Community acquired pneumonia
Reading File
Finding Sources
Searching PubMed
"community-acquired pneumonia"[MeSH Terms] AND management
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
Reading File
Reading File
Reading File
Reading File
I now have comprehensive material from Goldman-Cecil, Harrison's 2025, Tintinalli, and Fishman's. Let me compile the full response.
Community-Acquired Pneumonia (CAP)
Definition
CAP is an acute infection of the alveolar (gas-exchanging) portion of the lung acquired outside of a hospital or long-term care facility (or within 14 days of leaving one). It is one of the most common serious health conditions and the most common infectious cause of hospitalization and death in the United States, accounting for roughly 3 million cases and 1.6 million hospitalizations annually. - Tintinalli's Emergency Medicine, p. 481
Pathophysiology
Pathogenic organisms reach the lungs via three main routes:
- Aspiration of oropharyngeal flora - the most common route
- Inhalation of airborne droplets
- Hematogenous seeding (e.g., S. aureus, S. pneumoniae via bacteremia)
Once inoculated, organisms trigger an intense inflammatory response. Alveoli fill with exudate and WBCs, producing the classic consolidation pattern. Organisms spread via the bronchial tree or through Kohn's pores between alveoli. - Tintinalli's, p. 482
Risk factors for pneumonia:
- Aspiration risk: stroke, swallowing disorders, nasogastric tube, seizure, intubation
- Impaired mucociliary clearance: smoking, COPD, bronchiectasis
- Bacteremia risk: indwelling vascular devices, debilitation
- Systemic: extremes of age, alcoholism, malnutrition, immunosuppression, malignancy
Microbiology (Etiology)
In >50% of CAP cases, no pathogen is ever confirmed. Among identified pathogens (pre-SARS-CoV-2 era): - Goldman-Cecil Medicine, p. 990
| Category | Pathogen | Frequency |
|---|---|---|
| Typical bacteria | S. pneumoniae | 5-16% |
| H. influenzae | <1-7% | |
| S. aureus | 3-5% | |
| P. aeruginosa | <1-3% | |
| K. pneumoniae | <1% | |
| Atypical bacteria | M. pneumoniae | 1-2% |
| C. pneumoniae | 1-2% | |
| Legionella spp. | ~1% | |
| Viruses | Human rhinovirus | 9-13% |
| Influenza A/B | 1-6% | |
| Human metapneumovirus | 2-4% | |
| RSV | 2-3% |
Organism-specific clues:
| Organism | Clinical Features | Sputum | CXR |
|---|---|---|---|
| S. pneumoniae | Sudden onset, rigors, pleuritic pain, productive cough | Rust-colored; gram-positive diplococci | Lobar consolidation |
| S. aureus | Gradual onset post-viral illness | Purulent; gram-positive cocci in clusters | Patchy multilobar; empyema, abscess |
| K. pneumoniae | Sudden onset, bloody sputum; alcoholics/nursing home | "Currant jelly"; thick gram-negative coccobacilli | Upper lobe; bulging fissure sign, abscess |
| Legionella | Fever, diarrhea, GI symptoms, hyponatremia | Few neutrophils, no dominant organism | Patchy nonsegmental; progresses to consolidation |
| M. pneumoniae | Upper + lower tract symptoms; bullous myringitis, headache | Organisms invisible | Interstitial (reticulonodular) pattern |
| Anaerobes | Gradual onset, putrid sputum; alcoholics | Mixed organisms | Consolidation of dependent zone; abscess |
- Tintinalli's Emergency Medicine, p. 482
Clinical Presentation
Typical CAP (pneumococcal pattern): Abrupt onset, high fever, rigors, pleuritic chest pain, productive cough with purulent/rust sputum, dyspnea.
Atypical CAP (Mycoplasma, Chlamydia, Legionella): More indolent onset, dry cough, prominent systemic features (headache, malaise, GI symptoms), minimal auscultatory findings relative to CXR changes.
