analyse_media
Reading File
Finding Sources
Searching the Web
neurofibromatosis type 1 optic pathway glioma diagnostic criteria management
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
I now have sufficient information to provide a comprehensive answer. Let me compile it.
Diagnosis: Neurofibromatosis Type 1 (NF1) - von Recklinghausen Disease
This is a classic presentation of NF1 in a 17-year-old girl. Here is a complete breakdown:
What the Slide Shows
MRI (axial T2-weighted brain images):
- A large, lobulated hyperintense mass involving the optic chiasm, suprasellar region, and hypothalamus
- This is an optic pathway glioma (OPG) - the most characteristic CNS tumor in NF1
- The mass causes significant mass effect, explaining her headache and blurred vision in the left eye (increased intracranial pressure + direct optic pathway compression)
Skin findings (photos by James M. Coombs, MD, U of Iowa, 2005):
- Axillary freckling (Crowe sign): Clustered small hyperpigmented macules in both axillae (top-right images)
- Café-au-lait macules (CALMs): Multiple flat, light-brown oval patches on the trunk/back (bottom image)
Diagnostic Criteria for NF1 (Revised 2021)
A diagnosis requires 2 or more of the following in an individual without a family history of NF1:
| Criterion | Details |
|---|---|
| Café-au-lait macules | ≥6 macules; ≥5 mm prepubertal, ≥15 mm postpubertal |
| Neurofibromas | ≥2 neurofibromas of any type, OR ≥1 plexiform neurofibroma |
| Axillary/inguinal freckling | (Crowe sign) |
| Optic pathway glioma | |
| Lisch nodules | ≥2 iris hamartomas (slit-lamp exam) |
| Distinctive bony lesion | Sphenoid dysplasia, tibial pseudarthrosis |
| Pathogenic NF1 variant | In blood or tissue at VAF ≥50% |
| First-degree relative with NF1 | Only 1 criterion needed if parent has NF1 |
This patient already has 3 criteria (CALMs + axillary freckling + optic pathway glioma), making the diagnosis certain.
Key Disease Facts
Genetics:
- Autosomal dominant; chromosome 17q11.2 (NF1 gene)
- Encodes neurofibromin, a 327 kDa tumor suppressor that negatively regulates RAS signaling
- Incidence: ~1 in 2,000-3,000 births; up to 50% are new (de novo) mutations
- Penetrance approaches 100% in adults but expressivity is highly variable
Neurofibromin function: Acts as a GTPase-activating protein (GAP) - loss leads to constitutive RAS/MAPK pathway activation, driving tumor formation (Dermatology 2-Volume Set 5e, p. 1186)
Optic Pathway Gliomas in NF1
- Occur in 15-20% of NF1 children (Bradley & Daroff's Neurology, p. 1578)
- NF1 accounts for ~50% of all treated OPG cases
- Histology: mostly pilocytic astrocytoma (WHO grade I)
- NF1-associated OPGs tend to have a more indolent course than sporadic OPGs
- ~20% of NF1 children imaged prospectively will show MRI abnormalities, but less than half develop progressive disease; occasional spontaneous regression occurs
Clinical features of OPG (as in this case):
- Unilateral/bilateral vision loss + blurring
- Proptosis (if optic nerve involved)
- Obstructive hydrocephalus -> headache (from hypothalamic/chiasmatic involvement)
- Diencephalic syndrome in infants (failure to thrive, nystagmus, irritability)
Management of OPG in NF1
The goal is vision preservation, not tumor elimination.
- Surveillance MRI - regular monitoring; many tumors are stable or regress spontaneously
- Chemotherapy (first-line for progressive disease):
- Carboplatin/vincristine (primary first-line)
- Vinblastine monotherapy
- Bevacizumab - shown to improve vision in patients with progressive visual loss
- Targeted therapy (emerging):
- MEK inhibitors (selumetinib) and BRAF inhibitors - impressive responses in early trials; selumetinib is now approved for NF1-related plexiform neurofibromas
- Note: BRAF fusions are more common in non-NF1 OPGs
- Radiation therapy - relatively contraindicated in NF1 due to very high risk of secondary high-grade gliomas and vasculopathies (moyamoya syndrome) (Bradley & Daroff's, p. 1578)
- Surgery - limited role; biopsy for uncertain cases; partial resection only for symptomatic relief
Other NF1 Complications to Screen for
| System | Complication |
|---|---|
| CNS | T2 hyperintensities on MRI (50-75%), learning difficulties (30-50%), seizures (~5%), aqueductal stenosis |
| Musculoskeletal | Osteopenia, short stature, scoliosis, sphenoid wing dysplasia, pseudarthrosis of tibia |
| Tumors | Malignant peripheral nerve sheath tumors (3-15%), pheochromocytoma (~1%), JMML, GIST |
| Cardiovascular | Hypertension (~30%), renal artery stenosis, pulmonic stenosis |
| Eyes | Lisch nodules (iris hamartomas); optic atrophy if OPG untreated |
| Skin | Plexiform neurofibromas ("bag of worms"), cutaneous neurofibromas |
Summary
This 17-year-old girl's triad of café-au-lait macules + axillary freckling (Crowe sign) + optic pathway glioma is diagnostic of NF1. The OPG compresses the optic chiasm and hypothalamus, causing her headache and visual blurring. Management requires a multidisciplinary team: ophthalmology for serial visual acuity, neuro-oncology for chemotherapy decisions, and a dedicated NF clinic for long-term surveillance.
