Describe the embryologic development of the thyroid gland and thyroglossal duct and explain the pathogenesis of a thyroglossal duct cyst.
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Finding Sources
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive, well-illustrated answer. Let me compile it.
Embryologic Development of the Thyroid Gland and Thyroglossal Duct
1. Origin of the Thyroid Primordium
The thyroid is the first endocrine gland to form in the embryo. Under the influence of Notch and Hedgehog signaling pathways, it begins to develop approximately 24 days after fertilization (around the 3rd–4th week of gestation) from a median endodermal thickening in the floor of the primordial pharynx — specifically at the junction of the anterior two-thirds and posterior one-third of the tongue, at a site that will become the foramen cecum. This thickening forms a small outpouching called the thyroid primordium (medial thyroid anlage), which is primarily composed of foregut endoderm.
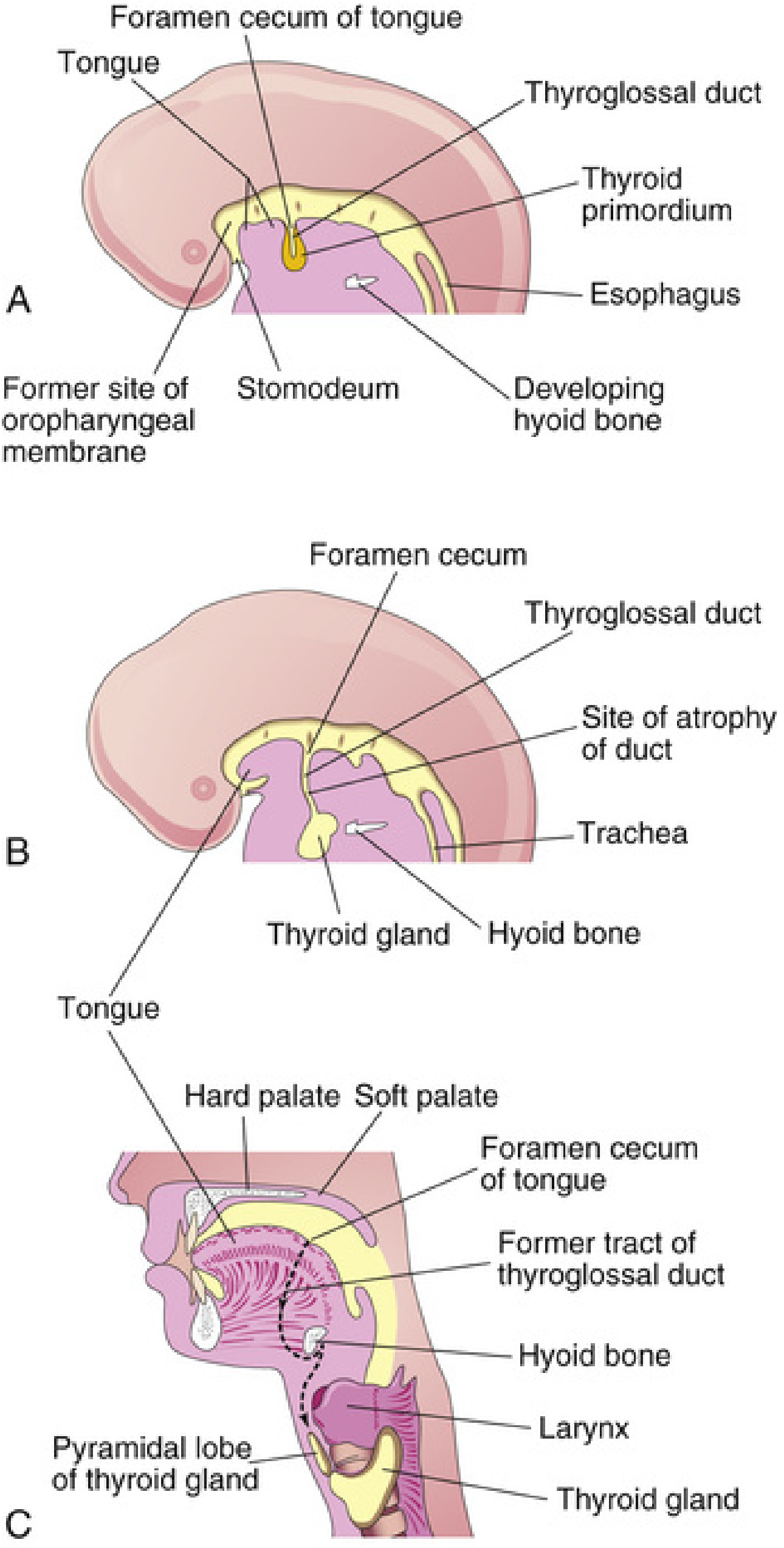
2. Descent and the Thyroglossal Duct
