Osteoarthritis, proper physiotherapy management and related medicine
Reading File
Finding Sources
Finding Sources
Searching PubMed
"osteoarthritis"[MeSH Terms] AND "physical therapy"[MeSH Terms]
Reading File
Reading File
Finding Sources
Searching PubMed
"osteoarthritis"[MeSH Terms] AND "exercise therapy"[MeSH Terms]
Reading File
Reading File
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
I now have all the content needed for a comprehensive answer. Let me compile the complete response.
Osteoarthritis: Pathophysiology, Physiotherapy Management & Pharmacology
Definition & Overview
Osteoarthritis (OA) is characterized by failed repair of synovial joint tissues after intra-articular stress. The resulting breakdown of cartilage and bone leads to pain, stiffness, and functional disability. It affects >500 million people worldwide and is the 15th highest cause of years lived with disability globally. Knee OA accounts for ~85% of the total OA burden; the lifetime risk is 40% in men and 47% in women.
— Goldman-Cecil Medicine, Ch. 241
Pathobiology
OA involves structural alterations in articular cartilage, subchondral bone, synovium, ligaments, capsule, and periarticular muscles — a dynamic interplay of mechanical, inflammatory, and metabolic pathways.
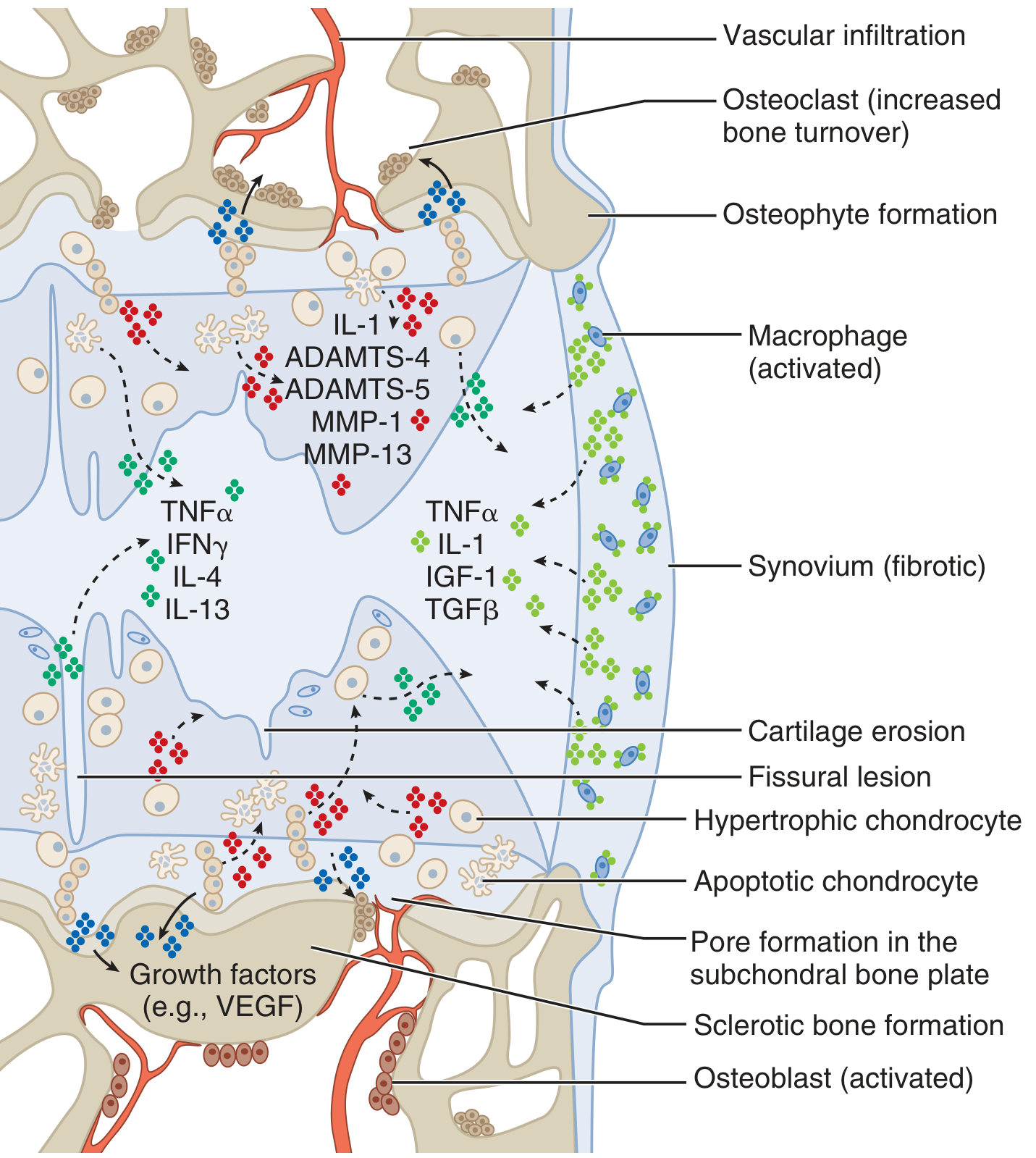
Key cellular events:
- Proteoglycan loss → cartilage swelling → disruption of type II collagen matrix
- Deep cartilage fissures + expansion of the calcified zone
- Hypertrophic chondrocytes release MMPs (MMP-1, MMP-13) and ADAMTS-4/5 (aggrecanases)
- Proinflammatory cytokines: IL-1, TNF-α, IL-4, IL-13, IFN-γ
- Subchondral: osteoclast activation → sclerotic bone, osteophyte formation, VEGF-driven vascular infiltration
- Synovium becomes fibrotic with macrophage and lymphocyte infiltration
Pain mechanisms follow a biopsychosocial model: peripheral nociception (loading of damaged joint) + central sensitization (neuropathic upregulation) — which is why standard analgesics sometimes fail and centrally-active agents may be needed.
