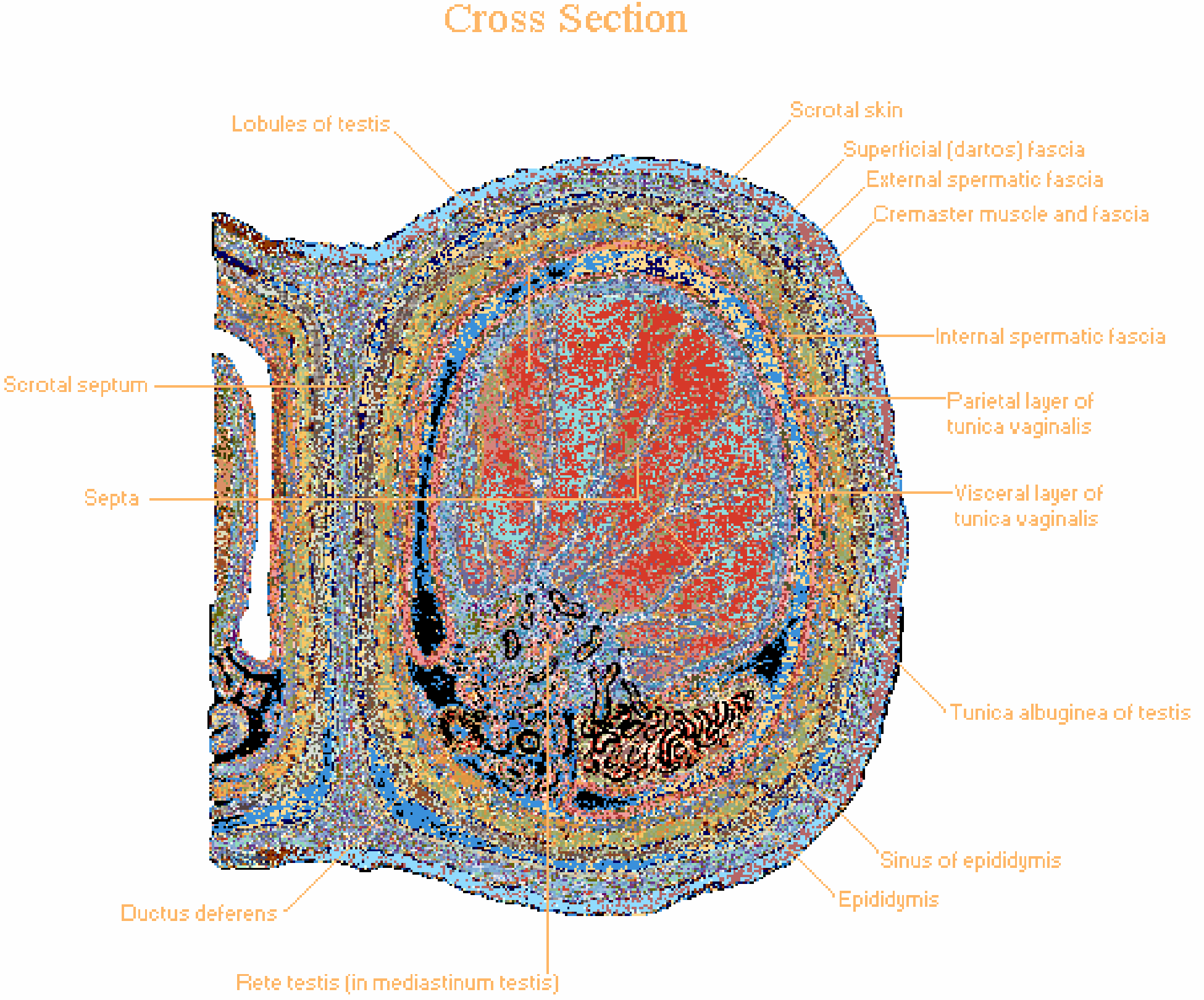
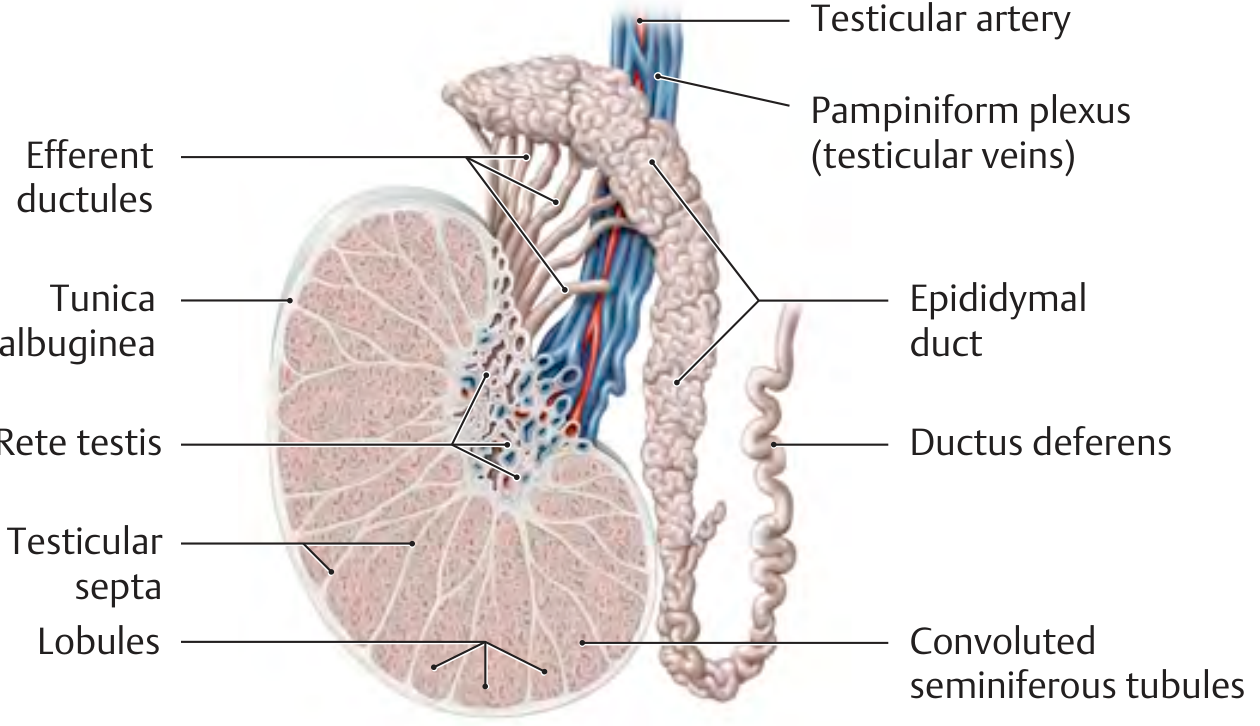
3. Internal Structure
- Tunica albuginea - thick dense fibrous capsule; invaginates posteriorly to form the mediastinum testis
- Mediastinum testis - the posterior connective tissue wedge housing the rete testis and main vessels; septa radiate from here
- Testicular septa - fibrous septa extending from the tunica albuginea toward the mediastinum, dividing the testis into ~250-370 wedge-shaped lobules
- Seminiferous tubules - each lobule contains 1-4 highly coiled tubules, each ~60 cm long; 400-600 total per testis; both ends become straight tubules that drain into the rete testis
- Rete testis - anastomosing channel network within the mediastinum testis; receives drainage from all seminiferous tubules
