Steroid synthesis Thyroid synthesis Thyroid Function tests P th calcium metabolism Ca and phhos Insulin stru also receptor Glucagon Somatostatin Glut transporters Role of c peptide Lab diag of dm Oral glucose Hba1 c Glucagon receptors Metabolism of insulin, glucagon all metabolism Somatostatin metabolism explain me biochemstry of this topic like i dont know anything each and every topic explain me clearly
You are a medical biochemistry expert. Search the medical textbook library database and retrieve detailed content on these topics: 1. Steroid hormone synthesis (cholesterol to steroid hormones, steroidogenesis pathway) 2. Thyroid hormone synthesis (iodine trapping, organification, coupling, T3/T4 formation) 3. Thyroid function tests (TSH, T3, T4, free T4, TRH stimulation, interpretation) Use query_library_db with FTS searches like: - SELECT book_title, section_heading, '/textbooks/' || block_file_path AS file_path, line_start, line_end, snippet(paragraphs_fts, 0, '>>>', '<<<', '...', 40) as snippet FROM paragraphs_fts WHERE paragraphs_fts MATCH 'steroid synthesis cholesterol' ORDER BY rank LIMIT 5 - Similarly for 'thyroid hormone synthesis iodination' - Similarly for 'thyroid function tests TSH T3 T4' - Similarly for 'steroidogenesis pathway cortisol aldosterone' Then read the actual file blocks using read_file with the paths and line numbers returned. Read at least 100-150 lines per block for each topic. Return a DETAILED summary of everything you find for each of the 3 topics - mechanisms, pathways, enzymes, clinical significance. Include exact biochemical steps.
🧬 COMPLETE BIOCHEMISTRY GUIDE: Hormones, Metabolism & Diabetes
PART 1: STEROID HORMONE SYNTHESIS
What is a steroid hormone? Start from scratch.
Where are they made?
| Gland/Organ | Hormones Produced |
|---|---|
| Adrenal Cortex (outer layer) | Cortisol, Aldosterone, DHEA |
| Testes (Leydig cells) | Testosterone |
| Ovaries (granulosa cells) | Estrogen, Progesterone |
| Placenta | Progesterone, Estriol |
The Big Picture Pathway
CHOLESTEROL (C27)
↓ [RATE-LIMITING STEP: StAR protein moves cholesterol into mitochondria]
↓ [Enzyme: CYP11A1 = P450scc, in inner mitochondrial membrane]
PREGNENOLONE ← This is the "mother of all steroids"
↓ [3β-HSD enzyme, in smooth ER]
PROGESTERONE
↓ splits into 3 pathways based on which zone of adrenal gland
┌───┴────────────────────────────┐
↓ ↓ ↓
GLUCOCORTICOIDS MINERALOCORTICOIDS ANDROGENS/ESTROGENS
(Zona Fasciculata) (Zona Glomerulosa) (Zona Reticularis)
CORTISOL ALDOSTERONE DHEA → Testosterone → Estradiol
Step-by-Step: Cholesterol to Each Hormone
Step 1 - The Rate-Limiting Step
- StAR protein (Steroidogenic Acute Regulatory protein) physically shuttles cholesterol from the outer to the inner mitochondrial membrane
- This is the first thing ACTH triggers - no StAR activity = no steroid synthesis
- Think of StAR as the "gate opener" - without it, the raw material (cholesterol) can't enter the factory (mitochondria)
Step 2 - Cholesterol → Pregnenolone
- Enzyme: P450scc (CYP11A1) - "scc" = side chain cleavage
- It snips off a 6-carbon piece from cholesterol (C27) to make pregnenolone (C21)
- Needs: NADPH + Oxygen
- Location: Inner mitochondrial membrane
Step 3 - Pregnenolone → Progesterone
- Enzyme: 3β-HSD (3-beta hydroxysteroid dehydrogenase) + isomerase
- Converts the Δ5 compound (pregnenolone) into a Δ4 compound (progesterone)
- Location: Smooth endoplasmic reticulum
Now the 3 Pathways Diverge:
Pathway A - CORTISOL (Zona Fasciculata - stress hormone)
Progesterone
↓ CYP17A1 (17α-hydroxylase) - adds OH at C17
17α-Hydroxyprogesterone (17-OHP)
↓ CYP21A2 (21-hydroxylase) - adds OH at C21
11-Deoxycortisol
↓ CYP11B1 (11β-hydroxylase) - adds OH at C11, in mitochondria
CORTISOL ✓
- Important exam fact: CYP21A2 deficiency = most common CAH (Congenital Adrenal Hyperplasia). If you can't make cortisol/aldosterone, all precursors flood into the androgen pathway → virilization + salt-wasting crisis.
Pathway B - ALDOSTERONE (Zona Glomerulosa - salt hormone)
Progesterone
↓ CYP21A2 (21-hydroxylase)
11-Deoxycorticosterone (DOC)
↓ CYP11B1 (11β-hydroxylase)
Corticosterone
↓ CYP11B2 (Aldosterone synthase) ← ONLY exists in zona glomerulosa!
ALDOSTERONE ✓
- Key: Zona glomerulosa lacks CYP17A1 (17α-hydroxylase) so it can't make cortisol or androgens - it's wired only for aldosterone.
Pathway C - ANDROGENS/ESTROGENS (Zona Reticularis + Gonads)
17-Hydroxypregnenolone
↓ CYP17A1 (now acting as 17,20-lyase - second function)
DHEA (C19 - weak androgen)
↓ 3β-HSD
Androstenedione
↓ 17β-HSD (in gonads)
TESTOSTERONE
↓ CYP19A1 (Aromatase) in ovarian granulosa cells
ESTRADIOL (C18 - most potent estrogen)
OR
↓ 5α-Reductase in prostate/skin
DHT (Dihydrotestosterone - most potent androgen)
Carbon Number Rule (Easy Memory)
- C21 = Glucocorticoids (cortisol) + Mineralocorticoids (aldosterone) + Progestogens
- C19 = Androgens (testosterone, DHEA)
- C18 = Estrogens (estradiol) - have aromatic ring A
Regulation - Who Controls All This?
PART 2: THYROID HORMONE SYNTHESIS
What are thyroid hormones?
- T4 (Thyroxine) = 4 iodine atoms, made exclusively in thyroid, is a prohormone (not very active)
- T3 (Triiodothyronine) = 3 iodine atoms, the active hormone, 80% comes from peripheral conversion of T4
The 6 Steps of Thyroid Hormone Synthesis
Where it happens
BLOOD (Iodide I⁻) → [STEP 1: TRAPPING] → Inside thyrocyte → [STEP 3: ORGANIFICATION]
→ COLLOID (Thyroglobulin + Iodine) → [STEP 4: COUPLING] → T4/T3 stored on Tg
→ [STEP 5: SECRETION] → Free T4/T3 released into blood
→ [STEP 6: PERIPHERAL CONVERSION] → T4 → T3 in liver/kidney
Step 1 - Iodide Trapping (Active Transport)
- Transporter: NIS (Sodium-Iodide Symporter) on the basolateral membrane (blood side)
- Brings 2 Na⁺ + 1 I⁻ into the cell together (symport)
- Concentrates iodide 20-40 times higher inside the cell than in blood
- Driven by the Na⁺ gradient (created by Na/K-ATPase)
- Pendrin transports I⁻ from cell into the colloid (apical membrane)
- Regulated by: TSH increases NIS activity; excess iodine inhibits it (Wolff-Chaikoff effect)
Step 2 - Thyroglobulin Synthesis
- Thyroglobulin (660 kDa glycoprotein) made in rough ER of thyrocyte
- Processed in Golgi, then secreted by exocytosis into the colloid
- Contains 123 tyrosine residues, but only 4-8 will actually become thyroid hormones
- Think of Tg as a "tyrosine delivery board" waiting to be iodinated
Step 3 - Organification of Iodide
- Enzyme: TPO (Thyroid Peroxidase) at the apical membrane (colloid side)
- TPO uses H₂O₂ (made by DUOX2 enzyme) to oxidize I⁻ → reactive iodine (I⁰)
- Reactive iodine attaches to tyrosine residues on Tg:
- One iodine added → MIT (Monoiodotyrosine)
- Two iodines added → DIT (Diiodotyrosine)
- Blocked by: Propylthiouracil (PTU), Methimazole (anti-thyroid drugs)
Step 4 - Coupling (Making T3 and T4)
- Same enzyme: TPO catalyzes coupling
- Two iodinated tyrosines join together on the Tg scaffold:
- DIT + DIT → T4 (thyroxine, 4 iodines) - most abundant
- MIT + DIT → T3 (3,5,3′-triiodothyronine, 3 iodines) - active form
- DIT + MIT → rT3 (reverse T3, biologically inactive)
- This all happens while tyrosines are still attached to thyroglobulin
Step 5 - Secretion
- TSH stimulates thyrocytes to endocytose (eat) the colloid
- Colloid vesicles fuse with lysosomes → proteases digest thyroglobulin
- Free T4 and T3 are released and diffuse into the bloodstream
- MIT and DIT are NOT secreted - iodotyrosine deiodinase strips their iodine off and recycles it back into new hormone synthesis
Step 6 - Peripheral Conversion (T4 → T3)
- T4 is a prohormone; it must be converted to T3 to be active
- 80% of circulating T3 comes from this conversion in liver, kidney, muscle
- Deiodinases contain selenocysteine (selenium):
| Enzyme | Location | Makes |
|---|---|---|
| D1 | Liver, kidney, thyroid | T3 (main circulating T3 source) |
| D2 | Brain, pituitary, brown fat | Local T3 (especially in brain) |
| D3 | Brain, placenta | Inactive rT3 (inactivates T4) |
How Thyroid Hormones Work (Receptor Mechanism)
- T3 enters the cell → binds nuclear thyroid hormone receptor (TR)
- TR-T3 complex binds to Thyroid Hormone Response Elements (TREs) in DNA
- Results: Upregulates genes for metabolic enzymes, Na/K-ATPase, cardiac proteins, growth hormones
Transport in Blood
- TBG (Thyroxine-binding globulin) - binds 67% of T4, 46% of T3
- Transthyretin - binds 20% of T4
- Albumin - binds 13% of T4, 53% of T3
- Only the free fraction (0.02% of T4, 0.2% of T3) is biologically active
HPT Axis (Regulation)
Hypothalamus: TRH (tripeptide)
↓
Anterior Pituitary (thyrotrophs): TSH (glycoprotein, α+β subunits)
↓
Thyroid Gland: T4 (mainly) + small T3
↑ Negative feedback (free T3/T4 suppress both TRH and TSH)
PART 3: THYROID FUNCTION TESTS
Why do we test thyroid function?
The Tests - One by One
1. TSH (Thyroid-Stimulating Hormone)
- Normal range: 0.35-5.0 mIU/L
- The most sensitive test for thyroid dysfunction
- HIGH TSH = thyroid is failing = the pituitary is screaming louder = Primary Hypothyroidism
- LOW TSH = thyroid is overactive = the pituitary is quiet = Primary Hyperthyroidism
- Exception: If the pituitary itself is diseased (central hypothyroidism), TSH may be low despite low T4 - always check TSH + FT4 together if you suspect pituitary disease
2. Free T4 (FT4)
- Normal range: 12-28 pmol/L (0.8-2.4 ng/dL)
- Measures only the unbound, biologically active T4
- More reliable than Total T4 because it's not affected by binding protein changes (e.g., pregnancy raises TBG → raises Total T4 but Free T4 stays normal)
3. Free T3 (FT3)
- Normal range: 3-9 pmol/L
- Used when: T3 toxicosis suspected (patient is hyperthyroid with normal FT4 but elevated FT3)
4. Total T4 and Total T3
- Measures bound + free hormone
- Less useful because binding protein changes confuse the results
- Estrogen (pregnancy, OCP) → ↑ TBG → ↑ Total T4/T3 (but patient is euthyroid, FT4 normal!)
- Androgens, glucocorticoids → ↓ TBG → ↓ Total T4/T3 (but patient is still euthyroid)
5. Reverse T3 (rT3)
- Elevated rT3 + Low T3 + Normal T4 = Euthyroid Sick Syndrome (nonthyroidal illness)
- In critical illness, starvation, major surgery: the body shunts T4 away from T3 (active) toward rT3 (inactive) to conserve energy
6. TRH Stimulation Test
- Inject 500 μg TRH IV → measure TSH at 0, 30, 60 min
- Normal: TSH rises by ≥6 mIU/L at 30 min
- Blunted response: primary hyperthyroidism OR pituitary disease
- Exaggerated response: primary hypothyroidism
- Largely replaced by modern sensitive TSH assays
7. Thyroid Antibodies
- Anti-TPO (aTPO): Positive in Hashimoto's (>80%) and Graves' disease
- TSI (Thyroid-Stimulating Immunoglobulin): Diagnostic for Graves' disease - these antibodies mimic TSH and stimulate the gland continuously
- Anti-thyroglobulin (ATG): Hashimoto's; also interferes with Tg measurements used in thyroid cancer monitoring
Interpretation Table (Memorize This)
| Condition | TSH | FT4 | FT3 |
|---|---|---|---|
| Primary Hyperthyroidism | ↓↓ | ↑ | ↑ |
| T3 Toxicosis | ↓ | Normal | ↑↑ |
| Subclinical Hyperthyroidism | ↓ | Normal | Normal |
| Primary Hypothyroidism | ↑↑ | ↓ | ↓ |
| Subclinical Hypothyroidism | ↑ | Normal | Normal |
| Central (Pituitary) Hypothyroidism | ↓ or Normal | ↓ | ↓ |
| Graves' disease | ↓ | ↑ | ↑ |
| Euthyroid Sick Syndrome | Variable ↓ | ↓ | ↓↓ |
| Pregnancy (↑TBG) | Normal | Normal FT4 | Total T4 ↑↑ |
PART 4: PTH AND CALCIUM METABOLISM
Why is calcium so important?
- Muscle contraction (including heart muscle)
- Nerve impulse transmission
- Blood clotting (coagulation cascade)
- Cell signaling (second messenger)
- Enzyme activation
Three Organs Control Calcium: Bone, Kidney, Intestine
- PTH (Parathyroid Hormone) - raises calcium
- Calcitriol (1,25-(OH)₂-Vitamin D) - raises calcium
- Calcitonin - lowers calcium (minor role in adults)
PTH: The Emergency Calcium Raiser
Structure
- PTH is an 84 amino acid polypeptide made by chief cells of the 4 parathyroid glands (tiny glands behind the thyroid)
- The biologically active portion is the first 34 amino acids (N-terminal)
What triggers PTH release?