Sources: Dermatology 2-Volume Set 5e, p. 1186; Bradley and Daroff's Neurology in Clinical Practice, p. 1578; Goldman-Cecil Medicine, p. 266; NF1 OPG multidisciplinary management - Frontiers in Surgery
analyse_media
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
mesial temporal sclerosis MRI findings young adult uncontrolled seizures temporal lobe epilepsy
Reading File
Reading File
Reading File
Reading File
Finding Sources
Loading Image
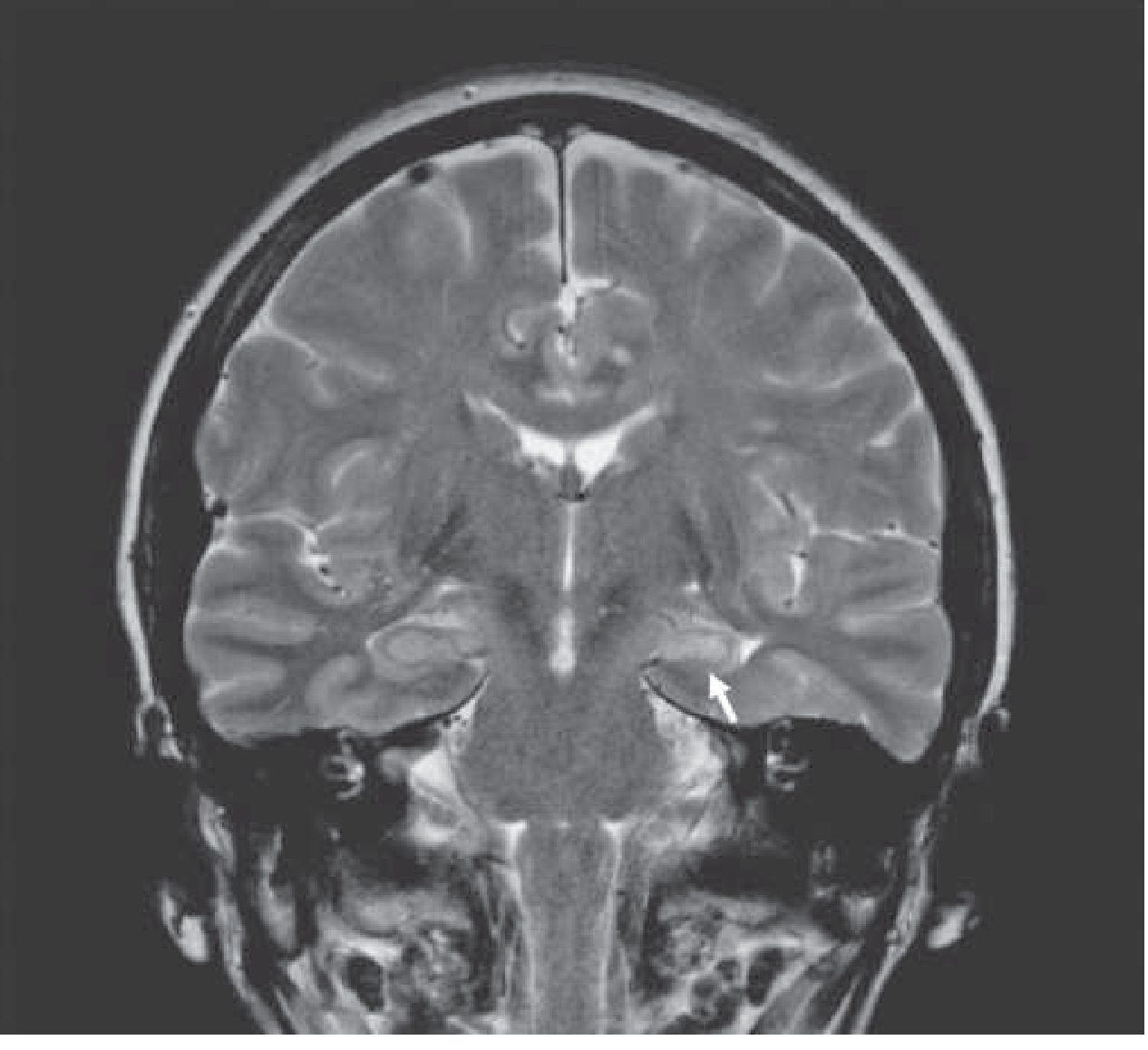
I now have all the information needed. The textbook image above is a perfect comparator - it shows mesial temporal sclerosis on coronal T2 with a small, hyperintense left hippocampus (arrow), which is exactly the pattern seen in this case. Let me compile the full answer.
Diagnosis: Mesial Temporal Sclerosis (MTS) / Hippocampal Sclerosis
Most likely diagnosis: Mesial Temporal Lobe Epilepsy (MTLE) due to Mesial Temporal Sclerosis (MTS) - the single most common cause of drug-resistant epilepsy in young adults.
