Explain me 10 common heart diseases with ECG changes and ECG images of those diseases
Reading File
Finding Sources
Searching the Web
10 common heart diseases ECG changes electrocardiogram findings
Finding Sources
Finding Sources
Searching the Web
ECG images STEMI atrial fibrillation heart block hypertrophic cardiomyopathy pericarditis
Finding Sources
Searching the Web
ECG example images heart failure LVH Wolff-Parkinson-White long QT syndrome ventricular tachycardia
Reading File
Finding Sources
Searching the Web
site:litfl.com ECG STEMI atrial fibrillation pericarditis images
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Loading Image
Finding Sources
Searching the Web
ECG images STEMI inferior anterior pericarditis long QT complete heart block litfl OR ecgwaves
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Loading Image
Reading File
Loading Image
Reading File
I now have rich textbook content and real ECG images. Let me compile the comprehensive answer.
10 Common Heart Diseases: ECG Changes and Images
1. ST-Elevation Myocardial Infarction (STEMI)
Pathophysiology: Complete occlusion of a coronary artery causes transmural myocardial ischemia and necrosis.
ECG Changes:
| Phase | Finding |
|---|---|
| Hyperacute (minutes) | Tall, broad "hyperacute" T waves before ST elevation |
| Acute (hours) | ST elevation in the territory of the infarcted artery; reciprocal ST depression in opposite leads |