- Low blood Ca²⁺ → chief cells detect this via CaSR (Calcium-Sensing Receptor) on their surface
- Low Ca²⁺ → CaSR inactive → PTH released
- High Ca²⁺ → CaSR activated → PTH suppressed
PTH's 3 Target Actions
| Target | Action | Effect |
|---|---|---|
| Bone | Activates osteoclasts (bone breakers) | Releases Ca²⁺ AND PO₄³⁻ from bone |
| Kidney (DCT) | Increases Ca²⁺ reabsorption; DECREASES PO₄³⁻ reabsorption (phosphaturic effect) | Saves Ca²⁺, loses PO₄³⁻ |
| Kidney (PCT) | Activates 1α-hydroxylase → converts 25-OH-Vitamin D to 1,25-(OH)₂-Vitamin D (Calcitriol) | Indirectly increases intestinal Ca²⁺ absorption |
PTH Mechanism of Action
- PTH receptor (PTH1R) is a GPCR (G-protein coupled receptor)
- Binds PTH → activates Gs → cAMP ↑ → PKA activation
- Also activates Gq → PLC → IP₃ → Ca²⁺ release + PKC activation
Vitamin D - The Intestinal Calcium Hero
Activation Pathway
Skin: UV light + 7-dehydrocholesterol → Cholecalciferol (Vitamin D3)
↓ Liver: 25-hydroxylase
25-hydroxyvitamin D (Calcidiol) ← this is what you measure in blood tests!
↓ Kidney: 1α-hydroxylase (activated by PTH, low PO₄, low Ca)
1,25-dihydroxyvitamin D (Calcitriol) ← the ACTIVE form
Actions of Calcitriol
- Intestine: Increases synthesis of calbindin-D (calcium transport protein) and TRPV6 channels → increases Ca²⁺ absorption (up to 80% of dietary calcium!)
- Bone: At normal levels, promotes bone mineralization; at high levels, works with PTH to release Ca from bone
- Kidney: Mild increase in Ca²⁺ reabsorption
- Parathyroid gland: Suppresses PTH synthesis (negative feedback)
Calcitonin - The Bone Protector
- Made by C-cells (parafollicular cells) of the thyroid gland
- Released when Ca²⁺ is HIGH
- Actions: Inhibits osteoclasts → reduces bone resorption; increases renal Ca excretion
- Clinical note: Calcitonin's role in adult humans is minor; it's more important in growing children and pregnant/lactating women. Used therapeutically in Paget's disease and hypercalcemia.
Calcium and Phosphate - The Inverse Relationship
- In hyperparathyroidism: Ca ↑, PO₄ ↓
- In hypoparathyroidism: Ca ↓, PO₄ ↑
- In Vitamin D toxicity: Both Ca AND PO₄ rise (because Vit D raises both)
- In Chronic Kidney Disease: Kidneys can't make calcitriol + can't excrete PO₄ → PO₄ ↑, Ca ↓ → Secondary hyperparathyroidism
Phosphate Regulation Summary
| Hormone | Effect on Blood Phosphate | Mechanism |
|---|---|---|
| PTH | ↓ (phosphaturia) | Inhibits NaPi cotransporter in kidney PCT |
| Calcitriol | ↑ | Increases intestinal PO₄ absorption |
| FGF-23 (from bone) | ↓↓ | Major phosphaturic hormone; also inhibits 1α-hydroxylase |
PART 5: INSULIN - STRUCTURE AND RECEPTOR
What is insulin? The basics.
- α cells (25%) - make Glucagon
- β cells (60%) - make Insulin
- δ cells (10%) - make Somatostatin
- PP cells (5%) - make Pancreatic polypeptide
Insulin Structure - Built Like a Two-Strand Rope
- Molecular weight: 5,808 Da
- Two chains: A chain (21 amino acids) + B chain (30 amino acids)
- Connected by: 2 disulfide bonds (between chains) + 1 within the A chain
- If you split the two chains apart, insulin completely loses its activity
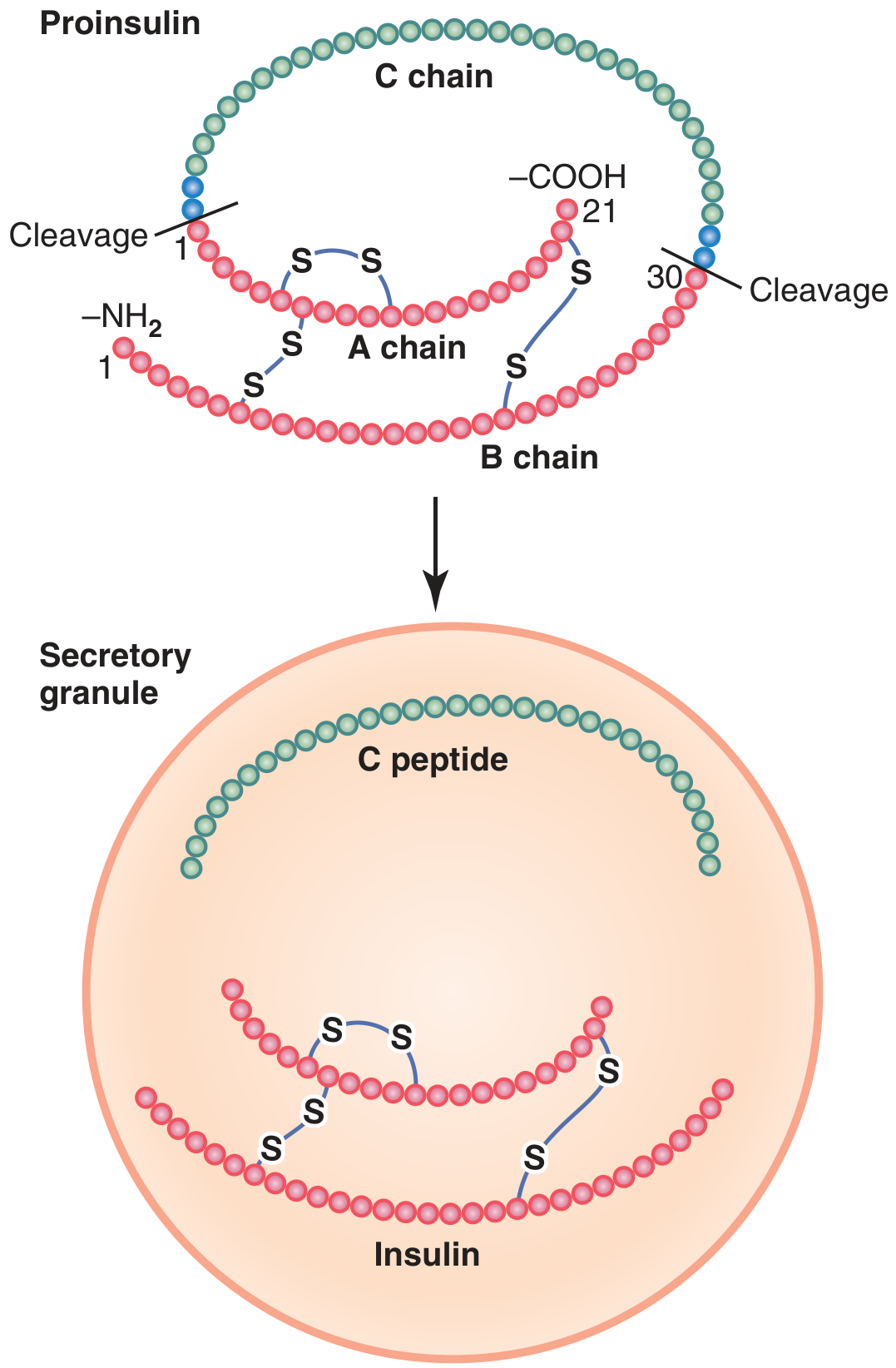
How Insulin is Made - The Biosynthesis Pathway
Gene on chromosome 11
↓ Transcription + Translation on ribosomes (RER)
PREPROINSULIN (110 amino acids, MW ~11,500)
↓ Signal peptide cleaved in ER lumen
PROINSULIN (86 amino acids, MW ~9,000) = A chain + B chain + C peptide
↓ Packaged in Golgi vesicles
↓ Cleavage by prohormone convertases (PC1 and PC2) + CPE
INSULIN (A+B chains, MW 5,808) + C PEPTIDE (31 amino acids)
↓ Both secreted together in equimolar amounts from secretory granules
What is C-Peptide? (Role of C-Peptide)
- Diagnostic use: Injected insulin has no C-peptide. So if a diabetic patient has high insulin but low C-peptide, they're injecting insulin (factitious hypoglycemia or insulin misuse). If insulin AND C-peptide are both high, the body is making too much insulin (insulinoma).
- Beta cell function marker: C-peptide measurement tells you how much insulin the pancreas is making. Because C-peptide has a longer half-life (~35 min vs. ~5 min for insulin), it's easier to measure.
- Biological activity: C-peptide binds a G-protein-coupled receptor and activates Na/K-ATPase and endothelial nitric oxide synthase (eNOS) → may protect against diabetic nephropathy and neuropathy. This biological role is still being studied.
Insulin Secretion - How Does Glucose Trigger It?
Glucose enters β-cell via GLUT2 (passive)
↓
Glucokinase (Hexokinase IV) phosphorylates glucose → Glucose-6-phosphate
↓
Glycolysis + TCA cycle → ATP production
↓
↑ ATP/ADP ratio
↓
ATP-sensitive K⁺ channel (KATP channel) CLOSES
↓
β-cell membrane DEPOLARIZES (K⁺ can't leave)
↓
Voltage-gated Ca²⁺ channels OPEN
↓
Ca²⁺ floods into β-cell
↓
Insulin granules FUSE with membrane → EXOCYTOSIS of insulin + C-peptide
- Phase 1 (First phase, 3-5 min): Rapid dump of pre-stored insulin granules (immediate response to glucose rise)
- Phase 2 (15 min to 2 hrs): Slower, sustained secretion from newly synthesized + stored insulin
The Insulin Receptor - How Insulin Acts
Structure
- Heterotetramer: 2α subunits (extracellular, bind insulin) + 2β subunits (transmembrane + intracellular kinase domain)
- Connected by disulfide bonds
Signal Transduction Cascade
Insulin binds to α subunit
↓
Conformational change activates β subunit tyrosine kinase
↓
β subunit AUTOPHOSPHORYLATES (phosphorylates itself on tyrosine residues)
↓
Phosphorylates IRS-1/IRS-2 (Insulin Receptor Substrate proteins)
↓
┌─────────────────────────────┐
↓ ↓
PI3K → PIP3 → PDK1 → Akt Grb2/SOS → Ras → Raf → MEK → ERK
(Metabolic effects: (Mitogenic effects:
GLUT4 translocation, cell growth,
glycogen synthesis, gene expression,
lipogenesis, differentiation)
protein synthesis)
PART 6: GLUCAGON
What is glucagon? The opposite of insulin.
- Insulin = fed state hormone (glucose ↑ → insulin ↑ → store energy)
- Glucagon = fasting state hormone (glucose ↓ → glucagon ↑ → release energy)
Glucagon Structure
- 29 amino acid polypeptide
- Made from proglucagon (158 amino acids) gene
- Same proglucagon gene, but processed differently in intestinal L-cells → makes GLP-1 (glucagon-like peptide 1) instead
What Stimulates Glucagon?
| Stimulates Glucagon | Inhibits Glucagon |
|---|---|
| Low blood glucose (hypoglycemia) | High blood glucose |
| Amino acids (especially alanine, arginine) | Insulin |
| Fasting, exercise, stress | Somatostatin |
| Epinephrine (α2-adrenergic) | Free fatty acids |
| Cortisol | GLP-1 |
Glucagon Receptor and Mechanism
Glucagon binds glucagon receptor on hepatocyte
↓
Gαs protein activates Adenylyl Cyclase
↓
ATP → cAMP ↑↑
↓
Protein Kinase A (PKA) activated
↓ (phosphorylates multiple enzymes simultaneously)
┌────────────────────────────────────────────┐
↓ ↓
GLYCOGENOLYSIS GLUCONEOGENESIS
(glycogen phosphorylase activated; (PEP carboxykinase,
phosphofructokinase-2 inhibited) fructose-1,6-bisphosphatase activated)
↓ ↓
Glucose released from glycogen New glucose made from
into blood amino acids, lactate, glycerol
- Lipolysis: Activates hormone-sensitive lipase → releases fatty acids from adipose
- Ketogenesis: Promotes fatty acid oxidation → acetyl-CoA → ketone bodies in liver
- Protein catabolism: Promotes amino acid release from muscle for gluconeogenesis
Glucagon Metabolism (How is it broken down?)
- Half-life: 3-6 minutes
- Degraded primarily by: liver (first pass, ~60% removed) and kidneys
- Mechanism: Proteolytic degradation by liver proteases and renal clearance
- The short half-life means glucagon levels change very quickly in response to blood glucose
PART 7: SOMATOSTATIN
What is somatostatin? The "off switch."
- δ (delta) cells of the pancreatic islets
- D cells of the stomach and intestine
- Hypothalamus (inhibits growth hormone from pituitary)
Structure
- Two forms: SS-14 (14 amino acids) and SS-28 (28 amino acids)
- Both are cyclic peptides (amino and carboxy termini linked by a disulfide bridge)
- SS-14 predominates in pancreas; SS-28 predominates in intestine
What Triggers Somatostatin Release?
- High glucose, amino acids, fatty acids after a meal
- Other GI hormones (CCK, secretin)
- High glucagon or insulin (local paracrine effect)
Somatostatin's Effects - "SOMATOSTATIN Stops Everything"
| Target | Effect |
|---|---|
| Pancreatic β cells | Inhibits insulin secretion |
| Pancreatic α cells | Inhibits glucagon secretion |
| Pituitary | Inhibits GH (growth hormone) and TSH release |
| Stomach | Inhibits gastrin, HCl, pepsin secretion |
| Intestine | Inhibits secretin, CCK, VIP, motilin |
| Liver | Inhibits bile flow |
| GI motility | Slows gastric emptying, reduces splanchnic blood flow |
Mechanism of Action
- Somatostatin receptors (SSTR1-5) are GPCRs coupled to Gi (inhibitory G-protein)
- Gi → inhibits adenylyl cyclase → cAMP ↓ → PKA activity ↓
- Also: Opens K⁺ channels → hyperpolarization → inhibits Ca²⁺ entry → inhibits exocytosis
- In α and β cells: the reduced cAMP + hyperpolarization directly suppresses hormone granule release
Somatostatin Metabolism
- Half-life: extremely short, ~1-3 minutes in circulation
- Degraded by peptidases in the blood and tissues
- This is why octreotide (a synthetic analog with half-life 1.5 hours) and lanreotide (long-acting, monthly injection) were developed for clinical use
- Clinical uses: acromegaly (excess GH), carcinoid tumors, VIPomas, glucagonomas, bleeding esophageal varices
PART 8: GLUT TRANSPORTERS
What are GLUT transporters?