MRI Analysis - Four Sequences
| Panel | Sequence | Key Finding |
|---|---|---|
| 1st (Coronal T1) | Coronal T1-weighted | Asymmetric hippocampal volume - one hippocampus appears smaller than the other |
| 2nd (Coronal T2) | Coronal T2-weighted | Increased T2 signal (hyperintensity) in the smaller hippocampus + loss of normal internal architecture - this is the hallmark finding |
| 3rd (Axial T2) | Axial T2-weighted | Confirms mesial temporal hyperintensity; ipsilateral temporal horn enlargement visible |
| 4th (Post-contrast) | Axial T1 post-gadolinium | No significant enhancement (expected in MTS - gliosis does not enhance) |
The textbook reference image below shows the identical pattern - small, hyperintense left hippocampus (white arrow) on coronal T2 at the level of the hippocampal bodies:
Classic MRI Triad of Hippocampal Sclerosis
All three features should be sought on dedicated epilepsy-protocol MRI:
- Hippocampal volume loss (atrophy/small hippocampus) - most sensitive sign
- Increased T2/FLAIR signal within the abnormally small hippocampus - due to gliosis replacing lost neurons
- Loss of internal trilaminar architecture of the hippocampus
Secondary MRI findings:
- Dilatation of the ipsilateral temporal horn (due to hippocampal atrophy)
- Atrophy of the ipsilateral mamillary body and fornix
- Small ipsilateral temporal lobe overall
MRI identifies up to 90% of hippocampal sclerosis cases (Grainger & Allison's Diagnostic Radiology)
Mesial Temporal Lobe Epilepsy Syndrome
Harrison's 22e provides the full syndrome characteristics:
| Feature | Details |
|---|---|
| History | Often history of febrile seizures in early childhood; family history of epilepsy; seizures often intractable to medications |
| Seizure semiology | Aura (epigastric rising sensation, déjà vu, fear), behavioral arrest/stare, complex automatisms (lip-smacking, chewing, fumbling), postictal disorientation and memory loss, dysphasia (dominant hemisphere) |
| EEG | Unilateral or bilateral anterior temporal spikes |
| PET | Interictal hypometabolism in temporal lobe |
| SPECT | Hyperperfusion during ictal phase |
| Wada test | Material-specific memory deficits |
Pathology
The histologic substrate is neuronal loss and gliosis in the hippocampus and amygdala - specifically:
- Loss of neurons in the CA1 (Sommer sector) of the pyramidal cell layer - most vulnerable zone
- Often extends into CA3, CA4 and the dentate gyrus
- Granule cell layer dispersion in the dentate
- Ipsilateral fornix and mamillary body atrophy (secondary to lost hippocampal output)
The chicken-or-egg question remains unresolved: does hippocampal sclerosis cause the seizures, or do recurrent seizures cause progressive hippocampal damage? Surgical outcomes favor the former in most cases. (Adams & Victor's Principles of Neurology, 12e)
Note: Bilateral MTS occurs in up to 20% of cases. "Dual pathology" (MTS + cortical dysplasia) must be excluded before surgery.
Differential Diagnosis in a 23-Year-Old with Uncontrolled Seizures
| Diagnosis | How to distinguish |
|---|---|
| Mesial temporal sclerosis | Most likely - small hyperintense hippocampus, no mass, no enhancement |
| Low-grade glioma (astrocytoma, DNET, ganglioglioma) | Cortical/subcortical mass; DNET is multicystic, T1 hypointense; ganglioglioma may calcify and enhance |
| Focal cortical dysplasia | Cortical thickening, blurred gray-white junction, may coexist with MTS |
| Autoimmune encephalitis (anti-NMDAR, LGI1, CASPR2) | Bilateral temporal T2 hyperintensity, rapidly progressive, CSF pleocytosis, positive antibodies |
| Rasmussen encephalitis | Progressive unilateral hemispheric atrophy |
| Cavernous malformation | Hemosiderin ring on T2*, "popcorn" appearance |
Management
Step 1 - AED optimization:
- Carbamazepine/oxcarbazepine are first-line for focal (temporal lobe) epilepsy
- This patient has uncontrolled seizures → likely drug-resistant (failure of ≥2 appropriate AEDs)
Step 2 - Pre-surgical evaluation (for drug-resistant cases):
- High-resolution epilepsy-protocol MRI (3T, coronal FLAIR/T2)
- Video-EEG monitoring to confirm seizure lateralization
- Neuropsychological testing (memory, language)
- FDG-PET (interictal hypometabolism)
- Ictal SPECT (if needed)
- Wada test or fMRI for language/memory lateralization
Step 3 - Surgery:
- Anterior temporal lobectomy (ATL) or selective amygdalohippocampectomy
- Outcomes: >80% experience significant seizure reduction; >60% become entirely seizure-free (Kaplan & Sadock's Comprehensive Psychiatry)
- Surgery is curative in up to 70% of patients with unilateral hippocampal sclerosis without dual pathology (Grainger & Allison's)
- Only delay to surgical referral predicts relapse post-surgery
Step 4 - Newer options:
- Laser interstitial thermal therapy (LITT/stereotactic laser amygdalohippocampectomy) - minimally invasive alternative
- Responsive neurostimulation (RNS) for bilateral or inoperable cases
- Vagus nerve stimulation (VNS)
Bottom Line
This 23-year-old woman has drug-resistant mesial temporal lobe epilepsy secondary to unilateral hippocampal sclerosis. The MRI shows the classic triad of hippocampal atrophy + T2 hyperintensity + loss of internal architecture. With uncontrolled seizures, she is a surgical candidate and should be referred to a dedicated epilepsy surgery center for comprehensive pre-surgical evaluation. Surgery offers >60% chance of seizure freedom.