| Evolved (hours-days) | Pathological Q waves (>40 ms wide, >25% of R wave) develop; T-wave inversion |
| Chronic | Persistent Q waves; ST normalizes |
Location-based criteria (from Tintinalli's Emergency Medicine):
- Anteroseptal: ST elevation V1-V3
- Anterior: ST elevation V1-V4
- Anterolateral: ST elevation V1-V6, I, aVL
- Inferior: ST elevation II, III, aVF (always get right-sided leads to exclude RV infarction)
- Right ventricular: ST elevation in RV leads V3R-V6R
- Posterior: Tall R wave in V1-V2, R/S ratio ≥1 (mirror image STEMI)

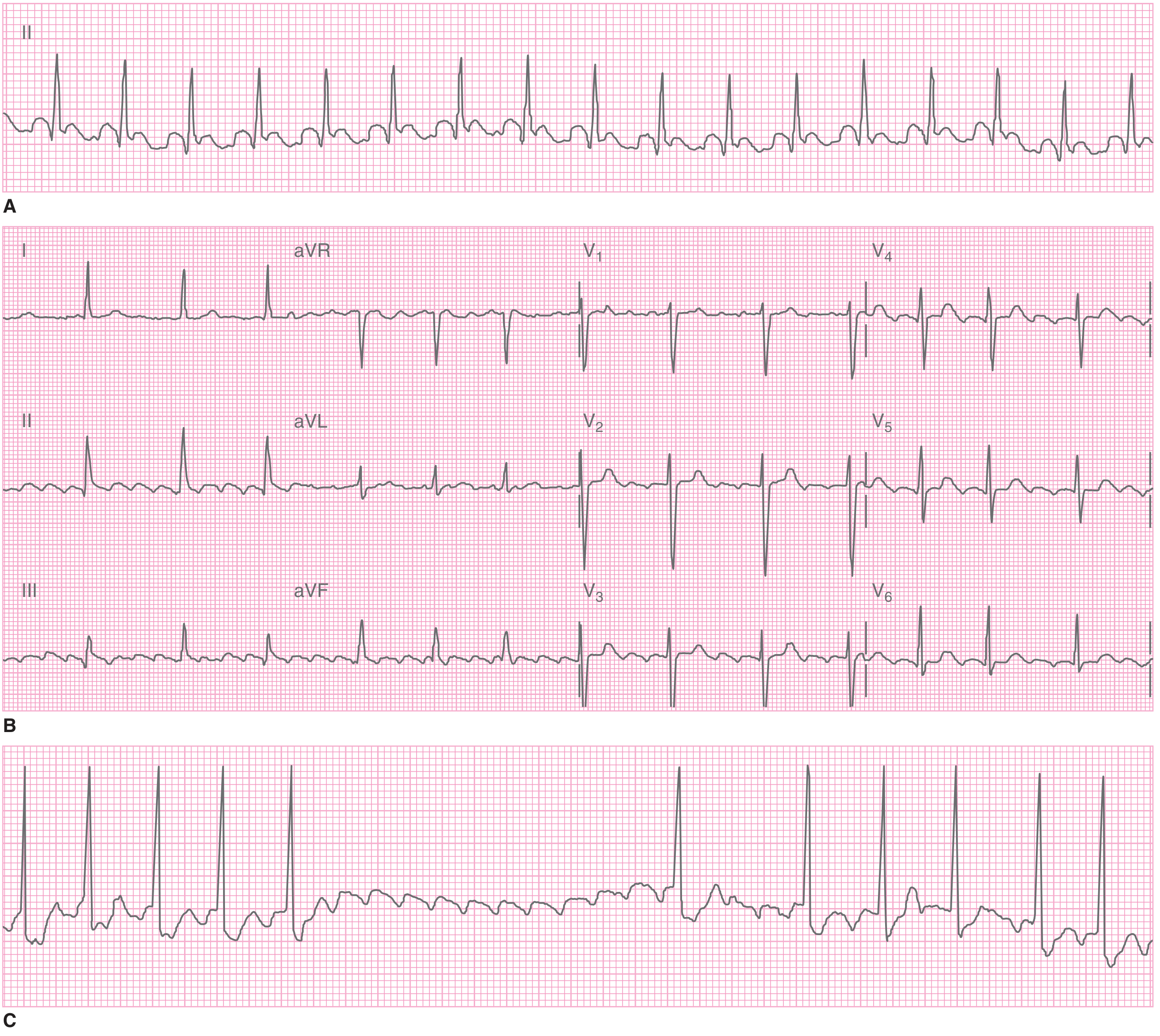
2. Atrial Fibrillation (AF)
Pathophysiology: Chaotic, disorganized atrial electrical activity with multiple re-entrant wavelets replacing organized P-wave-driven atrial contraction.
ECG Changes:
From the Tintinalli's Emergency Medicine (Table 18-8):
| Feature | Description |
|---|---|
| P waves | Absent - replaced by irregular, chaotic fibrillatory baseline |
| Baseline | Flat or chaotic (fine or coarse AF) |
| QRS | Narrow unless pre-existing bundle branch block or accessory pathway (WPW) |
| RR interval | Irregularly irregular - the hallmark of AF |
| Ventricular rate | Usually 100-160 bpm if uncontrolled |
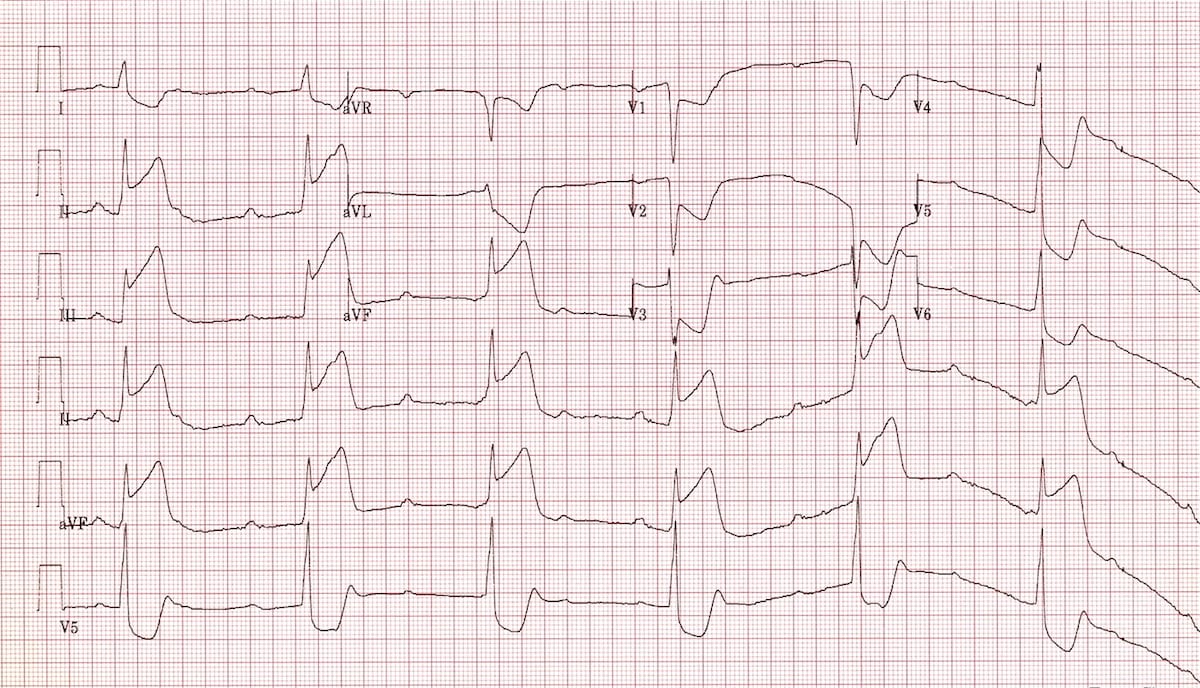
3. Acute Pericarditis
Pathophysiology: Inflammation of the pericardial sac (usually viral) causes widespread sub-epicardial injury producing characteristic diffuse ST changes.