Clinical Features
| Feature | Detail |
|---|---|
| Pain onset | Gradual; worse with use, relieved by rest |
| Stiffness | <30 min (morning or after inactivity — "gel phenomenon") |
| Signs | Crepitus, bony enlargement, Heberden nodes (DIP), Bouchard nodes (PIP), reduced ROM |
| Joints most affected | Knee, hip, hand (DIP/PIP/1st CMC), 1st MTP, spine |
| Distinguishing feature | NO systemic symptoms, no significant warmth/erythema |
Classification criteria for knee OA (ACR): knee pain + ≥3 of: age >50, stiffness <30 min, crepitus, bony tenderness, bony enlargement, no warmth → 95% sensitive, 69% specific.
Management Framework
Core principle: Active non-pharmacologic interventions are the mainstay; medications are adjuncts for persistent or severe symptoms. Management must be individually tailored.
I. Physiotherapy Management
A. Exercise Therapy (Core — Highest Evidence)
Exercise is the single most important, evidence-based intervention in OA. A 2024 Cochrane systematic review confirms exercise significantly reduces pain and improves function in knee OA. A 2025 BMJ network meta-analysis compared modalities and found combined aerobic + strengthening most effective.
| Exercise Type | Joints | Details |
|---|---|---|
| Aerobic exercise | Knee, Hip | Walking, cycling (stationary/outdoor), power walking, swimming — any activity raising heart rate |
| Strengthening | Hand, Knee, Hip | Quadriceps, hip abductors — via body weight, resistance bands, free weights, machines. Squats, seated knee extension |
| Neuromuscular / balance | Knee, Hip | Wobble boards, single-leg balancing, soft surface walking — improves proprioception & dynamic stability |
| Water-based (hydrotherapy) | Knee, Hip | Aqua aerobics, deep water running, hydrotherapy pool — low-impact, ideal for severe OA or obesity |
| Tai Chi / Yoga | Knee, Hip | Mind-body exercises with breathing coordination and mindfulness; evidence for pain and balance |
| Joint mobility & stability | Hand, Knee, Hip | Range-of-motion exercises, thumb base stability for hand OA |
| General physical activity | All | Walking, gardening, dancing, cycling to work |
Weak quadriceps may precede knee OA onset, underlining biomechanical importance of early strengthening. >44% of OA patients are currently inactive — activity promotion is essential.
B. Manual Therapy
Physiotherapists may apply joint mobilization and manipulation to improve ROM and reduce pain, used alongside exercise (not as a standalone).
C. TENS (Transcutaneous Electrical Nerve Stimulation)
Electrical stimulation has shown moderate improvement: ~25% improvement in knee OA, ~12% in cervical OA.
— Textbook of Family Medicine 9e
D. Thermal Modalities
- Heat: Superficial heat (hot packs, warm baths) for chronic stiffness
- Cold: Ice packs for acute flares and post-exercise swelling
E. Assistive Devices & Orthotics
- Walking aids (cane, walker) — reduce joint loading
- Bracing — indicated for varus/valgus malalignment (medial/lateral unloading brace for knee OA)
- Foot orthotics — lateral-wedge insoles for medial compartment knee OA; podiatry referral for abnormal foot posture
- Gait retraining — particularly if varus thrust is seen during gait
F. Patient Education & Self-Management
Patients should understand the disease process, set realistic goals, and participate in decision-making. Referral to self-management programs improves long-term adherence.