- Efferent ductules - 12-20 ductules arise from the upper end of the rete testis, pierce the tunica albuginea, and connect with the head of the epididymis
Netter's Frontal Section showing internal structure:
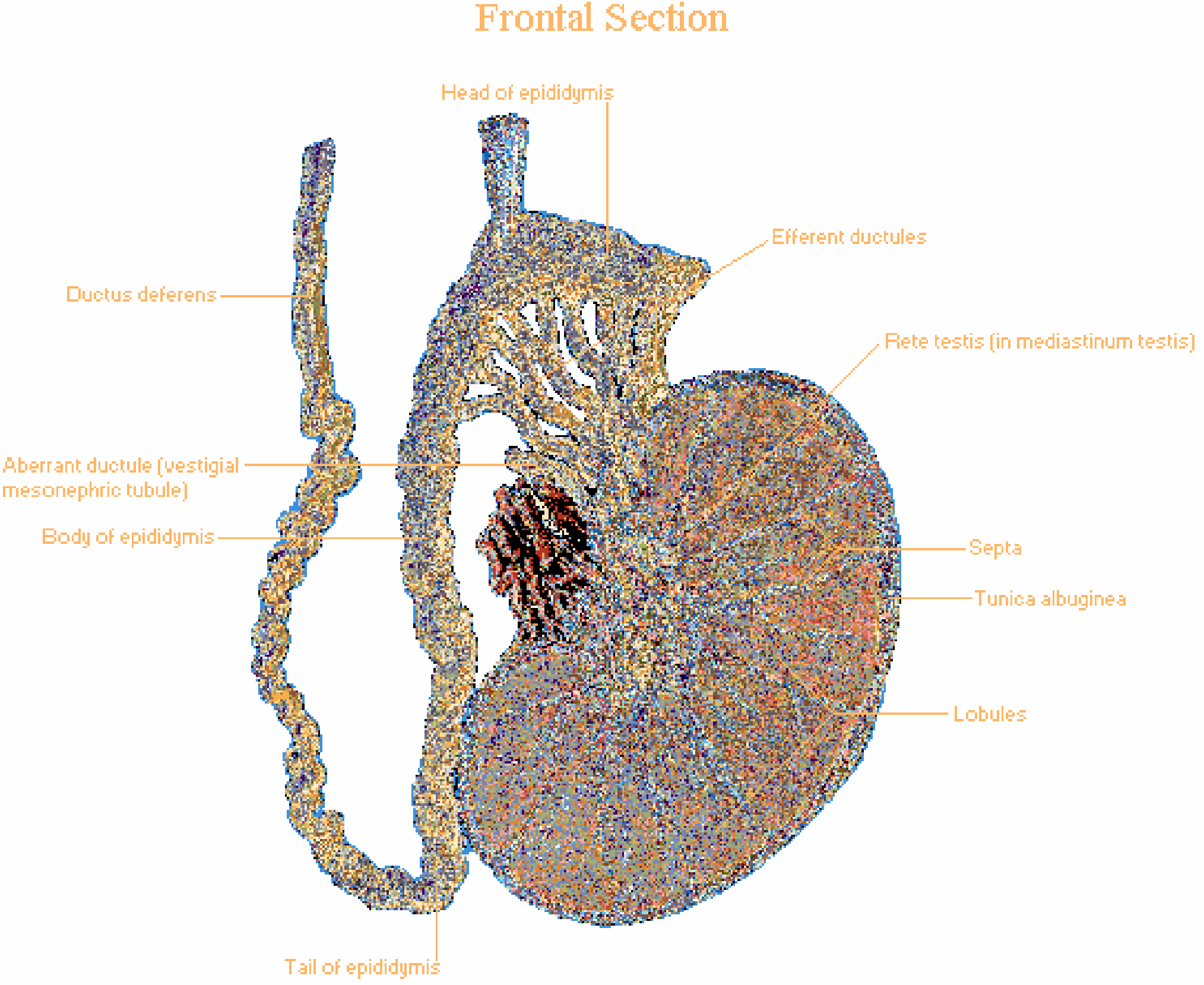
THIEME/Netter schema of tubular continuity:
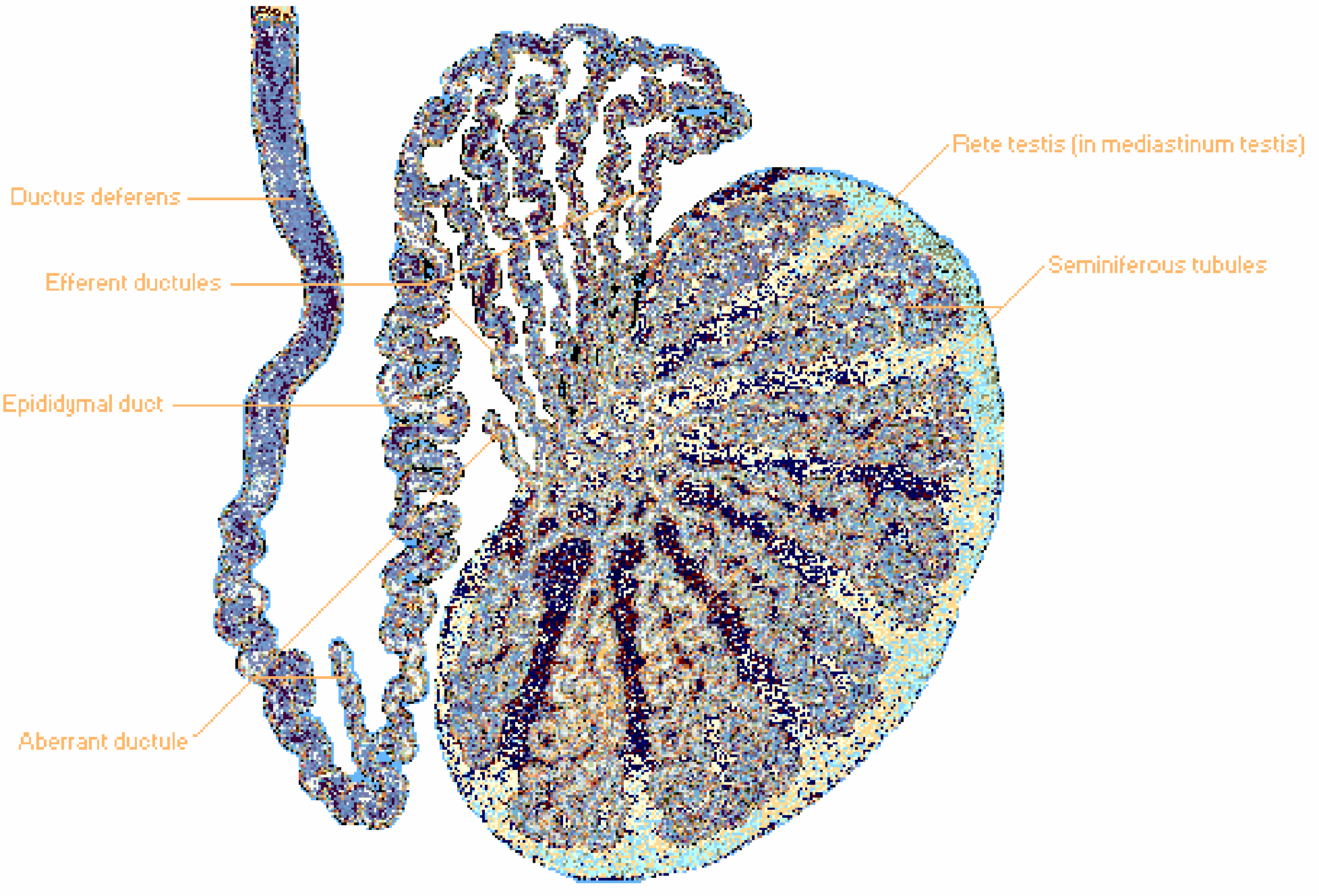
Gray's Anatomy adds the key detail that the straight tubules at each end of the seminiferous tubules connect to the rete testis, which sits within "a thick, vertically oriented linear wedge of connective tissue (the mediastinum testis), projecting from the capsule into the posterior aspect of the gonad."
4. Histology
The seminiferous tubule wall contains:
- Sertoli (sustentacular) cells - supporting cells; form the blood-testis barrier; secrete Anti-Mullerian Hormone (AMH) and androgen-binding protein
- Spermatogenic cells - in progressive stages from basal to luminal: spermatogonia → primary spermatocyte → secondary spermatocyte → spermatid → spermatozoon
The interstitium between tubules contains Leydig cells (interstitial cells), which secrete testosterone in response to LH stimulation.
5. Relations
- Closely attached posterolaterally to the epididymis (especially at upper and lower poles)
- Appendix testis - small pedunculated remnant of the paramesonephric (Mullerian) duct at the upper pole; clinically may undergo torsion (most common cause of acute scrotum in prepubertal boys)
- A midline scrotal raphe is visible on the skin; in some individuals it extends from the anal aperture over the scrotum to the frenulum of the glans penis
6. Blood Supply
Arterial - 3 arteries with anastomoses
| Artery | Origin | Supply |
|---|---|---|
| Testicular (internal spermatic) artery | Abdominal aorta at L2, below renal arteries | Main supply to testis and epididymis |
| Artery of the ductus deferens | Internal iliac artery | Ductus deferens and epididymis |
| Cremasteric artery | Inferior epigastric artery | Coverings of testis |
This three-vessel supply is the reason that ligation of the testicular artery alone (e.g., during varicocelectomy) does not always result in testicular atrophy.