ECG Changes (4 Stages):
| Stage | Timing | ECG Findings |
|---|---|---|
| Stage 1 | Days 1-2 | Diffuse concave (saddle-shaped) ST elevation in most leads; PR depression in II, V4-V6; PR elevation in aVR; no reciprocal ST depression (except aVR, V1) |
| Stage 2 | Days 1-3 | ST normalizes; T waves flatten |
| Stage 3 | Days 1-3 | Diffuse T-wave inversions |
| Stage 4 | Weeks-months | ECG normalizes |
Key distinguisher from STEMI: Pericarditis has concave (saddle-shaped) ST elevation in virtually all leads simultaneously - STEMI has convex elevation localized to one territory.

4. Complete (Third-Degree) AV Heart Block
Pathophysiology: Complete failure of conduction between atria and ventricles - the atria and ventricles beat independently at their own intrinsic rates.
ECG Changes:
- P waves: Regular at normal atrial rate (60-100 bpm), independent of QRS complexes
- QRS complexes: Slow escape rhythm: narrow (40-60 bpm) if junctional; wide and bizarre (20-40 bpm) if ventricular
- AV dissociation: P waves "march through" QRS complexes with no fixed PR relationship
- Cannon A waves may be noted clinically
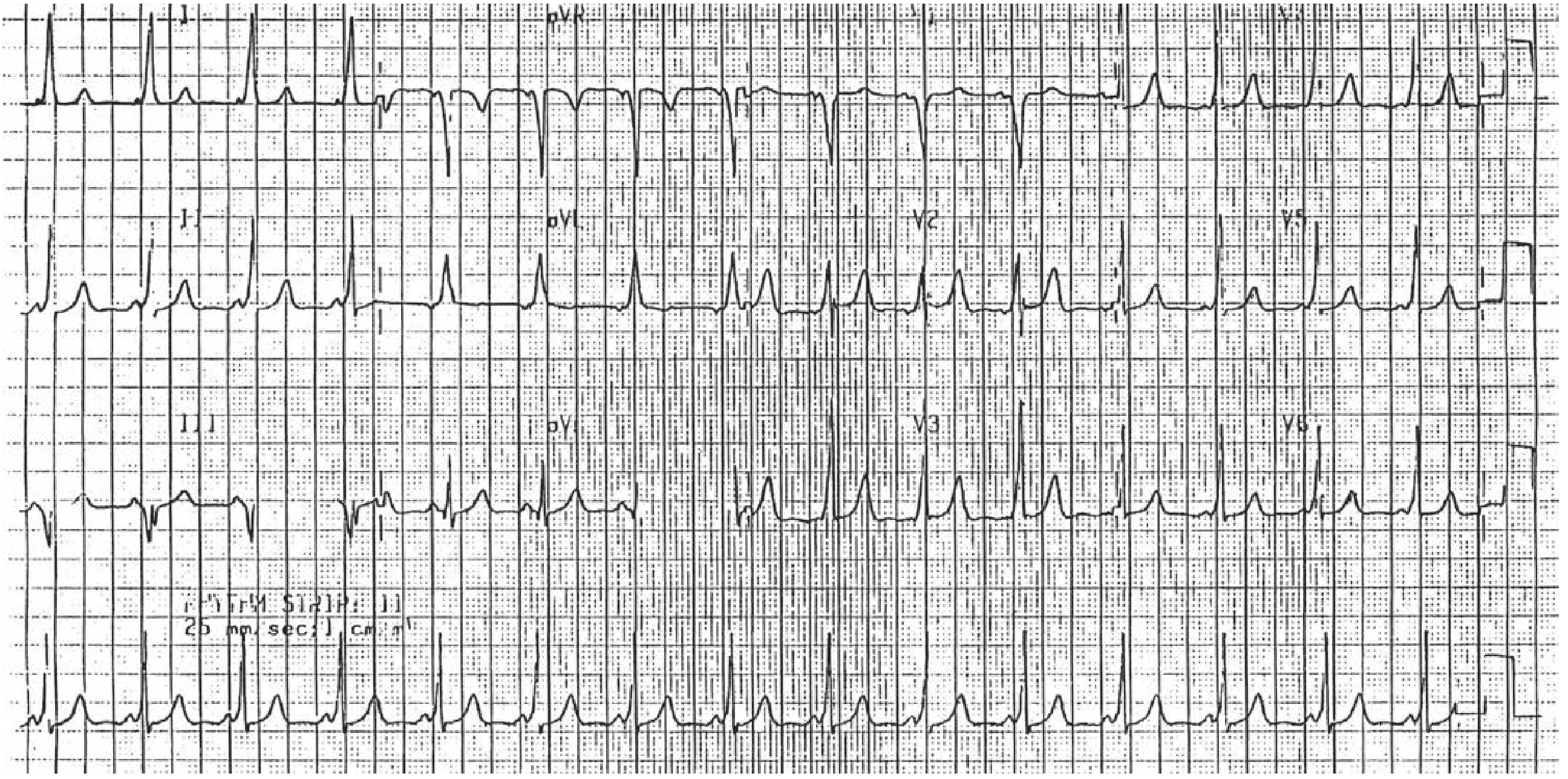
5. Left Ventricular Hypertrophy (LVH)
Pathophysiology: Chronic pressure overload (hypertension, aortic stenosis) causes increased left ventricular mass, producing larger electrical potentials on ECG.
ECG Changes (Harrison's Principles, 22nd Ed.):
- Sokolow-Lyon criteria: SV1 + RV5 or RV6 > 35 mm
- Cornell criteria: RaVL > 20 mm (women) or > 28 mm (men); or SV3 + RaVL > 28 mm (men), > 20 mm (women)
- Repolarization changes: ST depression + T-wave inversion in lateral leads (I, aVL, V5-V6) - formerly called "LV strain pattern"