Sources: Harrison's Principles of Internal Medicine 22e, p. 3456; Adams & Victor's Principles of Neurology 12e, p. 1206; Grainger & Allison's Diagnostic Radiology, p. 1497; Radiopaedia - Mesial Temporal Sclerosis
analyse_media
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Searching the Web
low grade glioma IDH mutant diffuse astrocytoma MRI T2 hyperintense non-enhancing young adult seizure diagnosis management 2024
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
Reading File
Loading Image
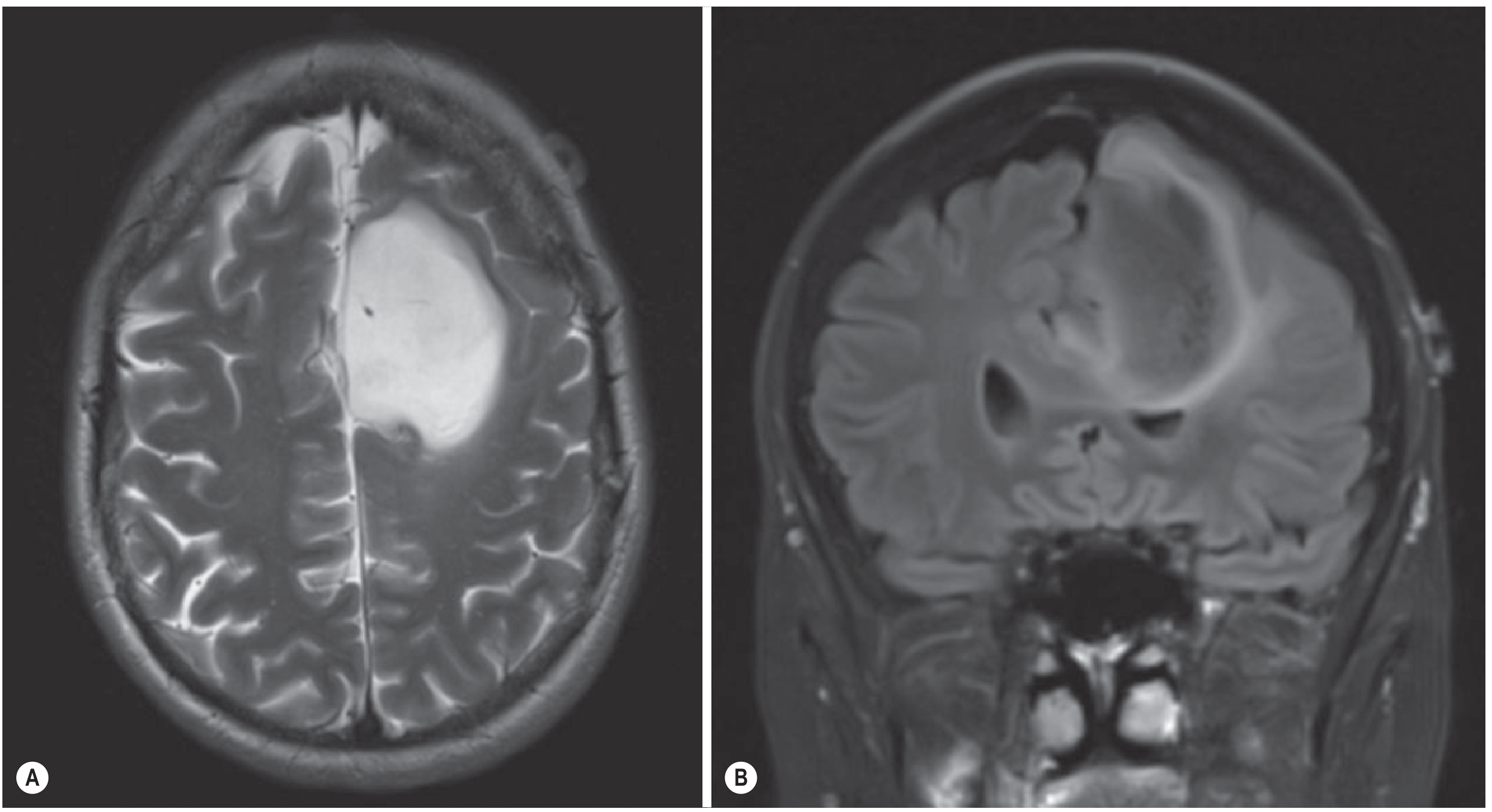
The textbook image above (Fig. 55.8 - FLAIR mismatch sign in IDH-mutant astrocytoma) is strikingly similar to the case. I now have everything needed for a comprehensive answer.
Diagnosis: Low-Grade Diffuse Glioma (WHO Grade 2) - Most Likely IDH-Mutant Astrocytoma
This is a classic imaging presentation of a low-grade diffuse glioma in a young adult. The MRI features are textbook.
MRI Analysis - Three Sequences
| Panel | Sequence | Finding |
|---|---|---|
| Left (Axial T1 ± contrast) | Axial T1-weighted | Large, well-demarcated, homogeneously hypointense (dark) mass in the left frontal/frontoparietal lobe, compressing the left lateral ventricle with mild rightward midline shift. No enhancement - intact blood-brain barrier |
| Middle (Axial T2) | Axial T2-weighted | Same mass is intensely and homogeneously hyperintense (bright), nearly CSF-signal. Minimal surrounding vasogenic edema despite large size - hallmark of slow-growing tumor |
| Right (Sagittal T1 ± contrast) | Sagittal T1 post-contrast | Confirms the large, well-circumscribed frontal mass with no significant internal or marginal enhancement. Mass effect on the overlying cortex is evident |
Key "classic triad" for low-grade glioma:
- T1 hypointense
- T2 hyperintense (homogeneous)
- Non-enhancing (intact blood-brain barrier - the most important distinguishing feature from high-grade glioma)
The textbook reference image below from Grainger & Allison's Diagnostic Radiology (Fig. 55.8) shows a virtually identical lesion - an IDH-mutant astrocytoma with the T2-FLAIR mismatch sign:
WHO 2021 Classification of Adult Diffuse Gliomas
The 2021 WHO CNS classification is molecularly integrated - histology alone is no longer sufficient:
| Tumor Type | Molecular Signature | Prognosis |
|---|---|---|
| Astrocytoma, IDH-mutant (grade 2-4) | IDH1/2 mutation + 1p19q intact + ATRX loss | ~6 years median (grade 2) |
| Oligodendroglioma, IDH-mutant (grade 2-3) | IDH mutation + 1p19q codeletion + TERT mutation | ~8 years median (grade 2) |
| Glioblastoma, IDH-wildtype (grade 4) | IDH wildtype + EGFR amplification or TERT mutation | 12-14 months |
For this patient (young, 26 years, frontal lobe, non-enhancing): IDH-mutant astrocytoma (grade 2) is the top diagnosis.