The Key GLUT Transporters - A Complete Table
| GLUT | Location | Km for Glucose | Characteristics | Regulation |
|---|---|---|---|---|
| GLUT1 | RBCs, brain (blood-brain barrier), placenta, all fetal tissues | 1 mM (low Km = high affinity) | Constitutive (always on surface); baseline glucose transport; not regulated by insulin | Constitutive |
| GLUT2 | Liver, pancreatic β-cells, kidney, small intestine | 15-20 mM (high Km = low affinity) | "Glucose sensor" - only transports glucose when it's abundant; allows liver to buffer post-meal glucose; essential for insulin secretion trigger | Not regulated by insulin |
| GLUT3 | Neurons (brain) | 1 mM (high affinity) | Ensures neurons ALWAYS get glucose even when levels fall | Constitutive |
| GLUT4 | Skeletal muscle, cardiac muscle, adipose tissue | 5 mM | The insulin-regulated transporter - stored in intracellular vesicles; moves to surface when insulin signals | Insulin-dependent! |
| GLUT5 | Small intestine (enterocytes), sperm | High Km | Fructose transporter (not glucose) | Constitutive |
The Magic of GLUT4 - Why Insulin Matters
- GLUT4 vesicles sit in the cytoplasm, docked to intracellular membranes
- Very few GLUT4 molecules on the cell surface
- Little glucose enters muscle/fat cells
Insulin → IR → IRS-1 → PI3K → PIP3 → Akt → phosphorylates AS160
↓
TBC1D4 (AS160) is inactivated
↓
Rab-GTPase proteins activated
↓
GLUT4 vesicles traffic to plasma membrane
↓
GLUT4 fuses with membrane (exocytosis)
↓
GLUT4 on surface increases 10-20 fold
↓
Glucose floods into muscle/fat cell
PART 9: LABORATORY DIAGNOSIS OF DIABETES MELLITUS
ADA Diagnostic Criteria (any ONE of these criteria on TWO separate days):
| Test | Diabetes | Prediabetes | Normal |
|---|---|---|---|
| Fasting Plasma Glucose (FPG) | ≥ 126 mg/dL (7.0 mmol/L) | 100-125 mg/dL (IFG) | < 100 mg/dL |
| 2-hr Plasma Glucose (OGTT) | ≥ 200 mg/dL (11.1 mmol/L) | 140-199 mg/dL (IGT) | < 140 mg/dL |
| HbA1c | ≥ 6.5% (48 mmol/mol) | 5.7-6.4% | < 5.7% |
| Random Plasma Glucose | ≥ 200 mg/dL WITH symptoms (polyuria, polydipsia, weight loss) | - | - |
Oral Glucose Tolerance Test (OGTT) - In Detail
Procedure
- Preparation: Patient fasts for 8-14 hours overnight; no heavy exercise 3 days prior; normal carbohydrate diet (≥150g/day) for 3 days prior
- Fasting blood sample taken
- Patient drinks 75g anhydrous glucose dissolved in 250-300 mL water (within 5 minutes)
- Blood samples taken at 1 hour and 2 hours
- Patient sits quietly, no smoking during test
Interpretation
| 2-hour value | Interpretation |
|---|---|
| < 140 mg/dL | Normal glucose tolerance |
| 140-199 mg/dL | IGT (Impaired Glucose Tolerance) = Prediabetes |
| ≥ 200 mg/dL | Diabetes Mellitus |
Why is OGTT used?
- Better than FPG for detecting early Type 2 DM
- Essential for diagnosing Gestational Diabetes Mellitus (GDM)
- Reveals glucose regulation under physiological stress (a real meal)
- 2-step approach (USA): 50g glucose screen at 24-28 weeks → if ≥130-140 mg/dL at 1hr → do 100g 3-hr OGTT
- 1-step approach (international): 75g OGTT directly; GDM if fasting ≥92, 1-hr ≥180, 2-hr ≥153 mg/dL
PART 10: HbA1c (GLYCATED HEMOGLOBIN)
What is HbA1c?
High blood glucose + Hemoglobin A
↓ (non-enzymatic, irreversible, SLOW process)
Schiff base (unstable)
↓ Amadori rearrangement
HbA1c (stable ketoamine)
Why does HbA1c reflect 3-month glucose control?
- RBCs (red blood cells) live for approximately 120 days (3 months)
- As the RBC is born, it has zero HbA1c
- Every day it lives, more glucose attaches to hemoglobin
- The amount of HbA1c at the end reflects the average glucose the RBC has been exposed to over its entire lifetime
- HbA1c is a "memory" of blood glucose for the past 2-3 months
- It reflects the last 30 days more heavily than earlier months (because younger RBCs are more abundant)
Reference Values
| HbA1c | Interpretation |
|---|---|
| < 5.7% | Normal |
| 5.7 - 6.4% | Prediabetes |
| ≥ 6.5% | Diabetes mellitus (diagnostic) |
| Target < 7% | Diabetic treatment goal (ADA guideline) |
| > 8% | Poor control, risk of complications |
How HbA1c Correlates to Average Blood Glucose
| HbA1c | Estimated Average Glucose (eAG) |
|---|---|
| 6% | 126 mg/dL |
| 7% | 154 mg/dL |
| 8% | 183 mg/dL |
| 9% | 212 mg/dL |
| 10% | 240 mg/dL |
Conditions That Falsely Alter HbA1c
| Condition | Effect on HbA1c | Reason |
|---|---|---|
| Hemolytic anemia | ↓ False low | RBCs destroyed faster → less time for glycation |
| Iron deficiency anemia | ↑ False high | RBCs live longer → more time for glycation |
| Hemoglobin variants (HbS, HbC, HbE) | Unreliable | Interfere with assay |
| Pregnancy (2nd/3rd trimester) | ↓ False low | Increased RBC turnover |
| Blood transfusion | ↓ False low | Dilutes patient's own RBCs |
| High-dose vitamin C/E | ↓ False low | Inhibit glycation |
PART 11: METABOLISM OF INSULIN, GLUCAGON, AND SOMATOSTATIN
Insulin Metabolism
Secretion
- Normal fasting insulin: 5-15 μU/mL (35-105 pmol/L)
- After a meal: peaks at 50-100 μU/mL
- Daily secretion: ~40-50 units/day
Half-Life
- ~5-8 minutes in circulation (very short!)
Degradation
- Liver - most important site (~50% of portal insulin removed in FIRST PASS through liver before it even reaches systemic circulation)
- Kidneys - second most important (~30-40% of peripheral insulin)
- Muscle, adipose - minor
Mechanism of Degradation
- Insulin-degrading enzyme (IDE) = insulysin - a zinc metalloprotease
- IDE degrades insulin in the cytosol after receptor-mediated endocytosis
- Also, insulin-receptor complex is internalized → insulin degraded in lysosomes → receptor recycled to surface
Why does this matter clinically?
- Kidney disease → insulin half-life prolonged → LESS insulin needed (risk of hypoglycemia)
- Liver disease → reduced first-pass extraction → HIGHER systemic insulin levels
Glucagon Metabolism
Secretion
- Normal fasting glucagon: 75-150 pg/mL
- After protein meal: rises significantly
- During hypoglycemia: rises markedly (key counter-regulatory response)
Half-Life
- 3-6 minutes (even shorter than insulin)
Degradation
- Liver is the primary site (60% removed in first pass)
- Kidneys are secondary
- Mechanism: Proteolytic degradation by liver enzymes + renal clearance
- This rapid degradation means glucagon works quickly but briefly - perfect for the acute hypoglycemia response
Somatostatin Metabolism
Secretion
- SS-14 predominates in pancreatic δ cells
- SS-28 predominates in intestinal D cells and hypothalamus
Half-Life
- Remarkably short: 1-3 minutes
- This is why it mainly acts locally (paracrine) rather than as a true circulating hormone
Degradation
- Peptidases in plasma (mainly endopeptidases)
- Liver and kidney clearance
- Clinical consequence: The natural hormone is useless therapeutically → synthetic analogs needed:
- Octreotide (t½ ~1.5 hours, SubQ injection 3x/day)
- Lanreotide (depot injection, monthly)
- Pasireotide (broader SSTR subtype binding, used in Cushing's)
QUICK REFERENCE SUMMARY TABLE
| Hormone | Made by | Chemical nature | Receptor type | Half-life | Main action |
|---|---|---|---|---|---|
| Cortisol | Adrenal zona fasciculata | Steroid (C21) | Nuclear | 60-90 min | Gluconeogenesis, anti-inflammatory |
| Aldosterone | Adrenal zona glomerulosa | Steroid (C21) | Nuclear | 15-20 min | Na⁺ retention, K⁺ excretion |
| Testosterone | Testes (Leydig cells) | Steroid (C19) | Nuclear | 2-4 hours | Virilization, anabolism |
| Estradiol | Ovaries (granulosa) | Steroid (C18) | Nuclear | 1-2 hours | Female reproductive |
| T4 (Thyroxine) | Thyroid follicular cells | Iodinated amino acid | Nuclear (after → T3) | 6-7 days | Metabolic rate (prohormone) |
| T3 | Peripheral conversion | Iodinated amino acid | Nuclear | 18 hours | Metabolic rate (active) |
| PTH | Parathyroid chief cells | Polypeptide (84 AA) | GPCR (Gs+Gq) | 2-4 min | Raise blood calcium |
| Insulin | Pancreatic β cells | Polypeptide (51 AA) | Receptor tyrosine kinase | 5-8 min | Lower blood glucose, anabolic |
| Glucagon | Pancreatic α cells | Polypeptide (29 AA) | GPCR (Gs → cAMP) | 3-6 min | Raise blood glucose, catabolic |
| Somatostatin | Pancreatic δ cells | Cyclic peptide (14 or 28 AA) | GPCR (Gi → ↓cAMP) | 1-3 min | Inhibit insulin, glucagon, GH |
Key Concepts to Always Remember
- All steroid hormones come from cholesterol; the rate-limiting step is StAR protein moving cholesterol into mitochondria.
- Thyroid hormone synthesis needs iodine + TPO enzyme; T4 is a prohormone, T3 is active.
- TSH is the most sensitive thyroid test; low TSH = overactive gland, high TSH = underactive gland.
- PTH raises calcium AND lowers phosphate; Vitamin D raises both.
- Insulin is made as preproinsulin → proinsulin → insulin + C-peptide (released in equal amounts).
- GLUT2 is the glucose sensor in β cells (low affinity, high capacity); GLUT4 is insulin-regulated in muscle/fat.
- C-peptide helps distinguish endogenous insulin production from exogenous injection.
- HbA1c reflects average blood glucose over 120 days (RBC lifespan); ≥6.5% = diabetes.
- Glucagon → GPCR → cAMP → PKA → glycogenolysis + gluconeogenesis.
- Somatostatin = master inhibitor of both insulin and glucagon via Gi → ↓cAMP pathway; half-life 1-3 minutes.
Make a presentation on clinical diagnosis and management of thyroid disorders step-by-step
ls /home/daytona/workspace/ 2>/dev/null && mkdir -p /home/daytona/workspace/thyr…
~/thyroid-pptx/build.js
const pptxgen = require("pptxgenjs");
const pres = new pptxgen();
pres.layout = "LAYOUT_WIDE";
pres.title = "Clinical Diagnosis & Management of Thyroid Disorders";
pres.author = "Medical Biochemistry";
// ── Palette ──────────────────────────────────────────────────────────────────
const C = {
navy: "0D2B55", // dominant dark
teal: "0F7D8C", // accent 1
sky: "38B2C0", // accent 2 (lighter)
mint: "D0F0F4", // light bg tint
amber: "E8963A", // warm accent / highlight
white: "FFFFFF",
offWhite:"F5F8FA",
text: "1A2E3F",
sub: "4A6578",
lightGray:"E2E8F0",
red: "D94F4F",
green: "2D9B5A",
orange: "E07A2F",
};
// ── Shared Helpers ────────────────────────────────────────────────────────────
function darkSlide(slide) {
slide.addShape(pres.shapes.RECTANGLE, { x:0, y:0, w:13.3, h:7.5, fill:{ color: C.navy }, line:{ color: C.navy } });
}
function accentBar(slide, color=C.teal, h=0.08) {
slide.addShape(pres.shapes.RECTANGLE, { x:0, y:7.42-h, w:13.3, h:h+0.1, fill:{ color: color }, line:{ color: color } });
}
function sectionHeader(slide, title, sub="") {
darkSlide(slide);
// left teal bar
slide.addShape(pres.shapes.RECTANGLE, { x:0, y:0, w:0.4, h:7.5, fill:{ color: C.teal }, line:{ color: C.teal } });
slide.addText(title, { x:0.7, y:2.5, w:11.5, h:1.3, fontSize:40, bold:true, color:C.white, fontFace:"Calibri Light" });
if (sub) slide.addText(sub, { x:0.7, y:3.85, w:11.5, h:0.8, fontSize:20, color:C.sky, fontFace:"Calibri" });
accentBar(slide, C.amber);
}
function contentSlide(slide) {
slide.addShape(pres.shapes.RECTANGLE, { x:0, y:0, w:13.3, h:7.5, fill:{ color: C.offWhite }, line:{ color: C.offWhite } });
accentBar(slide, C.teal);
}
function slideTitle(slide, title, x=0.4, y=0.22, w=12.5, h=0.7) {
slide.addShape(pres.shapes.RECTANGLE, { x:0, y:0, w:13.3, h:1.0, fill:{ color: C.navy }, line:{ color: C.navy } });
slide.addText(title, { x, y, w, h, fontSize:26, bold:true, color:C.white, fontFace:"Calibri Light", valign:"middle", margin:0 });
}
function pillBadge(slide, text, x, y, w, bgColor=C.teal) {
slide.addShape(pres.shapes.ROUNDED_RECTANGLE, { x, y, w, h:0.38, fill:{ color: bgColor }, line:{ color: bgColor }, rectRadius:0.15 });
slide.addText(text, { x, y, w, h:0.38, fontSize:12, bold:true, color:C.white, align:"center", valign:"middle", margin:0, fontFace:"Calibri" });
}
function card(slide, x, y, w, h, fill=C.white) {
slide.addShape(pres.shapes.RECTANGLE, { x, y, w, h, fill:{ color: fill }, line:{ color: C.lightGray }, shadow:{ type:"outer", color:"000000", blur:5, offset:2, angle:135, opacity:0.10 } });
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 1 — TITLE
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