- Left atrial abnormality (broad notched P wave in II, negative terminal deflection in V1) often accompanies LVH
- LVH often progresses to left bundle branch block (LBBB)
6. Wolff-Parkinson-White (WPW) Syndrome
Pathophysiology: An accessory pathway (Bundle of Kent) bypasses the AV node, causing ventricular pre-excitation. The ventricles are activated early via the bypass tract AND through the normal AV node.
ECG Changes (Tintinalli's Emergency Medicine, Fig. 130-1):
- Short PR interval: < 120 ms (pre-excitation bypasses AV nodal delay)
- Delta wave: Slurred, broad upstroke at the start of the QRS (accessory pathway depolarization)
- Widened QRS: > 120 ms (due to delta wave + fusion complex)
- Secondary ST-T changes in opposite direction to delta wave
- During AF with WPW: Irregular, very rapid wide-complex rhythm (>250 bpm) - life-threatening
7. Long QT Syndrome (LQTS)
Pathophysiology: Inherited (channelopathy) or acquired (drug-induced, electrolyte disorders) prolongation of ventricular repolarization, predisposing to torsade de pointes (TdP) and sudden cardiac death.
ECG Changes (Tintinalli's Emergency Medicine):
- Prolonged QTc: > 440 ms (men), > 460 ms (women); risk of events rises sharply at QTc > 500 ms
- Notched T waves in 3 or more leads (particularly LQT2)
- Prominent U waves (especially LQT3)
- T-wave alternans: Beat-to-beat variation in T-wave morphology (sign of electrical instability)
- Torsade de pointes: Polymorphic VT where QRS complexes rotate around the isoelectric baseline ("twisting of the points") - can degenerate to VF
Common causes of acquired LQTS: Macrolide antibiotics, fluoroquinolones, antipsychotics (haloperidol, quetiapine), antiarrhythmics (amiodarone, sotalol), hypokalemia, hypomagnesemia.