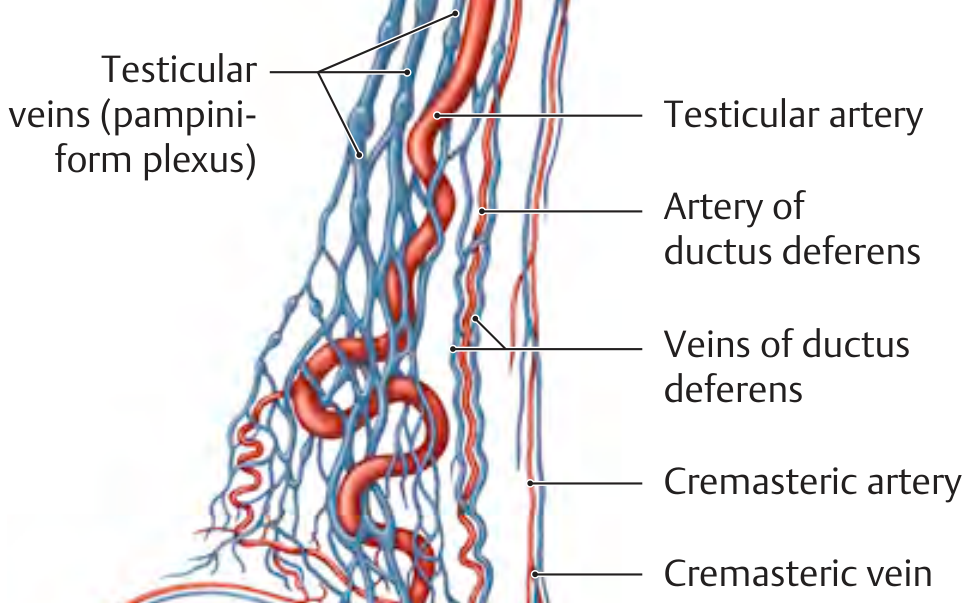
Venous - Pampiniform Plexus
- Venous blood drains into the pampiniform plexus - a network of veins surrounding the testicular artery, acting as a counter-current heat exchanger to maintain testicular temperature ~2-4°C below body temperature (required for spermatogenesis)
- At the internal inguinal ring, the plexus coalesces into the testicular (spermatic) vein:
- Right testicular vein → IVC (at an oblique angle)
- Left testicular vein → left renal vein at a right angle - this creates resistance to outflow, which is why varicocele occurs predominantly on the left (90%)
7. Lymphatic Drainage
| Structure | Drains To |
|---|---|
| Testis and epididymis | Lumbar (para-aortic) lymph nodes at L1-L2 |
| Scrotum and testicular coverings | Superficial inguinal lymph nodes |
Clinical point (Gray's): Because the testis developed in the abdomen and carried its lymphatics with it during descent, testicular tumors metastasize to retroperitoneal para-aortic nodes, NOT inguinal nodes. Inguinal node involvement only occurs if the scrotal skin or tunica vaginalis is invaded, or if prior surgery has disrupted normal lymphatic channels. This is also why testicular tumors must NOT be removed via a scrotal incision.
8. Nerve Supply
| Component | Nerve | Level |
|---|---|---|
| Autonomic and sensory (testis) | Testicular plexus (from renal and aortic plexuses) following the testicular artery | T10-T11 |
| Cremasteric reflex (afferent) | Ilioinguinal nerve | L1 |
| Cremasteric reflex (efferent/motor) | Genital branch of genitofemoral nerve | L1-L2 |
Because the testicular nerve supply arises at T10, pain from the testis is referred to the umbilical region (T10 dermatome). This is why a blow to the testis causes periumbilical pain, and why testicular torsion or tumor can occasionally present with abdominal pain.
9. Spermatic Cord
The spermatic cord runs from the deep inguinal ring to the posterior border of the testis. It is the "tube-shaped connection between the pouch in the scrotum and the abdominal wall" (Gray's). Contents:
- Ductus (vas) deferens
- Testicular artery
- Pampiniform plexus of veins
- Artery and vein of the ductus deferens
- Cremasteric artery and vein
- Genital branch of the genitofemoral nerve
- Sympathetic nerve fibers (testicular plexus)
- Lymphatic vessels
10. Descent of the Testis (Embryological Basis - Gray's)
The testis originally develops on the posterior abdominal wall. A fibrous cord - the gubernaculum - guides descent through the inguinal canal into the scrotum, typically completing by the last trimester of gestation. Arrest of descent = cryptorchidism (undescended testis):
- Found in ~30% of premature births, 3-5% of term births
- Usually completes descent spontaneously within 3 months after birth
- Watchful waiting recommended until 6 months; referral if still undescended; orchiopexy typically performed between 6-12 months
- During orchiopexy, the gubernaculum remnant (attaching the caudal pole of the testis to the scrotum) must be divided carefully
Sources:
- General Anatomy and Musculoskeletal System, THIEME Atlas of Anatomy, pp. 247-248
- Smith and Tanagho's General Urology, 19th Edition, p. 27
- Campbell-Walsh-Wein Urology, 3-Volume Set
- Gray's Anatomy for Students, pp. 327-328, 604, 7090-7116
- Netter's Atlas of Human Anatomy, pp. 658-663
This is a shared conversation. Sign in to Orris to start your own chat.