Examination: Dullness to percussion, decreased breath sounds, bronchial breathing, crepitations, egophony over consolidation.
In the elderly: Atypical presentation is common - confusion, functional decline, minimal respiratory symptoms. Fever may be absent in ~60% of nursing home patients with pneumonia.
Diagnosis
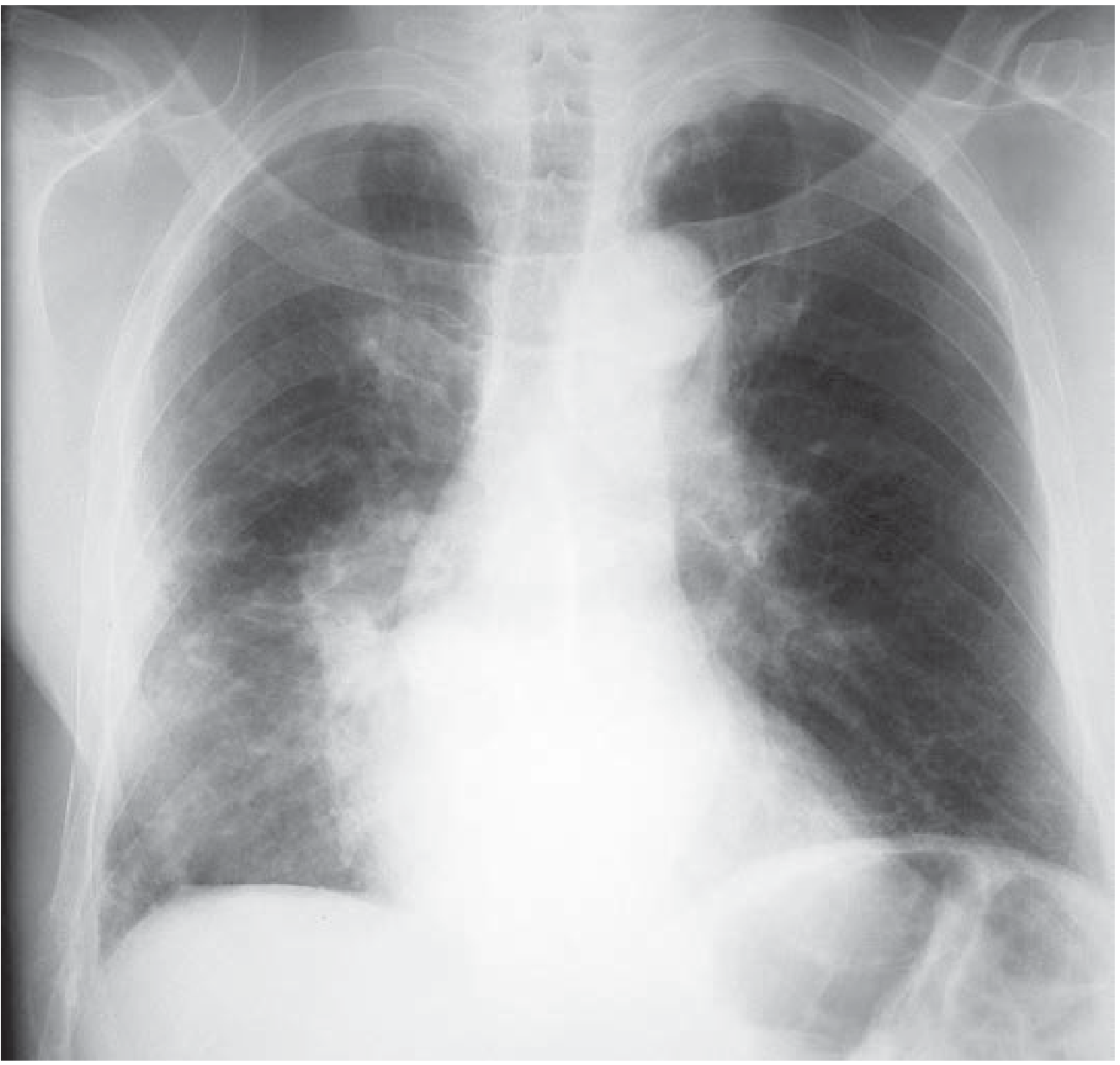
Chest Radiograph
- Required to confirm the diagnosis
- Findings range from lobar consolidation to patchy interstitial infiltrates
- Can lag behind clinical presentation; may be falsely negative early in dehydrated patients
- CXR alone cannot reliably identify the causative organism
Laboratory Workup
Outpatients (low severity): CXR + pulse oximetry + PCR for SARS-CoV-2 and influenza (in season) are generally sufficient. Sputum cultures are low-yield and not routinely recommended.