darkSlide(s);
// gradient-like overlay strip
s.addShape(pres.shapes.RECTANGLE, { x:0, y:0, w:5.5, h:7.5, fill:{ color: C.teal }, line:{ color: C.teal }, transparency:75 });
s.addText("CLINICAL DIAGNOSIS &\nMANAGEMENT OF", {
x:0.7, y:1.2, w:11.5, h:1.6, fontSize:34, bold:true, color:C.sky,
fontFace:"Calibri Light", charSpacing:2
});
s.addText("THYROID DISORDERS", {
x:0.7, y:2.65, w:11.5, h:1.6, fontSize:52, bold:true, color:C.white,
fontFace:"Calibri Light"
});
s.addText("A Step-by-Step Clinical Guide", {
x:0.7, y:4.35, w:8, h:0.55, fontSize:20, color:C.mint, fontFace:"Calibri", italic:true
});
s.addShape(pres.shapes.RECTANGLE, { x:0.7, y:5.1, w:2.5, h:0.06, fill:{ color: C.amber }, line:{ color: C.amber } });
s.addText("Topics: Hypothyroidism • Hyperthyroidism • Goiter • Thyroid Nodules • Thyroid Cancer", {
x:0.7, y:5.3, w:11.5, h:0.5, fontSize:14, color:C.mint, fontFace:"Calibri"
});
accentBar(s, C.amber);
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 2 — OVERVIEW / TABLE OF CONTENTS
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "What We Will Cover");
const topics = [
["01", "HPT Axis & Thyroid Physiology Review", C.teal],
["02", "Step-by-Step Diagnostic Approach", C.navy],
["03", "Hypothyroidism – Diagnosis & Management", C.teal],
["04", "Hyperthyroidism – Diagnosis & Management", C.navy],
["05", "Goiter & Thyroid Nodules", C.teal],
["06", "Thyroid Cancer – Diagnosis & Management", C.navy],
["07", "Special Situations (Pregnancy, Subclinical)", C.teal],
["08", "Key Laboratory Reference Values", C.navy],
];
const col1 = topics.slice(0,4);
const col2 = topics.slice(4);
col1.forEach(([num,title,col],i)=>{
const y = 1.3 + i*1.35;
card(s, 0.35, y, 5.9, 1.15, C.white);
s.addShape(pres.shapes.RECTANGLE, { x:0.35, y, w:0.7, h:1.15, fill:{ color:col }, line:{ color:col } });
s.addText(num, { x:0.35, y, w:0.7, h:1.15, fontSize:22, bold:true, color:C.white, align:"center", valign:"middle", margin:0, fontFace:"Calibri Light" });
s.addText(title, { x:1.15, y:y+0.28, w:5.0, h:0.6, fontSize:14, bold:true, color:C.text, fontFace:"Calibri", valign:"middle" });
});
col2.forEach(([num,title,col],i)=>{
const y = 1.3 + i*1.35;
card(s, 6.85, y, 6.0, 1.15, C.white);
s.addShape(pres.shapes.RECTANGLE, { x:6.85, y, w:0.7, h:1.15, fill:{ color:col }, line:{ color:col } });
s.addText(num, { x:6.85, y, w:0.7, h:1.15, fontSize:22, bold:true, color:C.white, align:"center", valign:"middle", margin:0, fontFace:"Calibri Light" });
s.addText(title, { x:7.65, y:y+0.28, w:5.0, h:0.6, fontSize:14, bold:true, color:C.text, fontFace:"Calibri", valign:"middle" });
});
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 3 — SECTION: PHYSIOLOGY
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
sectionHeader(s, "PART 1: PHYSIOLOGY", "HPT Axis – The Foundation of Thyroid Diagnostics");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 4 — HPT AXIS
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "The HPT Axis – How the Thyroid is Controlled");
// Flow boxes
const boxes = [
{ label:"Hypothalamus", sub:"Releases TRH\n(Thyrotropin-releasing\nhormone – tripeptide)", x:0.4, col:C.navy },
{ label:"Anterior Pituitary", sub:"Releases TSH\n(Thyroid-stimulating\nhormone – glycoprotein)", x:3.9, col:C.teal },
{ label:"Thyroid Gland", sub:"Produces T4 (80%)\nand T3 (20%)\nvia NIS + TPO", x:7.4, col:C.sky },
{ label:"Target Tissues", sub:"T4 → T3 conversion\n(liver, kidney, muscle)\nActive T3 acts on nucleus", x:10.1, col:C.amber },
];
boxes.forEach(b=>{
card(s, b.x, 1.3, 2.9, 3.6, C.white);
s.addShape(pres.shapes.RECTANGLE, { x:b.x, y:1.3, w:2.9, h:0.55, fill:{ color:b.col }, line:{ color:b.col } });
s.addText(b.label, { x:b.x, y:1.3, w:2.9, h:0.55, fontSize:14, bold:true, color:C.white, align:"center", valign:"middle", margin:0, fontFace:"Calibri" });
s.addText(b.sub, { x:b.x+0.1, y:2.0, w:2.7, h:2.8, fontSize:13, color:C.text, fontFace:"Calibri", valign:"top", lineSpacingMultiple:1.3 });
});
// arrows
["3.35","6.85","10.38"].forEach((ax,i)=>{
s.addShape(pres.shapes.RIGHT_ARROW, { x:parseFloat(ax), y:2.8, w:0.5, h:0.4, fill:{ color:C.teal }, line:{ color:C.teal } });
});
// Negative feedback label
s.addShape(pres.shapes.RECTANGLE, { x:0.4, y:5.2, w:12.5, h:0.65, fill:{ color:C.mint }, line:{ color:C.sky } });
s.addText("NEGATIVE FEEDBACK: Free T3/T4 suppress both TRH (hypothalamus) and TSH (pituitary) — this forms the basis of ALL thyroid function tests", {
x:0.55, y:5.22, w:12.2, h:0.6, fontSize:12.5, color:C.teal, bold:true, fontFace:"Calibri", valign:"middle"
});
s.addText("Key Principle: TSH has a LOGARITHMIC inverse relationship with free T4 — a tiny drop in FT4 causes a LARGE surge in TSH, making TSH the most sensitive test.", {
x:0.4, y:6.05, w:12.5, h:0.55, fontSize:12, color:C.sub, fontFace:"Calibri", italic:true
});
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 5 — SECTION: DIAGNOSTIC APPROACH
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
sectionHeader(s, "PART 2: DIAGNOSTIC APPROACH", "Step-by-step framework for any thyroid presentation");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 6 — STEP-BY-STEP DIAGNOSTIC ALGORITHM
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "Step-by-Step Diagnostic Algorithm");
const steps = [
{ n:"1", title:"History & Physical Exam", body:"Symptoms: weight change, palpitations, fatigue, heat/cold intolerance\nNeck: goiter, nodule, tenderness | Family history | Drug history (amiodarone, lithium, immunotherapy)", col:C.navy },
{ n:"2", title:"Screen with TSH (3rd-gen assay)", body:"TSH normal → euthyroid (no further testing in stable outpatient)\nTSH low → suspect hyperthyroidism → add FT4 + FT3\nTSH high → suspect hypothyroidism → add FT4", col:C.teal },
{ n:"3", title:"Confirm with Free T4 (± Free T3)", body:"FT4 low + TSH high → Primary hypothyroidism\nFT4 high + TSH low → Primary hyperthyroidism\nFT4 low + TSH low → Central (pituitary) hypothyroidism", col:C.navy },
{ n:"4", title:"Identify Etiology (Cause)", body:"Anti-TPO antibodies → Hashimoto's or Graves'\nTSI (thyroid-stimulating immunoglobulin) → Graves' disease\nRAIU scan → Graves' vs. toxic nodule vs. thyroiditis\nUltrasound → structural: nodule, goiter, cancer risk", col:C.teal },
{ n:"5", title:"Classify & Manage", body:"Primary / Secondary / Subclinical? Overt vs. borderline?\nInitiate treatment based on type (see following slides)\nMonitor response: TSH every 6-8 weeks after any dose change", col:C.amber },
];
steps.forEach((st,i)=>{
const y = 1.15 + i*1.21;
card(s, 0.35, y, 12.6, 1.1, C.white);
s.addShape(pres.shapes.RECTANGLE, { x:0.35, y, w:0.65, h:1.1, fill:{ color:st.col }, line:{ color:st.col } });
s.addText(st.n, { x:0.35, y, w:0.65, h:1.1, fontSize:20, bold:true, color:C.white, align:"center", valign:"middle", margin:0, fontFace:"Calibri Light" });
s.addText("STEP "+st.n+": "+st.title, { x:1.1, y:y+0.05, w:4.2, h:0.45, fontSize:13, bold:true, color:st.col, fontFace:"Calibri", valign:"middle" });
s.addText(st.body, { x:1.1, y:y+0.5, w:11.7, h:0.55, fontSize:11.5, color:C.text, fontFace:"Calibri", valign:"top" });
});
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 7 — SECTION: HYPOTHYROIDISM
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
sectionHeader(s, "PART 3: HYPOTHYROIDISM", "Deficiency of thyroid hormones — the most common thyroid disorder");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 8 — HYPOTHYROIDISM CAUSES & CLINICAL FEATURES
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "Hypothyroidism — Causes & Clinical Features");
// LEFT PANEL: Causes
card(s, 0.35, 1.15, 4.2, 5.8, C.white);
s.addShape(pres.shapes.RECTANGLE, { x:0.35, y:1.15, w:4.2, h:0.55, fill:{ color:C.navy }, line:{ color:C.navy } });
s.addText("CAUSES", { x:0.35, y:1.15, w:4.2, h:0.55, fontSize:15, bold:true, color:C.white, align:"center", valign:"middle", margin:0, fontFace:"Calibri" });
const causes = [
["Primary (most common)",""],
["Hashimoto's thyroiditis","Autoimmune (anti-TPO +)"],
["Post-radioiodine / surgery","Iatrogenic"],
["Iodine deficiency","Worldwide #1 cause"],
["Drugs","Amiodarone, lithium, PTU excess, immune checkpoint inhibitors"],
["Congenital hypothyroidism","Absent gland / TPO defect"],
["",""],
["Secondary (central)",""],
["Pituitary adenoma","Low TSH + Low FT4"],
["Sheehan's syndrome","Post-partum pituitary necrosis"],
];
causes.forEach((c,i)=>{
if(c[0]==="Primary (most common)" || c[0]==="Secondary (central)") {
s.addText(c[0], { x:0.5, y:1.82+i*0.48, w:3.9, h:0.38, fontSize:11.5, bold:true, color:C.teal, fontFace:"Calibri" });
} else if(c[0]==="") {
// spacer
} else {
s.addText("• "+c[0], { x:0.55, y:1.82+i*0.48, w:2.4, h:0.38, fontSize:11, color:C.text, fontFace:"Calibri", valign:"middle" });
if(c[1]) s.addText(c[1], { x:2.95, y:1.82+i*0.48, w:1.5, h:0.38, fontSize:9.5, color:C.sub, fontFace:"Calibri", italic:true, valign:"middle" });
}
});
// RIGHT PANEL: Symptoms
card(s, 4.85, 1.15, 8.1, 5.8, C.white);
s.addShape(pres.shapes.RECTANGLE, { x:4.85, y:1.15, w:8.1, h:0.55, fill:{ color:C.teal }, line:{ color:C.teal } });
s.addText("CLINICAL FEATURES (Myxedema Symptoms)", { x:4.85, y:1.15, w:8.1, h:0.55, fontSize:15, bold:true, color:C.white, align:"center", valign:"middle", margin:0, fontFace:"Calibri" });
const systems = [
{ sys:"General", sx:"Weight gain, cold intolerance, fatigue, lethargy", x:5.05, y:1.85 },
{ sys:"Skin", sx:"Dry, coarse skin; puffy face (periorbital edema); non-pitting edema; alopecia; brittle nails", x:5.05, y:2.45 },
{ sys:"CVS", sx:"Bradycardia, reduced cardiac output, pericardial effusion, hypertension", x:5.05, y:3.1 },
{ sys:"Neuro", sx:"Slowed reflexes (delayed relaxation), cognitive slowing, depression, carpal tunnel syndrome", x:5.05, y:3.75 },
{ sys:"GI", sx:"Constipation, macroglossia, abdominal distension", x:5.05, y:4.38 },
{ sys:"Repro", sx:"Menorrhagia, anovulation, infertility; galactorrhea (↑TRH → ↑prolactin)", x:5.05, y:4.95 },
{ sys:"Labs", sx:"↑TSH, ↓FT4, ↑cholesterol, ↑CK, hyponatremia, normocytic or macrocytic anemia", x:5.05, y:5.55 },
];
systems.forEach(({sys,sx,x,y})=>{
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x, y, w:1.3, h:0.42, fill:{ color:C.navy }, line:{ color:C.navy }, rectRadius:0.08 });
s.addText(sys, { x, y, w:1.3, h:0.42, fontSize:11, bold:true, color:C.white, align:"center", valign:"middle", margin:0, fontFace:"Calibri" });
s.addText(sx, { x:x+1.4, y:y+0.02, w:6.4, h:0.4, fontSize:11, color:C.text, fontFace:"Calibri", valign:"middle" });
});
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 9 — HYPOTHYROIDISM DIAGNOSIS & MANAGEMENT
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "Hypothyroidism — Diagnosis & Management");
// DIAGNOSIS
card(s, 0.35, 1.15, 5.9, 2.9, C.white);
s.addShape(pres.shapes.RECTANGLE, { x:0.35, y:1.15, w:5.9, h:0.5, fill:{ color:C.navy }, line:{ color:C.navy } });
s.addText("DIAGNOSIS", { x:0.35, y:1.15, w:5.9, h:0.5, fontSize:16, bold:true, color:C.white, align:"center", valign:"middle", margin:0 });
const diag = [
"TSH > 5.0 mIU/L = hypothyroid; confirm with FT4",
"Overt hypothyroidism: TSH ↑ + FT4 ↓",
"Subclinical hypothyroidism: TSH ↑ (5–10) + FT4 normal",
"Central hypothyroid: TSH low/normal + FT4 ↓ (pituitary disease)",
"Anti-TPO antibodies positive → Hashimoto's",
];
diag.forEach((d,i)=>{
s.addText("• "+d, { x:0.55, y:1.78+i*0.44, w:5.6, h:0.4, fontSize:11.5, color:C.text, fontFace:"Calibri", valign:"middle" });
});
// LABS
card(s, 0.35, 4.2, 5.9, 2.65, C.white);
s.addShape(pres.shapes.RECTANGLE, { x:0.35, y:4.2, w:5.9, h:0.5, fill:{ color:C.teal }, line:{ color:C.teal } });
s.addText("SUPPORTING LABS", { x:0.35, y:4.2, w:5.9, h:0.5, fontSize:16, bold:true, color:C.white, align:"center", valign:"middle", margin:0 });
const labs = [
"Lipid panel (hypercholesterolemia common)",
"CBC (normocytic / macrocytic anemia)",
"Serum CK (elevated in myxedema)",
"Thyroid ultrasound if nodule/goiter palpated",
"Anti-TPO, anti-Tg antibodies",
];
labs.forEach((l,i)=>{
s.addText("• "+l, { x:0.55, y:4.82+i*0.44, w:5.6, h:0.4, fontSize:11.5, color:C.text, fontFace:"Calibri", valign:"middle" });