8. Hypertrophic Cardiomyopathy (HCM)
Pathophysiology: Genetic mutation (usually sarcomere proteins) causes asymmetric LV hypertrophy, diastolic dysfunction, and dynamic LVOT obstruction.
ECG Changes:
- LVH voltage criteria - often very prominent (Sokolow-Lyon > 35 mm)
- Deep, narrow ("dagger-like") Q waves in lateral and inferior leads (II, III, aVF, V4-V6) - due to septal hypertrophy (not infarction)
- T-wave inversions in lateral and/or anterior leads
- Left atrial abnormality
- Apical HCM (Yamaguchi variant): Giant, deeply inverted T waves in precordial leads V3-V5 (called "giant negative T waves"), with tall R waves - a distinct pattern
- Arrhythmias: AF, SVT, ventricular arrhythmias
- Normal ECG is present in ~5-10% of patients with HCM
9. Pulmonary Embolism (PE)
Pathophysiology: Sudden obstruction of pulmonary vasculature causes acute right ventricular pressure overload and dilation.
ECG Changes (Harrison's Principles, 22nd Ed.):
- Sinus tachycardia - most common finding (present in >40%)
- S1Q3T3 pattern: Prominent S wave in lead I + Q wave in lead III + T-wave inversion in lead III (classic but present in only ~20%)
- Right axis deviation (RAD)
- Right bundle branch block (RBBB): New or incomplete RBBB
- T-wave inversions in V1-V4 (right ventricular strain pattern - the most sensitive sign of large PE)
- P pulmonale: Tall peaked P wave in II, III, aVF (right atrial enlargement)
- Atrial fibrillation or flutter may occur
- Normal ECG does NOT exclude PE
10. Ventricular Tachycardia (VT)
Pathophysiology: Rapid ventricular rhythm originating from the ventricular myocardium or conduction system below the His bundle, usually in the context of ischemic heart disease or cardiomyopathy.
ECG Changes:
| Feature | Description |
|---|---|
| Rate | 100-250 bpm |
| QRS | Wide (>120 ms), bizarre morphology |
| Regularity | Usually regular |
| AV dissociation | P waves march independently through QRS (diagnostic when seen) |
| Fusion beats | P wave conducts partially through normal pathway fusing with VT complex (diagnostic) |
| Capture beats | Occasional narrow QRS from supraventricular capture (diagnostic) |
| Concordance | All precordial QRS complexes pointing same direction (positive or negative) - highly specific for VT |
Distinction from SVT with aberrancy: Brugada criteria: (1) no RS in precordial leads, (2) RS interval >100 ms in any precordial lead, (3) AV dissociation, (4) morphology criteria - any one positive = VT.
Torsade de pointes (TdP): Polymorphic VT - QRS twists around baseline, seen in LQTS.
Quick Reference Summary Table
| Disease | Key ECG Features |
|---|---|
| STEMI | ST elevation in culprit territory + reciprocal depression + Q waves |
| Atrial Fibrillation | Absent P waves, irregularly irregular RR, narrow QRS |
| Pericarditis | Diffuse concave ST elevation, PR depression, all leads affected |
| Complete Heart Block | AV dissociation, slow escape rhythm, P waves independent of QRS |
| LVH | High voltage (SV1+RV5 >35mm), lateral strain pattern (ST depression + T inversion) |
| WPW | Short PR, delta wave, widened QRS |
| Long QT | QTc >500ms, notched T waves, U waves, risk of TdP |
| HCM | LVH + deep lateral Q waves + giant T inversions (apical variant) |
| Pulmonary Embolism | S1Q3T3, sinus tachycardia, RV strain (V1-V4 T inversions), RBBB |
| Ventricular Tachycardia | Wide QRS tachycardia, AV dissociation, fusion/capture beats |
Sources: Tintinalli's Emergency Medicine (9th Ed.) - Tables 18-8, 49-4, 130-1; Harrison's Principles of Internal Medicine (22nd Ed., 2025) - Chapters 247; LITFL ECG Library
This is a shared conversation. Sign in to Orris to start your own chat.