Molecular Pathogenesis
IDH mutations are the key early event in low-grade glioma genesis:
- IDH (isocitrate dehydrogenase) normally converts isocitrate → α-ketoglutarate
- Mutant IDH (most commonly IDH1 R132H, >90%) produces 2-hydroxyglutarate (2-HG) instead
- 2-HG is an oncometabolite that disrupts epigenetic regulation (DNA/histone hypermethylation) and impairs cellular differentiation
- 2-HG also mimics glutamate at NMDA receptors - this directly contributes to the high seizure burden seen in these patients
- Despite producing 2-HG, IDH-mutant gliomas have a significantly better prognosis than IDH-wildtype
FLAIR-mismatch sign - a highly specific imaging biomarker for IDH-mutant, 1p19q-intact astrocytoma:
- Markedly T2-hyperintense solid tumor with relatively suppressed FLAIR signal internally
- Present in ~50% of IDH-mutant astrocytomas; very high specificity when present
Why This Patient Has His Three Symptoms
| Symptom | Mechanism |
|---|---|
| Seizures | Cortical irritation from infiltrating tumor; 2-HG mimicking glutamate at NMDA receptors |
| Headache | Mass effect + raised intracranial pressure from the large lesion compressing the ventricle |
| Slowness of thought | Frontal lobe infiltration (executive function, processing speed) + subcortical white matter involvement |
Differential Diagnosis
| Diagnosis | How to distinguish |
|---|---|
| IDH-mutant astrocytoma (grade 2) ✓ Most likely | Non-enhancing, T2 bright, young adult, frontal lobe, no calcification |
| Oligodendroglioma (IDH-mutant, 1p19q-del) | Also non-enhancing; calcification on CT (up to 90%); more cortical; 1p19q deletion on molecular testing |
| IDH-wildtype astrocytoma (grade 3) | May appear identical on MRI but has malignant behavior; needs molecular testing |
| Glioblastoma (grade 4) | Ring-enhancing with central necrosis, surrounding edema; unusual at age 26 |
| DNET / Ganglioglioma | More cortical/"bubbly", often temporal, may have scalloping of overlying calvarium |
| Cerebral abscess | Ring-enhancing, restricted diffusion (DWI bright), clinical signs of infection |
Management
Step 1 - Tissue diagnosis is mandatory (biopsy or resection):
- Stereotactic biopsy if eloquent location
- Maximum safe resection if feasible - extends survival, reduces seizure burden, and provides adequate tissue for molecular profiling
Step 2 - Molecular profiling (required for WHO 2021 diagnosis):
- IDH1/2 mutation testing (immunohistochemistry ± sequencing)
- 1p/19q codeletion (FISH)
- ATRX expression
- MGMT promoter methylation
- TERT promoter mutation
Step 3 - Adjuvant therapy (for grade 2, after resection):
- Radiotherapy + temozolomide chemotherapy (standard for high-risk grade 2: age >40, incomplete resection, or large tumor)
- For low-risk grade 2: active surveillance or chemotherapy alone to defer radiation
Step 4 - Targeted therapy (2024 FDA approval - MAJOR UPDATE):
- Vorasidenib (dual IDH1/2 inhibitor) - FDA approved August 2024 for grade 2 IDH-mutant astrocytoma and oligodendroglioma after surgery
- The INDIGO Phase III trial showed vorasidenib prolonged progression-free survival from 11.1 → 27.7 months (HR 0.39)
- Brain-penetrant oral agent; delays need for chemoradiation and preserves cognitive function
- This represents a paradigm shift in management of grade 2 IDH-mutant gliomas
Step 5 - Seizure management:
- Anti-seizure medications (levetiracetam preferred; avoid enzyme inducers)
- Tumor resection itself often reduces seizure frequency
Prognosis
| Grade | Median Overall Survival |
|---|---|
| Grade 2 IDH-mutant astrocytoma | ~6 years (malignant transformation in 3-10 years) |
| Grade 2 oligodendroglioma | ~8 years |
| Grade 4 glioblastoma (IDH-wildtype) | 12-14 months |
Sources: Grainger & Allison's Diagnostic Radiology, pp. 1407-1408; Bradley & Daroff's Neurology in Clinical Practice, p. 1552; Vorasidenib FDA approval - Frontiers in Oncology 2025; Gliomas in adults - guidance 2024This is the same case as the previous slide (same patient: 26-year-old man with seizure, headache, and slowness in thoughts) - just a clearer, higher-resolution version of the identical MRI images. The three sequences and findings are the same.
Here is a quick comparison confirming it is the same case:
| Feature | Previous image | This image |
|---|---|---|
| Clinical details | 26y man, seizure, headache, slowness in thoughts | Identical |
| Left panel | Axial T1 - large hypointense left frontoparietal mass | Identical |
| Middle panel | Axial T2 - same mass intensely hyperintense, near-CSF signal | Identical |
| Right panel | Sagittal T1 - large non-enhancing frontal mass | Identical |
The cleaner version confirms the key features even more clearly:
- Left panel (Axial FLAIR or T1): The large left frontal mass is uniformly hypointense/dark, occupying a substantial portion of the left hemisphere with mild rightward midline shift and compression of the left ventricle
- Middle panel (Axial T2): Intensely, homogeneously hyperintense - nearly matching CSF signal - with a small focus of even brighter signal possibly representing a small cystic component. Minimal surrounding edema
- Right panel (Sagittal T1 post-contrast): The mass appears relatively hypointense to isointense with no significant enhancement, confirming intact blood-brain barrier
The diagnosis remains: Low-Grade Diffuse Glioma, WHO Grade 2 - most likely IDH-mutant astrocytoma.