});
// MANAGEMENT
card(s, 6.55, 1.15, 6.4, 5.7, C.white);
s.addShape(pres.shapes.RECTANGLE, { x:6.55, y:1.15, w:6.4, h:0.5, fill:{ color:C.amber }, line:{ color:C.amber } });
s.addText("MANAGEMENT", { x:6.55, y:1.15, w:6.4, h:0.5, fontSize:16, bold:true, color:C.white, align:"center", valign:"middle", margin:0 });
const mgmt = [
["Drug of Choice:", "Levothyroxine (LT4) – synthetic T4"],
["Starting Dose:", "1.6 μg/kg/day (full replacement)\nElderly/cardiac: start 25-50 μg/day, titrate slowly"],
["Monitoring:", "Check TSH every 6-8 weeks after ANY dose change\nTarget TSH: 0.5–2.5 mIU/L (younger patients)\nTarget TSH: 1–4 mIU/L (elderly, pregnancy: 0.1–2.5)"],
["Administration:", "Take on empty stomach, 30–60 min before food\nAvoid: calcium, iron, PPIs within 4 hours"],
["Subclinical:", "Treat if TSH > 10 OR if TSH 5–10 with symptoms,\npregnancy, anti-TPO positive"],
["Emergency:", "Myxedema coma: IV T4 200–400 μg stat + IV T3\n+ hydrocortisone (rule out adrenal crisis)"],
];
mgmt.forEach(([lbl,txt],i)=>{
s.addText(lbl, { x:6.75, y:1.78+i*0.9, w:1.9, h:0.35, fontSize:11.5, bold:true, color:C.amber, fontFace:"Calibri", valign:"middle" });
s.addText(txt, { x:8.7, y:1.78+i*0.9, w:4.1, h:0.75, fontSize:11, color:C.text, fontFace:"Calibri", valign:"top", lineSpacingMultiple:1.2 });
});
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 10 — SECTION: HYPERTHYROIDISM
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
sectionHeader(s, "PART 4: HYPERTHYROIDISM", "Excess thyroid hormone — a hypermetabolic state");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 11 — HYPERTHYROIDISM CAUSES & CLINICAL FEATURES
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "Hyperthyroidism — Causes & Clinical Features");
card(s, 0.35, 1.15, 4.2, 5.8, C.white);
s.addShape(pres.shapes.RECTANGLE, { x:0.35, y:1.15, w:4.2, h:0.55, fill:{ color:C.red }, line:{ color:C.red } });
s.addText("CAUSES", { x:0.35, y:1.15, w:4.2, h:0.55, fontSize:15, bold:true, color:C.white, align:"center", valign:"middle", margin:0 });
const hCauses = [
["Graves' Disease","Most common (70–80%)"],
["Toxic Multinodular Goiter","Middle-aged/elderly"],
["Toxic Adenoma","Single autonomous nodule"],
["Subacute thyroiditis","Painful, post-viral (de Quervain)"],
["Hashitoxicosis","Early Hashimoto's"],
["Exogenous T4/T3","Factitious hyperthyroidism"],
["TSH-secreting pituitary tumor","TSH ↑ + FT4 ↑ (rare)"],
["Struma ovarii","Ectopic thyroid in ovarian teratoma"],
];
hCauses.forEach(([cause,note],i)=>{
s.addText("• "+cause, { x:0.5, y:1.85+i*0.58, w:2.2, h:0.48, fontSize:11, color:C.text, bold:true, fontFace:"Calibri", valign:"middle" });
s.addText(note, { x:2.75, y:1.85+i*0.58, w:1.7, h:0.48, fontSize:10, color:C.sub, fontFace:"Calibri", italic:true, valign:"middle" });
});
card(s, 4.85, 1.15, 8.1, 5.8, C.white);
s.addShape(pres.shapes.RECTANGLE, { x:4.85, y:1.15, w:8.1, h:0.55, fill:{ color:C.red }, line:{ color:C.red } });
s.addText("CLINICAL FEATURES — Thyrotoxicosis", { x:4.85, y:1.15, w:8.1, h:0.55, fontSize:15, bold:true, color:C.white, align:"center", valign:"middle", margin:0 });
const hSx = [
{ sys:"General", sx:"Weight loss despite increased appetite, heat intolerance, sweating, fatigue" },
{ sys:"CVS", sx:"Palpitations, tachycardia (AF common), wide pulse pressure, cardiac failure" },
{ sys:"Neuro", sx:"Anxiety, irritability, tremor (fine), insomnia, hyperreflexia" },
{ sys:"GI", sx:"Diarrhea, hyperdefecation, nausea" },
{ sys:"Musculo", sx:"Proximal myopathy, thyrotoxic periodic paralysis (esp. Asian males)" },
{ sys:"Repro", sx:"Oligomenorrhea, reduced libido, gynaecomastia (males)" },
{ sys:"Eyes", sx:"Graves' ophthalmopathy: proptosis, lid lag, chemosis (TSI-mediated)" },
{ sys:"Neck", sx:"Diffuse goiter (Graves), nodular goiter (TMNG), bruit (Graves)" },
];
hSx.forEach(({sys,sx},i)=>{
s.addShape(pres.shapes.ROUNDED_RECTANGLE, { x:5.05, y:1.85+i*0.58, w:1.3, h:0.42, fill:{ color:C.red }, line:{ color:C.red }, rectRadius:0.08 });
s.addText(sys, { x:5.05, y:1.85+i*0.58, w:1.3, h:0.42, fontSize:11, bold:true, color:C.white, align:"center", valign:"middle", margin:0 });
s.addText(sx, { x:6.45, y:1.87+i*0.58, w:6.4, h:0.4, fontSize:11, color:C.text, fontFace:"Calibri", valign:"middle" });
});
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 12 — HYPERTHYROIDISM DIAGNOSIS & MANAGEMENT
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "Hyperthyroidism — Diagnosis & Management");
card(s, 0.35, 1.15, 5.9, 3.2, C.white);
s.addShape(pres.shapes.RECTANGLE, { x:0.35, y:1.15, w:5.9, h:0.5, fill:{ color:C.navy }, line:{ color:C.navy } });
s.addText("DIAGNOSIS", { x:0.35, y:1.15, w:5.9, h:0.5, fontSize:16, bold:true, color:C.white, align:"center", valign:"middle", margin:0 });
const hDiag = [
"TSH < 0.1 mIU/L (suppressed) + FT4 ↑ = overt hyperthyroidism",
"TSH low + FT4 normal → check FT3 (T3 toxicosis)",
"TSI positive → Graves' disease (90% sensitivity)",
"RAIU ↑ diffuse → Graves' | focal hotspot → Toxic adenoma",
"RAIU ↓ → Thyroiditis | Exogenous T4 | Struma ovarii",
"Thyroid ultrasound with Doppler (Graves' → hypervascular)",
];
hDiag.forEach((d,i)=>{
s.addText("• "+d, { x:0.55, y:1.78+i*0.42, w:5.6, h:0.38, fontSize:11.5, color:C.text, fontFace:"Calibri", valign:"middle" });
});
card(s, 0.35, 4.5, 5.9, 2.35, C.white);
s.addShape(pres.shapes.RECTANGLE, { x:0.35, y:4.5, w:5.9, h:0.5, fill:{ color:C.teal }, line:{ color:C.teal } });
s.addText("GRAVES' DISEASE SPECIFIC", { x:0.35, y:4.5, w:5.9, h:0.5, fontSize:16, bold:true, color:C.white, align:"center", valign:"middle", margin:0 });
const gd = [
"Diffuse goiter + eye signs + pretibial myxedema = classic triad",
"TSI/TRAb: diagnostic (differentiates from other causes)",
"First-line: Antithyroid drugs (ATDs) for 12–18 months",
"Monitor: TRAb levels to predict remission/relapse",
];
gd.forEach((d,i)=>{
s.addText("• "+d, { x:0.55, y:5.1+i*0.42, w:5.6, h:0.38, fontSize:11.5, color:C.text, fontFace:"Calibri", valign:"middle" });
});
card(s, 6.55, 1.15, 6.4, 5.7, C.white);
s.addShape(pres.shapes.RECTANGLE, { x:6.55, y:1.15, w:6.4, h:0.5, fill:{ color:C.red }, line:{ color:C.red } });
s.addText("MANAGEMENT — 3 Treatment Options", { x:6.55, y:1.15, w:6.4, h:0.5, fontSize:15, bold:true, color:C.white, align:"center", valign:"middle", margin:0 });
const opts = [
{ num:"1", title:"Antithyroid Drugs (ATDs)", body:"Methimazole (preferred) or PTU (pregnancy 1st trim)\nBlocks TPO → stops organification\nDose: Methimazole 10–30 mg/day; PTU 100–300 mg TDS\nSE: agranulocytosis (0.5%), hepatotoxicity (PTU)\nMonitor: TFTs every 4–6 weeks; CBC if fever/sore throat", col:C.navy },
{ num:"2", title:"Radioactive Iodine (¹³¹I)", body:"Ablates thyroid tissue → hypothyroidism in 6–12 months\nPreferred in Graves'/TMNG (not pregnancy, severe ophthalmopathy)\nPre-treat with ATDs in severe disease\nPost-treatment: lifelong levothyroxine replacement", col:C.teal },
{ num:"3", title:"Surgery (Thyroidectomy)", body:"Total thyroidectomy for large goiter, cancer risk,\nfailed ATDs, patient preference\nPre-op: render euthyroid with ATDs + iodine (Lugol's)\nComplications: hypoparathyroidism, RLN palsy", col:C.amber },
];
opts.forEach(({num,title,body,col},i)=>{
const y = 1.8 + i*1.85;
s.addShape(pres.shapes.RECTANGLE, { x:6.7, y, w:0.6, h:1.6, fill:{ color:col }, line:{ color:col } });
s.addText(num, { x:6.7, y, w:0.6, h:1.6, fontSize:22, bold:true, color:C.white, align:"center", valign:"middle", margin:0 });
s.addText(title, { x:7.4, y:y+0.05, w:5.4, h:0.4, fontSize:13, bold:true, color:col, fontFace:"Calibri" });
s.addText(body, { x:7.4, y:y+0.45, w:5.4, h:1.1, fontSize:11, color:C.text, fontFace:"Calibri", valign:"top", lineSpacingMultiple:1.2 });
});
// Thyroid storm box
s.addShape(pres.shapes.RECTANGLE, { x:0.35, y:6.85, w:12.6, h:0.55, fill:{ color:C.red }, line:{ color:C.red } });
s.addText("⚠ THYROID STORM: PTU + Propranolol + Lugol's iodine + Dexamethasone + Cooling — ICU admission", { x:0.45, y:6.87, w:12.4, h:0.48, fontSize:12.5, bold:true, color:C.white, fontFace:"Calibri", valign:"middle" });
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 13 — SECTION: GOITER & NODULES
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
sectionHeader(s, "PART 5: GOITER & NODULES", "Structural thyroid abnormalities — when to investigate");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 14 — GOITER & THYROID NODULE EVALUATION
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "Thyroid Nodule — Step-by-Step Evaluation");
// Flowchart-style algorithm
const nodes = [
{ label:"Thyroid Nodule Detected\n(clinical / incidental / US)", x:4.5, y:1.25, w:4.3, h:0.7, fill:C.navy, textColor:C.white, fontSize:13 },
{ label:"Step 1: Check TSH", x:5.0, y:2.2, w:3.3, h:0.55, fill:C.teal, textColor:C.white, fontSize:12 },
{ label:"TSH Low\n(Autonomous nodule?)", x:0.7, y:3.1, w:3.0, h:0.65, fill:C.orange, textColor:C.white, fontSize:11 },
{ label:"TSH Normal/High\n(Most common)", x:9.1, y:3.1, w:3.5, h:0.65, fill:C.teal, textColor:C.white, fontSize:11 },
{ label:"RAIU Scan:\nHot nodule → treat hyper-\nthyroidism (RAI or surgery)", x:0.4, y:4.05, w:3.5, h:0.85, fill:C.white, textColor:C.text, fontSize:10.5 },
{ label:"Step 2: Thyroid Ultrasound\nTIRADS scoring (size, echogenicity,\nmargins, calcification, shape)", x:8.0, y:4.05, w:4.95, h:0.85, fill:C.white, textColor:C.text, fontSize:10.5 },
{ label:"TIRADS 1-2: Benign\nNo biopsy needed\nRoutine follow-up", x:0.4, y:5.15, w:3.5, h:0.85, fill:C.green, textColor:C.white, fontSize:10.5 },
{ label:"TIRADS 3: Low suspicion\nBiopsy if ≥2.5 cm\nor growing", x:4.2, y:5.15, w:3.2, h:0.85, fill:C.teal, textColor:C.white, fontSize:10.5 },
{ label:"TIRADS 4-5: High suspicion\nFNA Biopsy regardless\nof size (>1 cm)", x:7.65, y:5.15, w:3.5, h:0.85, fill:C.red, textColor:C.white, fontSize:10.5 },
{ label:"Bethesda Classification (Cytology): I=Non-diagnostic | II=Benign | III/IV=Indeterminate | V=Suspicious | VI=Malignant", x:0.4, y:6.22, w:12.5, h:0.6, fill:C.navy, textColor:C.white, fontSize:11 },
];
nodes.forEach(({label,x,y,w,h,fill,textColor,fontSize})=>{
card(s, x, y, w, h, fill);
s.addShape(pres.shapes.RECTANGLE, { x, y, w, h, fill:{ color:fill }, line:{ color:fill } });
s.addText(label, { x:x+0.06, y, w:w-0.12, h, fontSize, color:textColor, fontFace:"Calibri", align:"center", valign:"middle", lineSpacingMultiple:1.2 });
});
// Arrows
s.addShape(pres.shapes.DOWN_ARROW, { x:6.4, y:1.97, w:0.5, h:0.28, fill:{ color:C.teal }, line:{ color:C.teal } });
s.addShape(pres.shapes.DOWN_ARROW, { x:2.05, y:3.78, w:0.45, h:0.3, fill:{ color:C.orange }, line:{ color:C.orange } });
s.addShape(pres.shapes.DOWN_ARROW, { x:10.45, y:3.78, w:0.45, h:0.3, fill:{ color:C.teal }, line:{ color:C.teal } });
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 15 — SECTION: THYROID CANCER
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
sectionHeader(s, "PART 6: THYROID CANCER", "Diagnosis, staging and management of malignant thyroid disease");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 16 — THYROID CANCER TYPES & MANAGEMENT
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "Thyroid Cancer — Types, Diagnosis & Management");
const types = [
{ name:"Papillary\nThyroid Ca", pct:"85%", origin:"Follicular cells", markers:"Thyroglobulin, BRAF V600E", spread:"Lymph nodes (cervical)", prog:"Excellent (>95% 10-yr survival)", mgmt:"Total thyroidectomy + RAI ablation + TSH suppression with LT4", col:C.teal },
{ name:"Follicular\nThyroid Ca", pct:"10%", origin:"Follicular cells", markers:"Thyroglobulin, RAS mutations", spread:"Hematogenous (lung, bone)", prog:"Good (80% 10-yr survival)", mgmt:"Total thyroidectomy + RAI + TSH suppression", col:C.navy },
{ name:"Medullary\nThyroid Ca", pct:"3-4%", origin:"C-cells (parafollicular)", markers:"Calcitonin, CEA, RET mutation", spread:"Lymph nodes + systemic", prog:"Moderate (75% 10-yr)", mgmt:"Total thyroidectomy (NO RAI — calcitonin not iodine-avid)\nVandetanib/Cabozantinib for metastatic", col:C.orange },