As the embryo and tongue grow, the thyroid primordium descends in the neck, passing ventral to the developing hyoid bone and laryngeal cartilages. During this migration, the anlage remains connected to the foramen cecum via an epithelial-lined tube — the thyroglossal duct. Key milestones:
| Week of Gestation | Event |
|---|---|
| ~3–4 weeks | Median thyroid anlage forms at the floor of pharynx (foramen cecum) |
| ~5 weeks | Thyroglossal duct lumen begins to obliterate; lateral anlages form from 4th branchial pouches |
| ~6 weeks | Thyroid descends past the hyoid bone; foramen cecum begins to resorb |
| ~7–8 weeks | Thyroid reaches its definitive anterior neck position; thyroglossal duct normally degenerates completely |
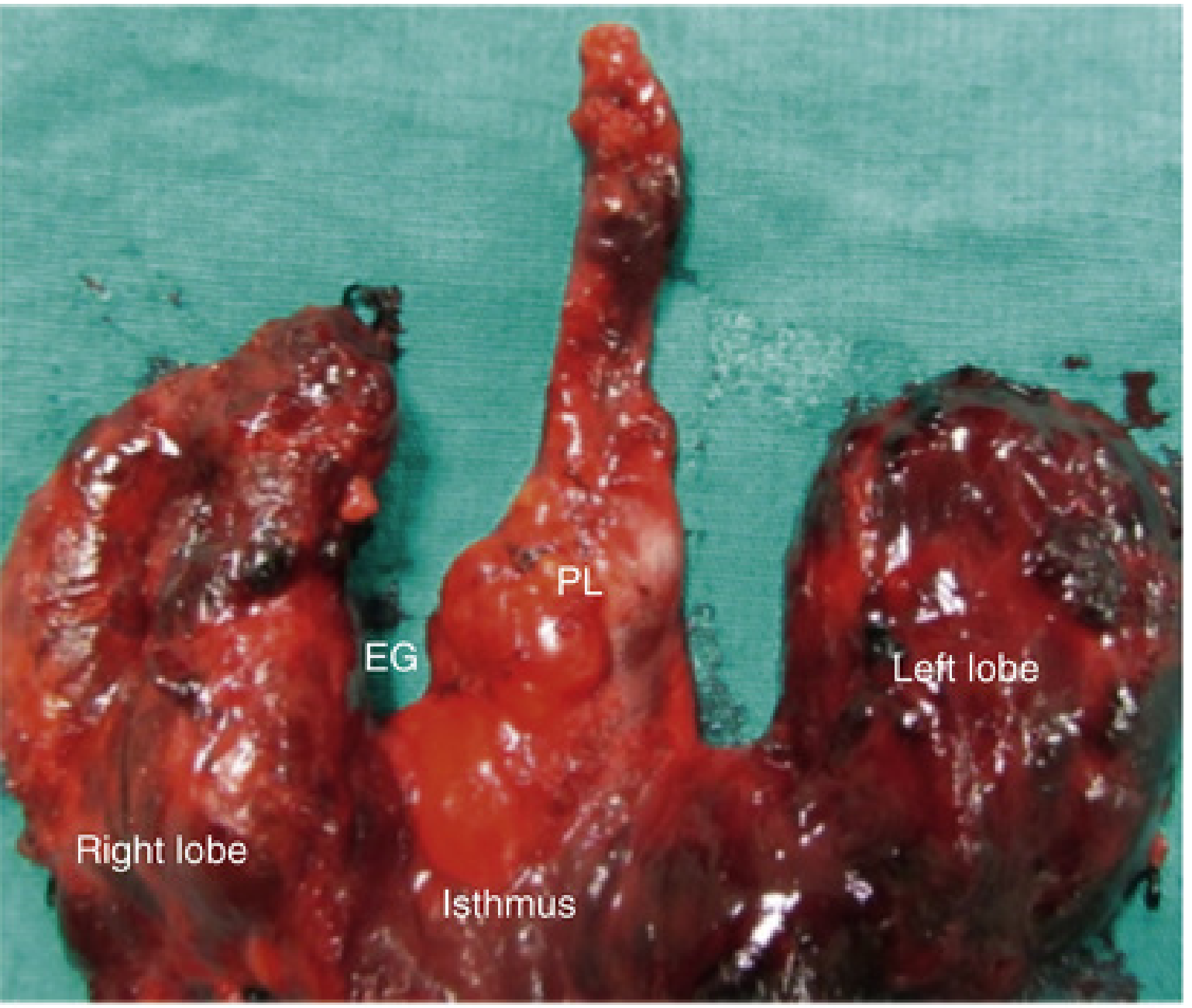
The thyroid's descent is intimately connected with the development of the hyoid bone — the duct passes in close association with its central portion. At first the thyroid primordium is hollow, but it soon becomes a solid cellular mass, then divides into right and left lobes connected by the isthmus, which lies anterior to the 2nd and 3rd tracheal rings.