Please refer to my full analysis in the previous response for:
- Complete MRI characterization and the T2-FLAIR mismatch sign
- WHO 2021 molecular classification (IDH mutation, 1p/19q, ATRX)
- Pathogenesis (2-HG oncometabolite, NMDA receptor mechanism for seizures)
- Management including the 2024 FDA approval of vorasidenib
- Differential diagnosis and prognosis tableThis is the exact same image as the one you just sent moments ago - same case, same MRI, same patient (26-year-old man with seizure, headache, and slowness in thoughts).
The diagnosis and full analysis remain unchanged: Low-Grade Diffuse Glioma, WHO Grade 2 - IDH-mutant astrocytoma (most likely).
Is there a specific question you'd like me to address about this case? For example:
- Differentiating astrocytoma vs. oligodendroglioma - what additional imaging/tests help?
- Surgical planning - eloquent cortex mapping, extent of resection strategy
- The FLAIR-mismatch sign - how to apply it in this case
- Vorasidenib and IDH inhibitors - mechanism and the INDIGO trial in detail
- Seizure management in glioma patients
- Malignant transformation - when and how to monitor for upgrade to grade 3/4
Or if you meant to upload a different slide from your lecture series, please try again and I'll analyze it fresh.
analyse_media
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Reading File
Reading File
Reading File
I now have all the information needed. Here is the complete answer.
Diagnosis: Tuberous Sclerosis Complex (TSC) with Subependymal Giant Cell Astrocytoma (SEGA)
The classic teaching point of this case: what looks like "severe acne" is actually facial angiofibromas - the cardinal dermatological sign of TSC.
What the Slide Shows
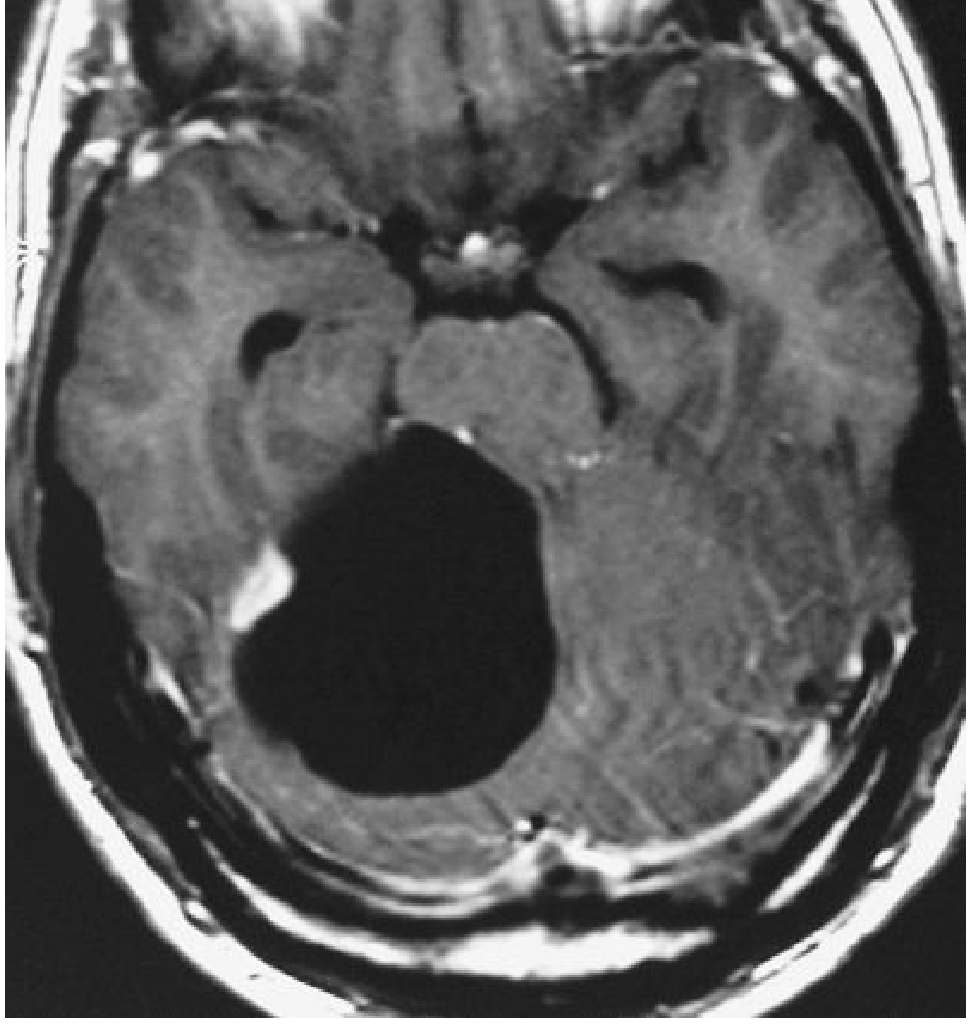
MRI (axial post-contrast T1):
- A well-circumscribed, intensely and homogeneously enhancing mass at the foramen of Monro (right side), projecting into the lateral ventricle
- Obstructive hydrocephalus with dilatation of the lateral ventricles bilaterally
- This is pathognomonic for a Subependymal Giant Cell Astrocytoma (SEGA) in the context of TSC
Clinical photo (right):
- Multiple reddish-brown papules and nodules distributed symmetrically over the nose, cheeks, and nasolabial folds - a butterfly/malar distribution
- Grossly resembles severe acne, but the symmetry, location, and texture are characteristic of facial angiofibromas (historically called "adenoma sebaceum")
- Present in 75-90% of TSC patients older than 4 years
The textbook photo below (Andrews' Diseases of the Skin) shows the same lesions:

Tuberous Sclerosis Complex (TSC) - Overview
Genetics:
- Autosomal dominant; up to 50-86% are spontaneous (de novo) mutations
- Two genes: TSC1 (chromosome 9q34.3, encodes hamartin) and TSC2 (chromosome 16p13.3, encodes tuberin)
- TSC1 and TSC2 proteins form a complex that inhibits mTOR signaling (via suppression of RHEB GTPase)
- Loss of function → constitutive mTOR activation → uncontrolled hamartoma growth throughout the body
- TSC2 mutations = more severe disease (more SEGA, angiomyolipomas, intellectual disability)
Diagnostic Criteria (2012 International Consensus)
Definite diagnosis: 2 major features OR 1 major + ≥2 minor features
Major Features
| # | Feature |
|---|---|
| 1 | Hypomelanotic macules (≥3, ≥5 mm) - ash-leaf spots |
| 2 | Facial angiofibromas (≥3) or fibrous cephalic plaque |
| 3 | Ungual fibromas (Koenen tumors) |
| 4 | Shagreen patch (collagenoma on lower back) |
| 5 | Multiple retinal hamartomas |
| 6 | Cortical dysplasias (tubers + radial migration lines) |
| 7 | Subependymal nodules ("candle drippings") |
| 8 | Subependymal giant-cell astrocytoma (SEGA) |