{ name:"Anaplastic\nThyroid Ca", pct:"1-2%", origin:"Follicular cells (undifferentiated)", markers:"None specific", spread:"Rapid local + distant", prog:"Very poor (median survival 5 months)", mgmt:"Multimodal: surgery + XRT + Dabrafenib/Trametinib (BRAF+)\nPalliative airway management", col:C.red },
];
types.forEach(({name,pct,origin,markers,spread,prog,mgmt,col},i)=>{
const x = 0.35 + i*3.24;
card(s, x, 1.15, 3.1, 5.7, C.white);
s.addShape(pres.shapes.RECTANGLE, { x, y:1.15, w:3.1, h:0.6, fill:{ color:col }, line:{ color:col } });
s.addText(name, { x, y:1.15, w:3.1, h:0.6, fontSize:13, bold:true, color:C.white, align:"center", valign:"middle", margin:0, fontFace:"Calibri" });
pillBadge(s, pct+" of cases", x+0.7, 1.87, 1.7, col);
const rows = [["Origin",origin],["Marker",markers],["Spread",spread],["Prognosis",prog],["Management",mgmt]];
rows.forEach(([lbl,val],j)=>{
s.addText(lbl+":", { x:x+0.1, y:2.42+j*0.9, w:1.0, h:0.3, fontSize:10.5, bold:true, color:col, fontFace:"Calibri" });
s.addText(val, { x:x+0.1, y:2.73+j*0.9, w:2.9, h:0.5, fontSize:10.5, color:C.text, fontFace:"Calibri", lineSpacingMultiple:1.1 });
});
});
s.addText("Post-operative monitoring: Thyroglobulin (PTC/FTC) | Calcitonin (MTC) | Whole-body ¹³¹I scan | Neck ultrasound every 6–12 months", {
x:0.35, y:7.05, w:12.6, h:0.38, fontSize:11.5, color:C.sub, fontFace:"Calibri", italic:true
});
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 17 — SECTION: SPECIAL SITUATIONS
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
sectionHeader(s, "PART 7: SPECIAL SITUATIONS", "Subclinical thyroid disease • Pregnancy • Euthyroid sick syndrome");
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 18 — SPECIAL CLINICAL SITUATIONS
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "Special Clinical Situations");
const panels = [
{ title:"Subclinical Hypothyroidism", col:C.navy, content:[
"TSH 5–10 mIU/L, FT4 NORMAL",
"Treat if: TSH >10, OR symptomatic,\nOR anti-TPO positive, OR pregnant",
"Start low-dose LT4 (25–50 μg/day)",
"Risk if untreated: cardiovascular disease, progression to overt hypothyroidism (4–8%/yr)",
]},
{ title:"Subclinical Hyperthyroidism", col:C.red, content:[
"TSH <0.1 mIU/L, FT4 NORMAL",
"Treat if: TSH <0.1 + age >65 + cardiac arrhythmia/osteoporosis",
"TSH 0.1–0.5 (mild): usually monitor",
"Risk if untreated: AF (3× risk), bone loss",
]},
{ title:"Thyroid in Pregnancy", col:C.teal, content:[
"TSH targets (trimester-specific):\n1st: 0.1–2.5 | 2nd: 0.2–3.0 | 3rd: 0.3–3.0 mIU/L",
"↑ LT4 dose by 20–30% in pregnancy (↑TBG + fetal demand)",
"Hyperthyroidism: PTU in 1st trim; Methimazole from 2nd trim",
"Screen all pregnant women with TSH at booking",
"Post-partum thyroiditis: hyper phase → hypo phase → recovery",
]},
{ title:"Euthyroid Sick Syndrome (NTI)", col:C.orange, content:[
"Critical illness → ↓T3, ↑rT3, normal/low TSH, normal FT4",
"NOT true thyroid disease — adaptive response",
"Do NOT initiate thyroid treatment on TFTs alone",
"Treat underlying illness; TFTs normalize on recovery",
"If clinical hypothyroidism pre-existing → continue LT4 IV",
]},
];
panels.forEach(({title,col,content},i)=>{
const x = 0.35 + i * 3.24;
card(s, x, 1.15, 3.1, 5.75, C.white);
s.addShape(pres.shapes.RECTANGLE, { x, y:1.15, w:3.1, h:0.55, fill:{ color:col }, line:{ color:col } });
s.addText(title, { x:x+0.05, y:1.15, w:3.0, h:0.55, fontSize:12.5, bold:true, color:C.white, align:"center", valign:"middle", margin:0, fontFace:"Calibri" });
content.forEach((c,j)=>{
s.addText("• "+c, { x:x+0.1, y:1.84+j*1.0, w:2.9, h:0.9, fontSize:11, color:C.text, fontFace:"Calibri", valign:"top", lineSpacingMultiple:1.2 });
});
});
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 19 — LABORATORY REFERENCE VALUES
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
contentSlide(s);
slideTitle(s, "Key Laboratory Reference Values & Interpretation");
// Table header
const cols = ["Test","Reference Range","Hypothyroid","Hyperthyroid","Note"];
const colW = [2.1, 2.3, 1.95, 1.95, 4.6];
const startX = 0.35;
let cx = startX;
cols.forEach((c,i)=>{
s.addShape(pres.shapes.RECTANGLE, { x:cx, y:1.15, w:colW[i], h:0.5, fill:{ color:C.navy }, line:{ color:C.navy } });
s.addText(c, { x:cx, y:1.15, w:colW[i], h:0.5, fontSize:13, bold:true, color:C.white, align:"center", valign:"middle", margin:0 });
cx += colW[i];
});
const rows = [
["TSH","0.35–5.0 mIU/L","↑↑ (>10 = overt)","↓↓ (<0.1 = overt)","Most sensitive thyroid test"],
["Free T4","12–28 pmol/L","↓","↑","Not affected by TBG changes"],
["Free T3","3–9 pmol/L","↓","↑↑","Check if T3 toxicosis suspected"],
["Total T4","55–150 nmol/L","↓↓","↑","Affected by TBG (pregnancy ↑, steroids ↓)"],
["Total T3","1.5–3.5 nmol/L","↓","↑","T3 toxicosis: T3 ↑ with normal T4"],
["rT3",">0.32 nmol/L (if elevated)","↓","normal","↑ in euthyroid sick syndrome"],
["Anti-TPO","><35 IU/mL = positive","↑ (Hashimoto's)","↑ (Graves')","Marker of autoimmune thyroid disease"],
["TSI","<1.75 IU/L","Negative","↑↑ (Graves')","90% sensitivity for Graves' disease"],
["Thyroglobulin","1–25 ng/mL (post-thyroidectomy <1)","Varies","Varies","Post-cancer surveillance marker"],
["HbA1c (co-morbidity)","<5.7% normal","Screen for DM in hypothyroid","Screen for DM","Insulin resistance ↑ in both states"],
];
rows.forEach((row,i)=>{
const rowFill = i%2===0 ? C.white : C.offWhite;
cx = startX;
row.forEach((cell,j)=>{
s.addShape(pres.shapes.RECTANGLE, { x:cx, y:1.65+i*0.54, w:colW[j], h:0.54, fill:{ color:rowFill }, line:{ color:C.lightGray } });
const textColor = j===2 ? C.red : j===3 ? C.red : C.text;
s.addText(cell, { x:cx+0.05, y:1.65+i*0.54, w:colW[j]-0.1, h:0.54, fontSize:11, color:textColor, fontFace:"Calibri", valign:"middle", lineSpacingMultiple:1.1 });
cx += colW[j];
});
});
}
// ─────────────────────────────────────────────────────────────────────────────
// SLIDE 20 — SUMMARY / KEY TAKE-AWAYS
// ─────────────────────────────────────────────────────────────────────────────
{
const s = pres.addSlide();
darkSlide(s);
s.addShape(pres.shapes.RECTANGLE, { x:0, y:0, w:0.55, h:7.5, fill:{ color:C.amber }, line:{ color:C.amber } });
s.addText("KEY TAKE-AWAYS", { x:0.75, y:0.35, w:12.0, h:0.75, fontSize:36, bold:true, color:C.white, fontFace:"Calibri Light", charSpacing:3 });
s.addShape(pres.shapes.RECTANGLE, { x:0.75, y:1.18, w:3.5, h:0.06, fill:{ color:C.amber }, line:{ color:C.amber } });
const points = [
"TSH is the FIRST and MOST SENSITIVE test for thyroid function — always start here.",
"Low TSH = hyperthyroid; High TSH = hypothyroid. Central disease (pituitary) breaks this rule — check FT4 together.",
"Hashimoto's (Hypothyroid) = Anti-TPO positive; Graves' (Hyperthyroid) = TSI positive, diffuse goiter, eye signs.",
"Levothyroxine (LT4) is the drug of choice for hypothyroidism; check TSH every 6-8 weeks after any dose change.",
"Hyperthyroidism: 3 options — ATDs (methimazole), Radioiodine (¹³¹I), or Surgery. Choose based on cause.",
"All thyroid nodules need TSH + ultrasound (TIRADS) ± FNA based on size/features — Bethesda cytology guides surgery.",
"Papillary carcinoma (85%) = best prognosis; Anaplastic (1-2%) = worst prognosis. Medullary thyroid Ca monitors calcitonin.",
"In pregnancy: trim-specific TSH targets; PTU in 1st trimester, methimazole thereafter; increase LT4 dose by 20-30%.",
"Euthyroid sick syndrome (NTI): ↓T3, ↑rT3 — do NOT treat unless true thyroid disease confirmed.",
];
points.forEach((p,i)=>{
const y = 1.45 + i*0.66;
s.addShape(pres.shapes.RECTANGLE, { x:0.75, y:y+0.08, w:0.35, h:0.35, fill:{ color:C.amber }, line:{ color:C.amber } });
s.addText((i+1).toString(), { x:0.75, y:y+0.08, w:0.35, h:0.35, fontSize:12, bold:true, color:C.white, align:"center", valign:"middle", margin:0 });
s.addText(p, { x:1.25, y, w:11.7, h:0.58, fontSize:13, color:C.white, fontFace:"Calibri", valign:"middle", lineSpacingMultiple:1.15 });
});
accentBar(s, C.amber);
}
// ─────────────────────────────────────────────────────────────────────────────
// WRITE FILE
// ─────────────────────────────────────────────────────────────────────────────
pres.writeFile({ fileName: "/home/daytona/workspace/thyroid-pptx/Thyroid_Disorders_Clinical_Guide.pptx" })
.then(() => console.log("✅ Done: Thyroid_Disorders_Clinical_Guide.pptx"))
.catch(err => { console.error("❌ Error:", err); process.exit(1); });
cd /home/daytona/workspace/thyroid-pptx && node build.js 2>&1
ls -lh /home/daytona/workspace/thyroid-pptx/Thyroid_Disorders_Clinical_Guide.ppt…
Thyroid Disorders Clinical Guide
Presentation · PPTX
What's inside (20 slides, wide 16:9 format)
| Slide | Content |
|---|---|
| 1 | Title slide with topic overview |
| 2 | Table of Contents (8 parts, card layout) |
| 3 | Section header - Physiology |
| 4 | HPT Axis - flow diagram with 4 stations and negative feedback rule |
| 5 | Section header - Diagnostic Approach |
| 6 | 5-Step Diagnostic Algorithm (history → TSH → FT4 → etiology → management) |
| 7 | Section header - Hypothyroidism |
| 8 | Hypothyroidism - Causes (Hashimoto's, iatrogenic, drugs, central) + Clinical Features by system |
| 9 | Hypothyroidism Management - LT4 dosing, targets, monitoring, myxedema coma protocol |
| 10 | Section header - Hyperthyroidism |
| 11 | Hyperthyroidism - 8 causes + full system-wise symptoms (tachycardia, tremor, eye signs, etc.) |
| 12 | Hyperthyroidism Management - Diagnosis, 3 treatment options (ATDs/RAI/Surgery), Graves'-specific, Thyroid Storm box |
| 13 | Section header - Goiter & Nodules |
| 14 | Thyroid Nodule Algorithm - TSH → US (TIRADS) → FNA → Bethesda classification flowchart |
| 15 | Section header - Thyroid Cancer |
| 16 | Thyroid Cancer - 4 types side-by-side (Papillary/Follicular/Medullary/Anaplastic) with markers, spread, prognosis, management |
| 17 | Section header - Special Situations |
| 18 | Special Situations - Subclinical hypo/hyper, Pregnancy (trimester TSH targets), Euthyroid Sick Syndrome |
| 19 | Laboratory Reference Table - TSH, FT4, FT3, antibodies with normal ranges + hypo/hyper columns |
| 20 | Key Take-Aways (9 points, dark closing slide) |
Make a presentation on clinical diagnosis and management of thyroid disorders step-by-step
ls -lh /home/daytona/workspace/thyroid-pptx/Thyroid_Disorders_Clinical_Guide.ppt…
Thyroid Disorders Clinical Guide
Presentation · PPTX
Presentation Overview (20 slides, wide 16:9)
| # | Slide | Key Content |
|---|---|---|
| 1 | Title | Full topic title + subtopics listed |
| 2 | Table of Contents | 8 parts shown as numbered cards |
| 3 | Section break | Physiology |
| 4 | HPT Axis | 4-box flow: Hypothalamus → Pituitary → Thyroid → Tissues + negative feedback rule |
| 5 | Section break | Diagnostic Approach |
| 6 | 5-Step Diagnostic Algorithm | History → TSH screen → FT4 confirm → Etiology → Classify & Treat |
| 7 | Section break | Hypothyroidism |
| 8 | Hypothyroid: Causes & Features | Hashimoto's, iatrogenic, drugs, central; symptoms by system |
| 9 | Hypothyroid: Diagnosis & Mgmt | LT4 dosing, TSH targets, monitoring, myxedema coma |
| 10 | Section break | Hyperthyroidism |
| 11 | Hyperthyroid: Causes & Features | Graves', TMNG, toxic adenoma; symptoms by system incl. eye signs |
| 12 | Hyperthyroid: Diagnosis & Mgmt | ATDs / Radioiodine / Surgery; Graves'-specific; Thyroid Storm box |
| 13 | Section break | Goiter & Nodules |
| 14 | Thyroid Nodule Algorithm | TSH → US TIRADS → FNA → Bethesda cytology flowchart |
| 15 | Section break | Thyroid Cancer |
| 16 | Thyroid Cancer (4 types) | Papillary / Follicular / Medullary / Anaplastic - markers, spread, prognosis, treatment |
| 17 | Section break | Special Situations |
| 18 | Special Situations | Subclinical hypo/hyper, Pregnancy TSH targets, Euthyroid Sick Syndrome |
| 19 | Lab Reference Table | TSH, FT4, FT3, antibodies - normal ranges + hypo/hyper columns |
| 20 | Key Take-Aways | 9 clinical pearls on dark closing slide |
u given information first i want that information
🧬 COMPLETE BIOCHEMISTRY GUIDE: Hormones, Metabolism & Diabetes
PART 1: STEROID HORMONE SYNTHESIS
What is a steroid hormone?