Hospitalized patients: CBC (leukocytosis with neutrophilia in bacterial; leukopenia in viral or overwhelming sepsis), BMP (renal function, glucose), blood cultures x2 before antibiotics, ABG if tachypneic, procalcitonin (elevated in bacterial infection), CRP.
Severe CAP or ICU patients: Add urinary Legionella antigen + urinary pneumococcal antigen. Consider bronchoscopy/BAL if diagnosis is uncertain or patient is not responding.
- Goldman-Cecil Medicine, p. 993
Severity Assessment
Two validated scoring tools guide the site-of-care decision:
CURB-65 Score
| Variable | Points |
|---|---|
| Confusion (new onset) | 1 |
| Urea >7 mmol/L (BUN >20 mg/dL) | 1 |
| Respiratory rate ≥30/min | 1 |
| Blood pressure: systolic ≤90 or diastolic ≤60 mmHg | 1 |
| Age ≥65 years | 1 |
- Score 0: Outpatient (30-day mortality ~1.5%)
- Score 1-2: Consider hospital admission (modify if age alone drives the score)
- Score ≥3: Hospitalize; consider ICU (30-day mortality ~22%)
PSI (Pneumonia Severity Index)
- Uses 20 variables (age, sex, comorbidities, physical exam, labs)
- Assigns patients to Risk Classes I-V with mortality ranging from 0.1% (Class I) to 29.2% (Class V)
- Classes I-II: outpatient; Class III: observation; Classes IV-V: admit
The PSI has greater efficacy and has been more robustly validated than CURB-65 but is harder to calculate without a calculator. - Harrison's Principles of Internal Medicine 22E (2025), p. 1069
ICU Admission Criteria (ATS/IDSA Minor Criteria)
Admit to ICU if 1 major criterion OR ≥3 minor criteria:
- Major: Septic shock requiring vasopressors; invasive mechanical ventilation
- Minor: RR ≥30/min; PaO2/FiO2 ≤250; multilobar infiltrates; confusion; BUN ≥20 mg/dL; WBC <4,000; platelets <100,000; temperature <36°C; hypotension requiring IV fluids
Treatment
Outpatient Treatment
| Patient Category | Preferred Regimen |
|---|---|
| No comorbidities, no resistance risk | Amoxicillin 1g TID alone, OR doxycycline 100mg BID, OR macrolide (if local resistance <25%) |
| With comorbidities (COPD, heart disease, DM, malignancy, alcoholism) | Amoxicillin-clavulanate or cephalosporin + macrolide or doxycycline; OR monotherapy with respiratory fluoroquinolone (levofloxacin 750mg/d, moxifloxacin 400mg/d) |
- Harrison's Principles of Internal Medicine 22E (2025), p. 1070-1071
Note: Newer guidelines (post-2019 ATS/IDSA update) permit beta-lactam monotherapy for low-risk outpatient CAP - a departure from prior guidelines requiring atypical coverage in all patients. - Fishman's Pulmonary Diseases, p. 2202
Inpatient (Non-ICU) Treatment
| Risk Status | Regimen |
|---|---|
| No MRSA/Pseudomonas risk | Beta-lactam (ceftriaxone 1-2g/d, ampicillin-sulbactam, cefotaxime, or ertapenem) + macrolide (azithromycin 500mg/d) OR respiratory fluoroquinolone monotherapy |
| Prior respiratory isolation of MRSA | Add vancomycin 15mg/kg q12h or linezolid 600mg q12h |
| Prior respiratory isolation of P. aeruginosa | Antipseudomonal beta-lactam + FQ or aminoglycoside |
ICU / Severe CAP Treatment
| Risk Status | Regimen |
|---|---|
| No Pseudomonas risk | Beta-lactam + macrolide OR beta-lactam + respiratory FQ |
| Pseudomonas risk | Piperacillin-tazobactam (or antipseudomonal carbapenem or cefepime) + ciprofloxacin 400mg IV; add aminoglycoside if FQ not used |
| MRSA risk | Add vancomycin or linezolid to above |
- Harrison's 22E (2025), p. 1071; Tintinalli's, p. 487
Antibiotic duration: Typically 5 days for low-severity CAP; 7-10 days for moderate-severe. De-escalate based on clinical response and culture results.