3. Contribution of the Lateral Anlages
The paired lateral anlages originate from the 4th branchial pouch (ultimobranchial bodies) and are neuroectodermal in origin. They fuse with the median anlage at approximately the 5th week of gestation, forming the tubercle of Zuckerkandl. These lateral components contribute the calcitonin-producing parafollicular (C) cells, which come to lie in the superoposterior regions of the gland, while the midline median anlage gives rise to the thyroid follicular cells.
4. Histogenesis
- By 8 weeks: Thyroid follicles are initially apparent.
- By 10–11 weeks: Epithelial cords invaded by vascular mesenchyme divide into small clusters; lumina form, and cells arrange around thyroid follicles.
- By 11 weeks: Colloid begins to appear; iodine concentration and thyroid hormone synthesis can be demonstrated.
- By 20 weeks: Fetal TSH and thyroxine levels begin rising, reaching adult levels at 35 weeks.
Key transcription factors governing thyroid development include TTF1, FOXE1, PAX8, TSHR, and DUOX2, along with NIS (sodium-iodine symporter).
5. Normal Fate of the Thyroglossal Duct
By 7–8 weeks, the thyroglossal duct normally degenerates and disappears. Two remnants are normal and expected:
- The foramen cecum — a small pit persisting on the posterosuperior surface of the tongue, marking the original site of thyroid descent.
- The pyramidal lobe — present in ~50% of people; represents a persistent portion of the inferior end of the thyroglossal duct that has differentiated into thyroid tissue, extending superiorly from the isthmus and sometimes attached to the hyoid bone by fibrous tissue or smooth muscle.
Pathogenesis of Thyroglossal Duct Cysts
Mechanism
A thyroglossal duct cyst (TGDC) results from failure of the thyroglossal duct to involute completely after the thyroid reaches its definitive position. When epithelium-lined remnants of the duct persist despite complete thyroid descent, secretions accumulate within them and a cystic structure forms. The cyst can develop anywhere along the full migratory path — from the foramen cecum to the thyroid gland itself.
The close anatomical relationship between the duct and the central hyoid bone is pathogenically important: the duct descends immediately anterior to and around the hyoid, and hyoid development may actually divide or trap ductal remnants, explaining why ~80% of TGDCs are found juxtaposed to the hyoid bone.