Where are they made?
| Gland/Organ | Hormones Produced |
|---|---|
| Adrenal Cortex - Zona Fasciculata | Cortisol |
| Adrenal Cortex - Zona Glomerulosa | Aldosterone |
| Adrenal Cortex - Zona Reticularis | DHEA, Androgens |
| Testes (Leydig cells) | Testosterone |
| Ovaries (Granulosa cells) | Estrogen, Progesterone |
| Placenta | Progesterone, Estriol |
The Big Picture Pathway
CHOLESTEROL (C27)
↓ [RATE-LIMITING STEP: StAR protein moves cholesterol into mitochondria]
↓ [Enzyme: CYP11A1 = P450scc, inner mitochondrial membrane]
PREGNENOLONE ← "Mother of all steroids"
↓ [3β-HSD enzyme, smooth ER]
PROGESTERONE
↓ splits into 3 pathways based on adrenal zone
┌──────────────────┬────────────────────┬──────────────────────┐
↓ ↓ ↓
GLUCOCORTICOIDS MINERALOCORTICOIDS ANDROGENS → ESTROGENS
(Zona Fasciculata) (Zona Glomerulosa) (Zona Reticularis)
CORTISOL ALDOSTERONE DHEA → Testosterone → Estradiol
Step-by-Step Enzymatic Pathway
Step 1 - The Rate-Limiting Step
- StAR protein (Steroidogenic Acute Regulatory protein) shuttles cholesterol from the outer to the inner mitochondrial membrane
- ACTH triggers StAR immediately - no StAR = no steroid synthesis
- Think of StAR as the "gate opener"
Step 2 - Cholesterol → Pregnenolone
- Enzyme: P450scc (CYP11A1) - "scc" = side chain cleavage
- Snips off a 6-carbon piece from cholesterol (C27) → pregnenolone (C21)
- Needs NADPH + Oxygen
- Location: Inner mitochondrial membrane
Step 3 - Pregnenolone → Progesterone
- Enzyme: 3β-HSD + isomerase
- Converts Δ5 compound (pregnenolone) into Δ4 compound (progesterone)
- Location: Smooth ER
Pathway A - CORTISOL (Zona Fasciculata)
Progesterone
↓ CYP17A1 (17α-hydroxylase) → adds OH at C17
17α-Hydroxyprogesterone (17-OHP)
↓ CYP21A2 (21-hydroxylase) → adds OH at C21
11-Deoxycortisol
↓ CYP11B1 (11β-hydroxylase) → adds OH at C11, in mitochondria
CORTISOL ✓
Pathway B - ALDOSTERONE (Zona Glomerulosa)
Progesterone
↓ CYP21A2 (21-hydroxylase)
11-Deoxycorticosterone (DOC)
↓ CYP11B1 (11β-hydroxylase)
Corticosterone
↓ CYP11B2 (Aldosterone synthase) ← ONLY in zona glomerulosa!
ALDOSTERONE ✓
Pathway C - ANDROGENS & ESTROGENS
17-Hydroxypregnenolone
↓ CYP17A1 (17,20-lyase activity)
DHEA (C19 - weak androgen)
↓ 3β-HSD
Androstenedione
↓ 17β-HSD
TESTOSTERONE (C19)
↓ CYP19A1 (Aromatase) in ovarian granulosa cells
ESTRADIOL (C18 - most potent estrogen)
OR
↓ 5α-Reductase in prostate/skin
DHT (most potent androgen, 5× more potent than testosterone)
Carbon Number Rule
- C21 = Glucocorticoids (cortisol) + Mineralocorticoids (aldosterone) + Progestogens
- C19 = Androgens (testosterone, DHEA)
- C18 = Estrogens (estradiol) - have aromatic ring A
Key Enzyme Summary Table
| Enzyme | Gene | Location | Reaction |
|---|---|---|---|
| P450scc (side-chain cleavage) | CYP11A1 | Mitochondria | Cholesterol → Pregnenolone |
| 3β-HSD | HSD3B2 | Smooth ER | Pregnenolone → Progesterone |
| 17α-Hydroxylase / 17,20-lyase | CYP17A1 | Smooth ER | 17-OH + androgen pathway |
| 21-Hydroxylase | CYP21A2 | Smooth ER | → Cortisol & Aldosterone pathway |
| 11β-Hydroxylase | CYP11B1 | Mitochondria | → Cortisol |
| Aldosterone synthase | CYP11B2 | Mitochondria (ZG only) | → Aldosterone |
| Aromatase | CYP19A1 | Smooth ER (ovary, adipose) | Androgens → Estrogens |
| 5α-Reductase | SRD5A | Target tissues | Testosterone → DHT |
Regulation
CAH - Enzyme Deficiency Clinical Table
| Deficiency | Effect | Clinical |
|---|---|---|
| 21-Hydroxylase (90-95%) | ↓ Cortisol, ↓ Aldosterone, ↑ Androgens | Salt-wasting crisis + virilization |
| 11β-Hydroxylase | ↑ DOC, ↑ Androgens, ↓ Cortisol | Hypertension + virilization |
| 17α-Hydroxylase | ↑ Aldosterone, ↓ Cortisol, ↓ Androgens | Hypertension + no sexual maturation |
PART 2: THYROID HORMONE SYNTHESIS
What are thyroid hormones?
- T4 (Thyroxine) = 4 iodine atoms, made exclusively in thyroid, is a prohormone (not very active)
- T3 (Triiodothyronine) = 3 iodine atoms, the active hormone, 80% comes from peripheral conversion of T4
Where it happens
The 6 Steps of Thyroid Hormone Synthesis
Step 1 - Iodide Trapping (Active Transport)
- Transporter: NIS (Sodium-Iodide Symporter) on the basolateral membrane (blood side)
- Brings 2 Na⁺ + 1 I⁻ into the cell together (symport)
- Concentrates iodide 20-40 times higher inside the cell than in blood
- Driven by the Na⁺ gradient (created by Na/K-ATPase)
- Pendrin transports I⁻ from cell into the colloid (apical membrane)
- Regulated by TSH (increases NIS activity); excess iodine inhibits it (Wolff-Chaikoff effect)
Step 2 - Thyroglobulin Synthesis
- Thyroglobulin (660 kDa glycoprotein) made in rough ER of thyrocyte
- Processed in Golgi, secreted by exocytosis into the colloid
- Contains 123 tyrosine residues, but only 4-8 actually become thyroid hormones
- Think of Tg as a "tyrosine delivery board" waiting to be iodinated
Step 3 - Organification of Iodide
- Enzyme: TPO (Thyroid Peroxidase) at the apical membrane (colloid side)
- TPO uses H₂O₂ (made by DUOX2 enzyme) to oxidize I⁻ → reactive iodine (I⁰)
- Reactive iodine attaches to tyrosine residues on Tg:
- One iodine added → MIT (Monoiodotyrosine)
- Two iodines added → DIT (Diiodotyrosine)
- Blocked by: PTU, Methimazole (antithyroid drugs)
Step 4 - Coupling (Making T3 and T4)
- Same enzyme: TPO catalyzes coupling
- Two iodinated tyrosines join together on the Tg scaffold:
- DIT + DIT → T4 (thyroxine, 4 iodines) - most abundant
- MIT + DIT → T3 (3,5,3′-triiodothyronine, 3 iodines) - active form
- DIT + MIT → rT3 (reverse T3, biologically inactive)
Step 5 - Secretion
- TSH stimulates thyrocytes to endocytose (eat) the colloid
- Colloid vesicles fuse with lysosomes → proteases digest thyroglobulin
- Free T4 and T3 released and diffuse into the bloodstream
- MIT and DIT are NOT secreted - iodotyrosine deiodinase strips their iodine off and recycles it
Step 6 - Peripheral Conversion (T4 → T3)
- T4 is a prohormone; must be converted to T3 to be active
- 80% of circulating T3 comes from this conversion in liver, kidney, muscle
- Deiodinases contain selenocysteine (selenium):
| Enzyme | Location | Makes |
|---|---|---|
| D1 | Liver, kidney, thyroid | T3 (main circulating T3 source) |
| D2 | Brain, pituitary, brown fat | Local T3 (especially in brain/pituitary) |
| D3 | Brain, placenta | Inactive rT3 (inactivates T4) |
Transport in Blood
| Binding Protein | % T4 Bound | % T3 Bound |
|---|---|---|
| TBG (Thyroxine-binding globulin) | 67% | 46% |
| Transthyretin | 20% | 1% |
| Albumin | 13% | 53% |
Half-Lives
| Hormone | Half-Life |
|---|---|
| T4 | 6-7 days |
| T3 | 18 hours |
HPT Axis (Regulation)
Hypothalamus → TRH (tripeptide)
↓
Anterior Pituitary (thyrotrophs) → TSH (glycoprotein, α+β subunits)
↓
Thyroid Gland → T4 (mainly) + small T3
↑ Negative feedback (free T3/T4 suppress both TRH and TSH)
PART 3: THYROID FUNCTION TESTS
The Tests - One by One
1. TSH (Thyroid-Stimulating Hormone)
- Normal range: 0.35-5.0 mIU/L
- The most sensitive test for thyroid dysfunction
- HIGH TSH = thyroid is failing = Primary Hypothyroidism
- LOW TSH = thyroid is overactive = Primary Hyperthyroidism
- Exception: If pituitary is diseased (central hypothyroidism), TSH may be low despite low T4
2. Free T4 (FT4)
- Normal range: 12-28 pmol/L (0.8-2.4 ng/dL)
- Measures only the unbound, biologically active T4
- More reliable than Total T4 because not affected by binding protein changes
3. Free T3 (FT3)
- Normal range: 3-9 pmol/L
- Used when: T3 toxicosis suspected (hyperthyroid with normal FT4 but elevated FT3)
4. Total T4 and Total T3
- Measures bound + free hormone
- Less useful because binding protein changes confuse results
- Estrogen (pregnancy, OCP) → ↑TBG → ↑Total T4/T3 (but patient is euthyroid, FT4 normal!)
- Androgens, glucocorticoids → ↓TBG → ↓Total T4/T3 (still euthyroid)
5. Reverse T3 (rT3)
- Elevated rT3 + Low T3 + Normal T4 = Euthyroid Sick Syndrome (nonthyroidal illness)
- In critical illness, starvation, major surgery: body shunts T4 → rT3 (inactive) to conserve energy
6. TRH Stimulation Test
- Inject 500 μg TRH IV → measure TSH at 0, 30, 60 min
- Normal: TSH rises by ≥6 mIU/L at 30 min
- Blunted response: Primary hyperthyroidism OR pituitary disease
- Exaggerated response: Primary hypothyroidism
- Largely replaced by modern sensitive TSH assays
7. Thyroid Antibodies
- Anti-TPO (aTPO): Positive in Hashimoto's (>80%) and Graves'
- TSI (Thyroid-Stimulating Immunoglobulin): Diagnostic for Graves' disease (~90% sensitivity)
- Anti-thyroglobulin (ATG): Hashimoto's
Complete Interpretation Table
| Condition | TSH | FT4 | FT3 |
|---|---|---|---|
| Primary Hyperthyroidism | ↓↓ | ↑ | ↑ |
| T3 Toxicosis | ↓ | Normal | ↑↑ |
| Subclinical Hyperthyroidism | ↓ | Normal | Normal |
| Primary Hypothyroidism | ↑↑ | ↓ | ↓ |
| Subclinical Hypothyroidism | ↑ | Normal | Normal |
| Central (Pituitary) Hypothyroidism | ↓ or Normal | ↓ | ↓ |
| Graves' Disease | ↓ | ↑ | ↑ |
| Euthyroid Sick Syndrome | Variable ↓ | ↓ | ↓↓ |
| Pregnancy (↑TBG) | Normal | Normal FT4 | Total T4 ↑↑ |
| Hashimoto's Thyroiditis | ↑ | ↓ or Normal | ↓ or Normal |
PART 4: PTH AND CALCIUM METABOLISM
Why is calcium important?
- Muscle contraction (including heart muscle)
- Nerve impulse transmission
- Blood clotting (coagulation cascade)
- Cell signaling (second messenger)
- Enzyme activation
Three Hormones Control Calcium
- PTH (Parathyroid Hormone) - raises calcium
- Calcitriol (1,25-(OH)₂-Vitamin D) - raises calcium
- Calcitonin - lowers calcium (minor role in adults)
PTH Structure and Trigger
- 84 amino acid polypeptide made by chief cells of the 4 parathyroid glands
- Biologically active portion = first 34 amino acids (N-terminal)
- CaSR (Calcium-Sensing Receptor) on chief cells detects blood calcium:
- Low Ca²⁺ → CaSR inactive → PTH released
- High Ca²⁺ → CaSR activated → PTH suppressed
PTH's 3 Target Actions
| Target | Action | Effect |
|---|---|---|
| Bone | Activates osteoclasts (bone breakers) | Releases Ca²⁺ AND PO₄³⁻ from bone |
| Kidney (DCT) | ↑ Ca²⁺ reabsorption; ↓ PO₄³⁻ reabsorption (phosphaturic effect) | Saves Ca²⁺, loses PO₄³⁻ |
| Kidney (PCT) | Activates 1α-hydroxylase → converts 25-OH-Vit D to Calcitriol | Indirectly ↑ intestinal Ca²⁺ absorption |
PTH Mechanism of Action
- PTH receptor (PTH1R) is a GPCR
- PTH → Gαs → Adenylyl cyclase → cAMP ↑ → PKA activation
- Also activates Gq → PLC → IP₃ → Ca²⁺ release + PKC
Vitamin D Activation Pathway
Skin: UV light + 7-dehydrocholesterol → Cholecalciferol (Vitamin D3)
↓ Liver: 25-hydroxylase
25-hydroxyvitamin D (Calcidiol) ← what you measure in blood tests!
↓ Kidney: 1α-hydroxylase (activated by PTH, low PO₄, low Ca)
1,25-dihydroxyvitamin D (Calcitriol) ← the ACTIVE form
Actions of Calcitriol
- Intestine: Increases calbindin-D (calcium transport protein) + TRPV6 channels → ↑ Ca²⁺ absorption (up to 80% of dietary calcium)
- Bone: At normal levels, promotes mineralization; at high levels, releases Ca with PTH
- Kidney: Mild increase in Ca²⁺ reabsorption
- Parathyroid gland: Suppresses PTH synthesis (negative feedback)
Calcitonin
- Made by C-cells (parafollicular cells) of the thyroid
- Released when Ca²⁺ is HIGH
- Inhibits osteoclasts → reduces bone resorption; increases renal Ca excretion
Calcium and Phosphate Inverse Relationship
| Condition | Calcium | Phosphate |
|---|---|---|
| Hyperparathyroidism | ↑ | ↓ |
| Hypoparathyroidism | ↓ | ↑ |
| Vitamin D toxicity | ↑ | ↑ |
| CKD | ↓ | ↑↑ (Secondary hyperparathyroidism) |
Phosphate Regulation
| Hormone | Effect on Blood Phosphate | Mechanism |
|---|---|---|
| PTH | ↓ (phosphaturia) | Inhibits NaPi cotransporter in kidney PCT |
| Calcitriol | ↑ | Increases intestinal PO₄ absorption |
| FGF-23 (from bone) | ↓↓ | Major phosphaturic hormone; also inhibits 1α-hydroxylase |
PART 5: INSULIN - STRUCTURE AND RECEPTOR
What is insulin?