G. Weight Management
- BMI >25 or waist >80 cm (women) / >94 cm (men) → counsel for 5–10% weight reduction
- Diet + aerobic/strengthening exercise combination
- Refer to dietitian as needed
- Weight loss reduces mechanical joint load and systemic inflammatory adipokines
II. Pharmacologic Treatment
Step 1: Topical Agents (Preferred First-line Systemic Sparing)
| Drug | Notes |
|---|---|
| Topical NSAIDs (diclofenac gel/patch) | First preference over oral NSAIDs — equivalent efficacy for knee OA with minimal systemic absorption |
| Topical capsaicin | Depletes substance P; useful adjunct for hand/knee OA |
Step 2: Oral Analgesics
| Drug | Dose / Notes |
|---|---|
| Acetaminophen (paracetamol) | First-line oral analgesic; 500–1000 mg TID-QID; safer GI/CV profile than NSAIDs |
| Oral NSAIDs (ibuprofen, naproxen, diclofenac, celecoxib) | First-line for moderate–severe OA pain; use at lowest effective dose for shortest duration; COX-2 inhibitors (celecoxib) preferred in GI-risk patients |
| Duloxetine | SNRI; effective for central sensitization phenotype; also treats comorbid depression/anxiety |
| Tramadol | Weak opioid; consider when NSAIDs/acetaminophen fail; avoid long-term use |
Opioids have at most very modest benefit in OA and carry significant risks — reserve only for end-stage disease awaiting surgery.
Step 3: Intra-Articular Injections
| Injection | Evidence |
|---|---|
| Corticosteroids (triamcinolone, methylprednisolone) | Short-term (4–6 weeks) pain relief; Grade B evidence; repeat injections have diminishing returns and potential cartilage concerns |
| Hyaluronic acid (viscosupplementation) — Hyalgan, Synvisc | FDA approved for knee OA; onset takes weeks, lasts up to 6 months; meta-analyses show minimal benefit vs. placebo |
| Platelet-rich plasma (PRP) | Not of documented benefit; evidence insufficient |
Supplements (Adjuncts)
| Supplement | Notes |
|---|---|
| Glucosamine sulfate 1500 mg/day | Stimulates proteoglycan synthesis; sulfate form (not HCl) shows modest benefit in pain and radiographic joint space preservation |
| Chondroitin sulfate 1200 mg/day | Some evidence for hand OA; less consistent for knee |
| S-adenosylmethionine (SAMe) | As effective as NSAIDs in some meta-analyses; do not use at bedtime (stimulant effect) |
| Avocado-soybean unsaponifiables | Cochrane review: beneficial effects on function and NSAID intake |
Step 4: Surgical Referral
Refer to orthopedic surgery when all conservative options have failed:
- Pain disrupting sleep
- Severely reduced walking distance
- Markedly restricted ADLs
- Significantly reduced quality of life
Total joint replacement (TKR / THR) is the definitive option for end-stage OA.
III. Newer & Emerging Options
- Sprifermin (recombinant FGF-18 intra-articular injection): increases femorotibial cartilage thickness in trials; no symptomatic benefit yet confirmed
- Research into disease-modifying OA drugs (DMOADs) targeting IL-1, MMPs, and ADAMTS pathways is ongoing
Holistic Assessment Checklist (Practical Guide)
| Domain | Action |
|---|---|
| Joint symptoms | Differential diagnosis; consider imaging if atypical |
| Comorbidities | CVD/renal/hepatic disease influences NSAID selection |
| Psychological screen | Treat depression/anxiety (duloxetine serves double purpose) |
| Muscle strength | Prescribe strengthening; physio referral if weak quadriceps |
| BMI/obesity | Dietary + exercise intervention; dietitian referral |
| Falls risk | Gait aid, footwear advice, balance training |
| Foot posture | Orthotics/podiatry if abnormal |
| Patient expectations | Education, realistic goal-setting, self-management programs |
Recent Evidence Update
- Cochrane 2024 — Exercise for knee OA (PMID 39625083): Exercise significantly reduces pain and improves function; supports current guidelines
- BMJ 2025 — Network meta-analysis (PMID 41093618): Combined aerobic + resistance exercise is the most efficacious modality
- J Evid Based Med 2024 — Knee OA evaluation & management (PMID 38963824): Systematic review confirming multimodal approach superiority
Sources: Goldman-Cecil Medicine (26th ed.), Textbook of Family Medicine (9th ed.), Robbins & Kumar Basic Pathology
This is a shared conversation. Sign in to Orris to start your own chat.