Complications
| Complication | Notes |
|---|---|
| Parapneumonic effusion / Empyema | Most common pulmonary complication; ~3-5% of hospitalized cases; requires drainage if exudative/complicated |
| Lung abscess | Cavitation, particularly with K. pneumoniae, S. aureus, anaerobes |
| Acute cardiac events | AF, new/worsening heart failure, myocardial ischemia in ~20-25% of hospitalized patients - Goldman-Cecil |
| Sepsis / Septic shock | Systemic progression requiring ICU level care |
| Respiratory failure | May require mechanical ventilation |
| Post-pneumonia cardiovascular risk | Increased risk of MI, stroke, and thromboembolism in months after pneumonia (see recent systematic review, PMID 41511415) |
Mortality: For hospitalized CAP: ~6% in-hospital, ~15% at 30 days. - Goldman-Cecil Medicine, p. 992
Special Populations
HIV/Immunocompromised
- S. pneumoniae remains the most common cause (bacteremia in 60% vs 15-30% in immunocompetent)
- P. aeruginosa is disproportionately common
- CD4 <200: suspect PCP (Pneumocystis jirovecii)
- CD4 250-500: TB, Cryptococcus, Histoplasma
- CD4 >800: typical bacterial CAP pattern
Elderly / Nursing Home Patients
- Atypical presentations common (confusion, functional decline, minimal fever)
- Organisms: S. pneumoniae, gram-negative bacilli, H. influenzae
- Influenza vaccine only 33-55% effective in preventing post-influenza pneumonia in nursing home residents
- MRSA coverage warranted for healthcare-associated organisms
Prevention
- Pneumococcal vaccines: PCV15 or PCV20 (preferred over PPSV23 alone per current guidelines) for adults ≥65 and high-risk groups
- Influenza vaccine: Annual; reduces post-influenza bacterial pneumonia
- COVID-19 vaccine: Reduces SARS-CoV-2 pneumonia
- Smoking cessation: Strong independent risk reduction
- Oral hygiene: Reduces aspiration pneumonia risk
Recent Evidence (2024-2026)
- A 2025 meta-analysis (PMID 40107661) identified key risk factors for drug-resistant pathogens in CAP, reinforcing the importance of targeted MDR risk stratification before antibiotic selection.
- A 2025 systematic review (PMID 41511415) confirmed significantly elevated cardiovascular and thromboembolic event risk in adults following CAP - an often underappreciated post-discharge risk.
- A 2025 meta-analysis (PMID 41062168) analyzed outcome variability drivers in CAP, highlighting age, multilobar disease, and bacteremia as key mortality predictors.
Sources: Goldman-Cecil Medicine (International Ed.); Harrison's Principles of Internal Medicine 22E (2025, McGraw Hill); Tintinalli's Emergency Medicine; Fishman's Pulmonary Diseases and Disorders; PubMed PMID 40107661, 41511415, 41062168
This is a shared conversation. Sign in to Orris to start your own chat.