| 9 | Cardiac rhabdomyoma |
| 10 | Lymphangioleiomyomatosis (LAM) |
| 11 | Angiomyolipomas (≥2) |
This patient already has 2 major features (facial angiofibromas + SEGA) = definite diagnosis.
Minor Features
Confetti skin lesions, dental enamel pits (≥3), intraoral fibromas, retinal achromic patch, multiple renal cysts, nonrenal hamartomas.
Neurological Features
| Feature | Details |
|---|---|
| Cortical tubers | Potato-like hamartomas; disorganized cortical lamination, balloon/giant cells, calcification; extend from ventricular wall to cortex |
| Subependymal nodules (SENs) | "Candle drippings" in ventricular walls; calcify in adolescence; asymptomatic unless they transform |
| SEGA | Arise from SENs near foramen of Monro; grow and enhance; cause obstructive hydrocephalus → headache (as in this patient) |
| Seizures | 80-90% of patients; most common cause of infantile spasms; often medically refractory |
| Intellectual disability | 40-60%; correlates with cortical tuber burden and early-onset epilepsy |
SENs → SEGA transformation: SENs enlarge over time, usually only through adolescence, then calcify. When they enlarge >1 cm, enhance on MRI, and are located near the foramen of Monro → SEGA.
Systemic Manifestations
| Organ | Lesion |
|---|---|
| Skin | Ash-leaf spots, facial angiofibromas, shagreen patch, ungual fibromas |
| Brain | Tubers, SENs, SEGA |
| Kidney | Angiomyolipomas (bilateral, multiple), renal cysts, renal cell carcinoma risk |
| Heart | Rhabdomyomas (highly specific; often regress after birth) |
| Lung | Lymphangioleiomyomatosis (LAM) - mainly women, progressive respiratory failure |
| Eye | Retinal hamartomas (phakomas), pigmentary changes |
| Bone | Cysts, sclerotic lesions |
| Teeth | ≥5 dental enamel pits (minor criterion) |
Management
1. SEGA causing obstructive hydrocephalus (as in this case):
- Surgical resection - standard treatment when symptomatic; can be curative for the obstructive hydrocephalus
- Everolimus (mTOR inhibitor) - FDA approved; shrinks SEGA in >50% of patients; useful to avoid/delay surgery or for recurrent/unresectable SEGA; also reduces angiomyolipoma size
- Regular MRI surveillance (every 1-3 years) for growing SENs to catch SEGA early
2. Seizures:
- Anti-seizure medications (vigabatrin preferred for infantile spasms in TSC - more effective than ACTH)
- Everolimus also has anti-seizure effects (mTOR pathway involved in epileptogenesis)
- Resective epilepsy surgery if seizures localize to 1-2 tubers
- Corpus callosotomy for severe cases
3. Renal angiomyolipomas:
- Embolization or nephron-sparing surgery for lesions >4 cm (risk of hemorrhage)
- Everolimus shrinks angiomyolipomas
4. Skin (facial angiofibromas):
- Topical rapamycin (sirolimus) gel - effective in reducing angiofibromas
- Laser ablation for cosmesis
Why This Was Misdiagnosed as "Severe Acne"
The key distinguishing features between angiofibromas and acne:
| Feature | Facial Angiofibromas | Acne Vulgaris |
|---|---|---|
| Distribution | Symmetric butterfly/malar pattern, nasolabial folds, nose | Variable; may involve back, chest |
| Lesion type | Firm, waxy, non-inflamed papules; NO comedones | Comedones, pustules, nodules |
| Evolution | Appear in preschool years, slowly increase, never resolve | Peaking in adolescence |
| Response to topical acne treatment | None | Variable |
| Associated features | Ash-leaf spots, seizures, family history | None |
The teaching point: In any teenager with "treatment-resistant acne" in a malar butterfly distribution - examine for ash-leaf spots under Wood's lamp, check for periungual fibromas, and ask about seizures.