- α cells (25%) - Glucagon
- β cells (60%) - Insulin
- δ cells (10%) - Somatostatin
- PP cells (5%) - Pancreatic polypeptide
Insulin Structure
- Molecular weight: 5,808 Da
- Two chains: A chain (21 amino acids) + B chain (30 amino acids)
- Connected by: 2 disulfide bonds between chains + 1 within the A chain
- If you split the two chains apart, insulin completely loses its activity
Insulin Biosynthesis Pathway
Gene on chromosome 11
↓ Transcription + Translation on ribosomes (RER)
PREPROINSULIN (110 amino acids, MW ~11,500)
↓ Signal peptide cleaved in ER lumen
PROINSULIN (86 amino acids, MW ~9,000) = A chain + B chain + C peptide
↓ Packaged in Golgi vesicles
↓ Cleavage by prohormone convertases (PC1 and PC2) + CPE
INSULIN (A+B chains, MW 5,808) + C PEPTIDE (31 amino acids)
↓ Both secreted together in EQUIMOLAR amounts from secretory granules
How Glucose Triggers Insulin Secretion
Glucose enters β-cell via GLUT2 (passive)
↓
Glucokinase (Hexokinase IV) phosphorylates glucose → G-6-P
↓
Glycolysis + TCA cycle → ATP production
↓
↑ ATP/ADP ratio
↓
ATP-sensitive K⁺ channel (KATP channel) CLOSES
↓
β-cell membrane DEPOLARIZES
↓
Voltage-gated Ca²⁺ channels OPEN
↓
Ca²⁺ floods into β-cell
↓
Insulin granules FUSE with membrane → EXOCYTOSIS of insulin + C-peptide
- Phase 1 (3-5 min): Rapid dump of pre-stored insulin granules
- Phase 2 (15 min to 2 hrs): Slower, sustained secretion from newly synthesized insulin
Insulin Receptor Signal Transduction
Insulin binds α subunit
↓
β subunit AUTOPHOSPHORYLATES (on tyrosine residues)
↓
Phosphorylates IRS-1/IRS-2 (Insulin Receptor Substrate proteins)
↓
┌─────────────────────────────────┐
↓ ↓
PI3K → PIP3 → PDK1 → Akt Grb2/SOS → Ras → ERK
(Metabolic effects: (Mitogenic effects:
GLUT4 translocation, cell growth,
glycogen synthesis, gene expression,
lipogenesis, differentiation)
protein synthesis)
PART 6: ROLE OF C-PEPTIDE
Why Does C-Peptide Matter?
- Injected insulin has no C-peptide
- High insulin + Low C-peptide → patient is injecting insulin (factitious hypoglycemia / insulin misuse)
- High insulin + High C-peptide → body is making too much insulin (insulinoma)
- C-peptide measurement tells you how much insulin the pancreas is actually making
- C-peptide has longer half-life (~35 min) vs. insulin (~5 min) → easier to measure
- Used to distinguish Type 1 DM (C-peptide absent/very low) from Type 2 DM (C-peptide normal/high)
- Binds a G-protein-coupled receptor
- Activates Na/K-ATPase and eNOS (endothelial nitric oxide synthase)
- May protect against diabetic nephropathy and neuropathy (role still being studied)
PART 7: GLUCAGON
What is glucagon?
- Insulin = fed state hormone (glucose ↑ → insulin ↑ → store energy)
- Glucagon = fasting state hormone (glucose ↓ → glucagon ↑ → release energy)
Structure
- 29 amino acid polypeptide
- Made from proglucagon (158 amino acids)
- Same proglucagon gene, but processed differently in intestinal L-cells → makes GLP-1 instead
Stimulation and Inhibition
| Stimulates Glucagon | Inhibits Glucagon |
|---|---|
| Low blood glucose (hypoglycemia) | High blood glucose |
| Amino acids (alanine, arginine) | Insulin |
| Fasting, exercise, stress | Somatostatin |
| Epinephrine | Free fatty acids |
| Cortisol | GLP-1 |
Glucagon Receptor and Mechanism
Glucagon binds glucagon receptor on hepatocyte
↓
Gαs protein activates Adenylyl Cyclase
↓
ATP → cAMP ↑↑
↓
Protein Kinase A (PKA) activated
↓
┌──────────────────────────────────────────┐
↓ ↓
GLYCOGENOLYSIS GLUCONEOGENESIS
(glycogen phosphorylase activated; (PEPCK, fructose-1,6-
PFK-2 inhibited) bisphosphatase activated)
↓ ↓
Glucose released from glycogen New glucose from
into blood amino acids, lactate, glycerol
- Lipolysis: Activates hormone-sensitive lipase → releases fatty acids from adipose
- Ketogenesis: Promotes fatty acid oxidation → ketone bodies in liver
- Protein catabolism: Promotes amino acid release from muscle for gluconeogenesis
Glucagon Metabolism
- Half-life: 3-6 minutes
- Degraded primarily by: liver (first pass, ~60% removed) and kidneys
- Mechanism: Proteolytic degradation by liver proteases + renal clearance
PART 8: SOMATOSTATIN
What is somatostatin?
- δ (delta) cells of the pancreatic islets
- D cells of the stomach and intestine
- Hypothalamus (inhibits growth hormone from pituitary)
Structure
- Two forms: SS-14 (14 amino acids) and SS-28 (28 amino acids)
- Both are cyclic peptides (linked by a disulfide bridge)
- SS-14 predominates in pancreas; SS-28 predominates in intestine
What Triggers Somatostatin Release?
- High glucose, amino acids, fatty acids after a meal
- Other GI hormones (CCK, secretin)
- High glucagon or insulin (local paracrine effect)
Somatostatin's Effects
| Target | Effect |
|---|---|
| Pancreatic β cells | Inhibits insulin secretion |
| Pancreatic α cells | Inhibits glucagon secretion |
| Pituitary | Inhibits GH and TSH release |
| Stomach | Inhibits gastrin, HCl, pepsin secretion |
| Intestine | Inhibits secretin, CCK, VIP, motilin |
| Liver | Inhibits bile flow |
| GI motility | Slows gastric emptying, reduces splanchnic blood flow |
Mechanism of Action
- Somatostatin receptors (SSTR1-5) are GPCRs coupled to Gi (inhibitory)
- Gi → inhibits adenylyl cyclase → cAMP ↓ → PKA activity ↓
- Also: Opens K⁺ channels → hyperpolarization → inhibits Ca²⁺ entry → inhibits exocytosis
Somatostatin Metabolism
- Half-life: extremely short, 1-3 minutes in circulation
- Degraded by peptidases in blood and tissues
- This is why octreotide (t½ 1.5 hours) and lanreotide (monthly depot) were developed
- Clinical uses: acromegaly, carcinoid tumors, VIPomas, glucagonomas, bleeding esophageal varices
PART 9: GLUT TRANSPORTERS
What are GLUT transporters?
The Key GLUT Transporters
| GLUT | Location | Km for Glucose | Characteristics | Regulation |
|---|---|---|---|---|
| GLUT1 | RBCs, brain (BBB), placenta, fetal tissues | 1 mM (high affinity) | Constitutive; baseline glucose transport | Not insulin-regulated |
| GLUT2 | Liver, pancreatic β-cells, kidney, small intestine | 15-20 mM (low affinity) | "Glucose sensor" - transports only when glucose abundant | Not insulin-regulated |
| GLUT3 | Neurons (brain) | 1 mM (high affinity) | Ensures neurons ALWAYS get glucose | Constitutive |
| GLUT4 | Skeletal muscle, cardiac muscle, adipose tissue | 5 mM | The insulin-regulated transporter; stored in intracellular vesicles | Insulin-dependent! |
| GLUT5 | Small intestine, sperm | High Km | Fructose transporter (not glucose) | Constitutive |
The Magic of GLUT4
Insulin → IR → IRS-1 → PI3K → PIP3 → Akt → phosphorylates AS160
↓
TBC1D4 (AS160) inactivated
↓
Rab-GTPase proteins activated
↓
GLUT4 vesicles traffic to plasma membrane
↓
GLUT4 fuses with membrane (exocytosis) - increases 10-20 fold
↓
Glucose floods into muscle/fat cell
PART 10: LABORATORY DIAGNOSIS OF DIABETES MELLITUS
ADA Diagnostic Criteria (any ONE on TWO separate days, except symptomatic random glucose):
| Test | Diabetes | Prediabetes | Normal |
|---|---|---|---|
| Fasting Plasma Glucose (FPG) | ≥ 126 mg/dL (7.0 mmol/L) | 100-125 mg/dL (IFG) | < 100 mg/dL |
| 2-hr Plasma Glucose (OGTT) | ≥ 200 mg/dL (11.1 mmol/L) | 140-199 mg/dL (IGT) | < 140 mg/dL |
| HbA1c | ≥ 6.5% (48 mmol/mol) | 5.7-6.4% | < 5.7% |
| Random Plasma Glucose | ≥ 200 mg/dL WITH symptoms | - | - |
PART 11: ORAL GLUCOSE TOLERANCE TEST (OGTT)
Procedure
- Patient fasts 8-14 hours overnight; normal carbohydrate diet (≥150g/day) for 3 days prior; no heavy exercise 3 days prior
- Fasting blood sample taken
- Patient drinks 75g anhydrous glucose dissolved in 250-300 mL water (within 5 minutes)
- Blood samples taken at 1 hour and 2 hours
- Patient sits quietly, no smoking during test
Interpretation
| 2-hour value | Interpretation |
|---|---|
| < 140 mg/dL | Normal glucose tolerance |
| 140-199 mg/dL | IGT (Impaired Glucose Tolerance) = Prediabetes |
| ≥ 200 mg/dL | Diabetes Mellitus |
For Gestational Diabetes (GDM)
- 2-step approach (USA): 50g glucose screen at 24-28 weeks → if ≥130-140 mg/dL at 1 hr → 100g 3-hour OGTT
- 1-step approach (international): 75g OGTT directly; GDM if fasting ≥92, 1-hr ≥180, 2-hr ≥153 mg/dL
PART 12: HbA1c (GLYCATED HEMOGLOBIN)
What is HbA1c?
High blood glucose + Hemoglobin A
↓ (non-enzymatic, irreversible, SLOW process)
Schiff base (unstable)
↓ Amadori rearrangement
HbA1c (stable ketoamine)
Why does it reflect 3-month glucose control?
- RBCs live for approximately 120 days (3 months)
- Every day the RBC lives, more glucose attaches to hemoglobin
- The amount of HbA1c reflects the average glucose the RBC has been exposed to over its entire lifetime
- HbA1c is a "memory" of blood glucose for the past 2-3 months
- It reflects the last 30 days more heavily (because younger RBCs are more abundant)
Reference Values
| HbA1c | Interpretation |
|---|---|
| < 5.7% | Normal |
| 5.7 - 6.4% | Prediabetes |
| ≥ 6.5% | Diabetes mellitus (diagnostic) |
| Target < 7% | Diabetic treatment goal (ADA) |
| > 8% | Poor control, risk of complications |
HbA1c to Average Blood Glucose Correlation
| HbA1c | Estimated Average Glucose |
|---|---|
| 6% | 126 mg/dL |
| 7% | 154 mg/dL |
| 8% | 183 mg/dL |
| 9% | 212 mg/dL |
| 10% | 240 mg/dL |
Conditions That Falsely Alter HbA1c
| Condition | Effect on HbA1c | Reason |
|---|---|---|
| Hemolytic anemia | ↓ False low | RBCs destroyed faster → less time for glycation |
| Iron deficiency anemia | ↑ False high | RBCs live longer → more time for glycation |
| Hemoglobin variants (HbS, HbC) | Unreliable | Interfere with assay |
| Pregnancy (2nd/3rd trimester) | ↓ False low | Increased RBC turnover |
| Blood transfusion | ↓ False low | Dilutes patient's own RBCs |
| High-dose vitamin C/E | ↓ False low | Inhibit glycation |
PART 13: METABOLISM OF INSULIN, GLUCAGON & SOMATOSTATIN
Insulin Metabolism
- Normal fasting insulin: 5-15 μU/mL
- After a meal, peaks at 50-100 μU/mL
- Daily secretion: ~40-50 units/day
- Half-life: ~5-8 minutes
- Liver - most important (~50% of portal insulin removed in FIRST PASS)
- Kidneys - second (~30-40% of peripheral insulin)
- Muscle, adipose - minor
- Kidney disease → insulin half-life prolonged → LESS insulin needed (risk of hypoglycemia)
- Liver disease → reduced first-pass extraction → HIGHER systemic insulin levels
Glucagon Metabolism
- Normal fasting glucagon: 75-150 pg/mL
- Half-life: 3-6 minutes
- Liver is the primary degradation site (60% removed in first pass)
- Kidneys are secondary
- Mechanism: Proteolytic degradation by liver enzymes + renal clearance
Somatostatin Metabolism
- Half-life: 1-3 minutes (shortest of all three)
- Mainly acts locally (paracrine) rather than as a true circulating hormone
- Degradation: Plasma peptidases + liver + kidney clearance
- Clinical consequence: Natural hormone is useless therapeutically → synthetic analogs needed:
- Octreotide (t½ ~1.5 hours, SubQ injection 3x/day)
- Lanreotide (depot injection, monthly)
- Pasireotide (broader SSTR subtype binding, used in Cushing's disease)
QUICK REFERENCE MASTER TABLE
| Hormone | Made by | Chemical Nature | Receptor Type | Half-life | Main Action |
|---|---|---|---|---|---|
| Cortisol | Adrenal zona fasciculata | Steroid (C21) | Nuclear | 60-90 min | Gluconeogenesis, anti-inflammatory |
| Aldosterone | Adrenal zona glomerulosa | Steroid (C21) | Nuclear | 15-20 min | Na⁺ retention, K⁺ excretion |
| Testosterone | Testes (Leydig cells) | Steroid (C19) | Nuclear | 2-4 hours | Virilization, anabolism |
| Estradiol | Ovaries (granulosa) | Steroid (C18) | Nuclear | 1-2 hours | Female reproductive |
| T4 (Thyroxine) | Thyroid follicular cells | Iodinated amino acid | Nuclear (after → T3) | 6-7 days | Metabolic rate (prohormone) |
| T3 | Peripheral conversion | Iodinated amino acid | Nuclear | 18 hours | Metabolic rate (active) |
| PTH | Parathyroid chief cells | Polypeptide (84 AA) | GPCR (Gs+Gq) | 2-4 min | Raise blood calcium |
| Insulin | Pancreatic β cells | Polypeptide (51 AA) | Receptor tyrosine kinase | 5-8 min | Lower blood glucose, anabolic |
| Glucagon | Pancreatic α cells | Polypeptide (29 AA) | GPCR (Gs → cAMP) | 3-6 min | Raise blood glucose, catabolic |
| Somatostatin | Pancreatic δ cells | Cyclic peptide (14 or 28 AA) | GPCR (Gi → ↓cAMP) | 1-3 min | Inhibit insulin, glucagon, GH |
10 Key Concepts to Always Remember
- All steroid hormones come from cholesterol; the rate-limiting step is StAR protein moving cholesterol into mitochondria.
- Thyroid hormone synthesis needs iodine + TPO enzyme; T4 is a prohormone, T3 is the active hormone.
- TSH is the most sensitive thyroid test; low TSH = overactive gland, high TSH = underactive gland.
- PTH raises calcium AND lowers phosphate; Vitamin D raises both; FGF-23 lowers phosphate.
- Insulin is made as preproinsulin → proinsulin → insulin + C-peptide (released in equimolar amounts).
- GLUT2 is the glucose sensor in β cells (low affinity, high capacity); GLUT4 is insulin-regulated in muscle/fat.
- C-peptide helps distinguish endogenous insulin production from exogenous injection; also a marker of beta cell reserve.
- HbA1c reflects average blood glucose over 120 days (RBC lifespan); ≥6.5% = diabetes; target <7% in treatment.
- Glucagon → GPCR → cAMP → PKA → glycogenolysis + gluconeogenesis in liver.
- Somatostatin = master inhibitor of both insulin and glucagon via Gi → ↓cAMP; half-life only 1-3 minutes.