Location Along the Tract
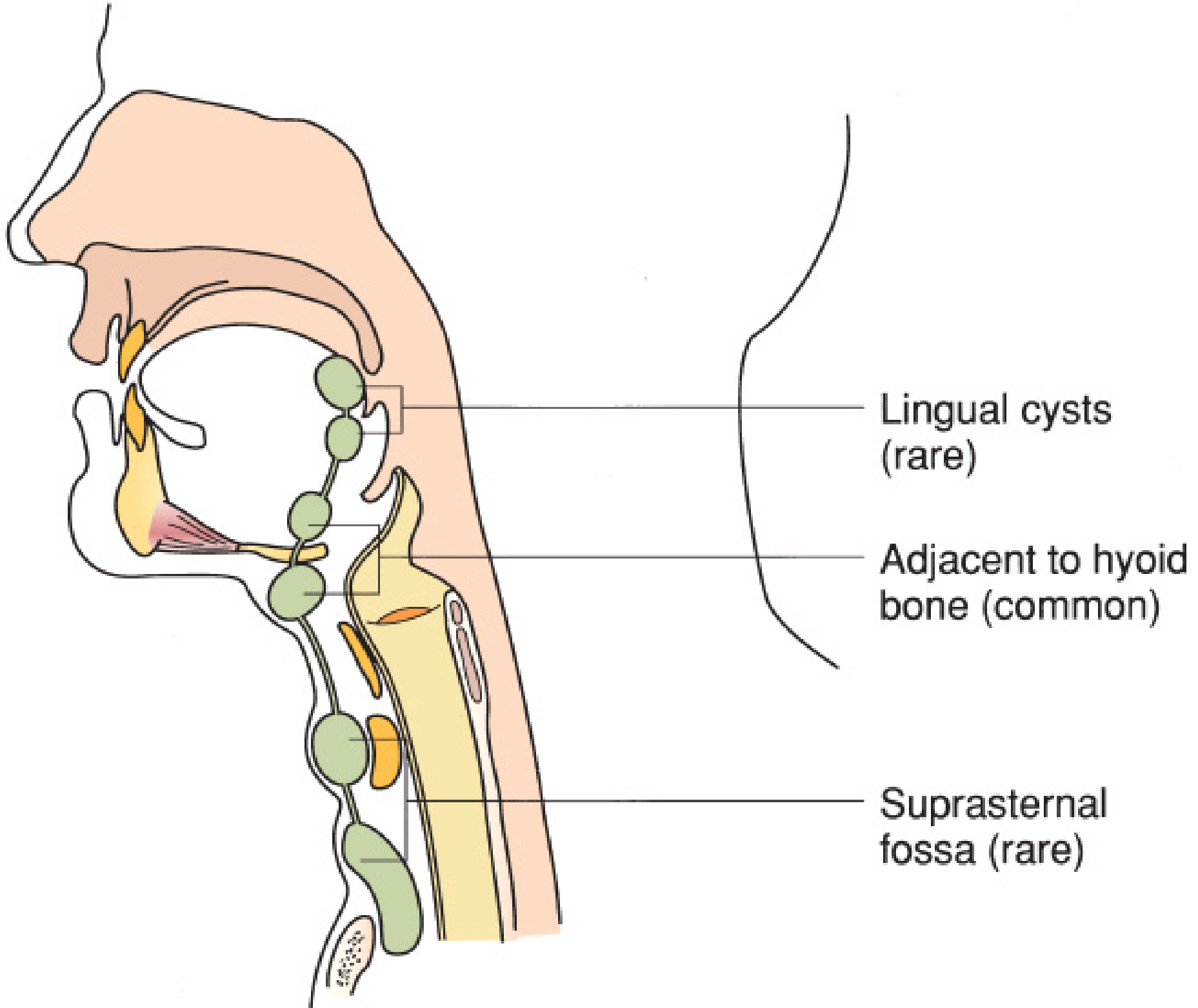
- Infrahyoid (most common, ~80%) — just below the hyoid bone, in the midline
- Suprahyoid / at the hyoid bone level
- Lingual — at or near the base of tongue (near foramen cecum) — rare
- Intralingual, suprasternal, or intrathyroidal — rare
Gross and Microscopic Pathology
The cysts are typically 1–4 cm in diameter. Their lining epithelium varies by location:
- Near the base of tongue (proximal tract): stratified squamous epithelium
- In lower (cervical) locations: pseudostratified ciliated columnar epithelium
- Transitional patterns occur between these two extremes
The fibrous cyst wall often contains lymphoid aggregates and, importantly, heterotopic thyroid follicular tissue in approximately 20% of cases — surgically significant because this may represent the patient's only functioning thyroid tissue.
Clinical Consequences of Ductal Persistence
| Feature | Detail |
|---|---|
| Presentation | Painless midline neck mass; moves upward with swallowing and tongue protrusion |
| Age at presentation | Most common in pediatric patients (2–4 years old as baby fat disappears); can present at any age |
| Infection | If the duct retains pharyngeal connection, oral bacteria may infect the cyst, producing an abscess and potentially a thyroglossal duct sinus (external drainage tract following spontaneous or surgical rupture) |
| Malignant potential | Exceedingly rare; papillary thyroid carcinoma arising in a TGDC has been reported, more often in adults |
Treatment
The Sistrunk operation is the definitive procedure — en-bloc excision of the cyst, the central portion of the hyoid bone, and the tract up to the base of the tongue with ligation at the foramen cecum. Simple cystectomy without hyoid resection carries a high recurrence rate, because ductal remnants are intimately adherent to the hyoid bone. The Sistrunk operation achieves cure in >90% of cases.
Sources: The Developing Human: Clinically Oriented Embryology (Moore & Persaud); Schwartz's Principles of Surgery, 11e; Mulholland & Greenfield's Surgery, 7e; Sabiston Textbook of Surgery; Robbins & Cotran Pathologic Basis of Disease
This is a shared conversation. Sign in to Orris to start your own chat.