Sources: Bradley & Daroff's Neurology in Clinical Practice, pp. 2199-2201; Andrews' Diseases of the Skin, p. 643; Harrison's Principles of Internal Medicine 22e, p. 1785
analyse_media
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Reading File
Finding Sources
Reading File
Loading Image
Excellent - the textbook image above (cerebellar pilocytic astrocytoma) shows a large dark cyst with a small bright enhancing mural nodule - this is the same morphological pattern identified in the case. I now have sufficient information for a complete answer.
Diagnosis: Cystic Tumor with Enhancing Mural Nodule - Most Likely Pilocytic Astrocytoma (WHO Grade I) or Pleomorphic Xanthoastrocytoma (PXA)
MRI Analysis - Four Sequences
| Panel | Sequence | Findings |
|---|---|---|
| 1st (Coronal T1 post-contrast) | Coronal T1+Gd | Right parietal subcortical lesion - large cystic component (hypointense, fluid-dark) with an intensely enhancing eccentric mural nodule abutting the dural/meningeal surface |
| 2nd (Coronal FLAIR) | Coronal FLAIR | Cystic component suppresses completely (confirming simple fluid, not necrosis); mural nodule remains visible; minimal perilesional FLAIR signal |
| 3rd (Axial T2) | Axial T2 | Bright white cystic component (near-CSF signal); small bright focus = mural nodule; mild surrounding T2 hyperintensity (modest vasogenic edema) |
| 4th (Axial T1 post-contrast) | Axial T1+Gd | Confirms the "cyst with enhancing mural nodule" pattern in axial plane; cyst wall does not enhance (differentiates from ring-enhancing abscess/GBM) |
The textbook reference image from Grainger & Allison's (Fig. 55.10) below shows an identical morphology - cerebellar pilocytic astrocytoma with a large dark cyst and small bright enhancing mural nodule:
Key Diagnostic Feature: The "Cyst with Enhancing Mural Nodule" Pattern
This is one of the most recognizable patterns in neuroimaging. It narrows the differential to a short list:
| Tumor | Location | Age | Key distinguishing features |
|---|---|---|---|
| Pilocytic Astrocytoma (PA), WHO I | Cerebellum >> optic path >> hemispheres | Children/young adults | BRAF-KIAA1549 fusion; Rosenthal fibers; >90% 5-year survival after GTR |
| Pleomorphic Xanthoastrocytoma (PXA), WHO II | Temporal lobe cortex, superficial, abuts meninges | Young adults (seizures) | May mimic "dural tail"; cystic in >50%; BRAF V600E in ~65% |
| Ganglioglioma, WHO I-II | Temporal > parietal cortex, superficial | Young adults (seizures) | Contains neurons + glia; calcification common; cystic variants |
| Hemangioblastoma | Cerebellum > supratentorial | Adults; VHL association | Highly vascular nodule; associated with VHL, polycythemia |
| DNET | Cortex, temporal | Young adults, seizures | Multicystic "bubbly"; no enhancement typically; calvarial remodeling |
For this patient (26-year-old female, right parietal, superficial/meningeal abutting, cyst + enhancing nodule, blackouts + headache):
- Primary diagnosis: Pilocytic Astrocytoma (PA) or PXA - both WHO low-grade, both present in young adults with seizures and headache, both show cyst+mural nodule
- PXA is favored if the lesion truly abuts the meninges (dural tail sign) - it has a predilection for the temporal lobe but can occur in the parietal lobe
- PA is favored if the mural nodule is the only enhancing component with complete non-enhancement of the cyst wall
Pilocytic Astrocytoma - Key Facts
Histology:
- Bipolar cells with long "pilocytic" processes
- Rosenthal fibers (corkscrew eosinophilic inclusions) - pathognomonic
- Eosinophilic granular bodies
- Microcysts
Molecular biology:
- BRAF-KIAA1549 fusion (most common, ~70%) → constitutive MAPK/ERK activation
- BRAF V600E mutation (~10%) - more common in cerebral/non-cerebellar location; worse prognosis
- IDH mutation: absent (unlike adult diffuse gliomas)
MRI signature:
- Large cyst + small enhancing mural nodule (especially cerebellar)
- Solid homogeneously enhancing mass (supratentorial)
- Minimal surrounding edema despite large size
- Non-infiltrating, well-circumscribed margins
Pleomorphic Xanthoastrocytoma (PXA) - Why it Fits
PXA particularly fits this case because:
- Young adult with seizures (blackouts) - PXA is strongly associated with cortical epilepsy
- Superficial cortical location abutting the meninges - PXA "hugs" the brain surface
- Cystic + solid enhancing component - in >50% of PXA
- Parietal lobe - less common than temporal but well-documented
- T1 hypointense, T2 hyperintense solid component
- May show a "dural tail sign" mimicking meningioma
PXA molecular: BRAF V600E in ~65% - targetable with vemurafenib/dabrafenib
Management
1. Surgery:
- Gross total resection (GTR) is the treatment of choice for both PA and PXA
- For PA: GTR is essentially curative - 5-year recurrence-free survival >90% after complete resection
- For PXA: GTR + resection of adjacent cortex (seizure focus); recurrence rate ~20% WHO II, higher for anaplastic (WHO III)
- Functional mapping needed given right parietal location (sensorimotor, visuospatial functions)
2. Post-operative:
- For PA: observation only after GTR; chemotherapy (carboplatin/vincristine) for incompletely resected/progressive tumors
- For PXA: adjuvant radiotherapy if anaplastic features; BRAF V600E+ tumors respond to dabrafenib ± trametinib (BRAF/MEK inhibition)
3. Seizure management:
- Pre-operatively: anti-seizure medications (levetiracetam)
- Surgical resection of the tumor + epileptogenic cortex often achieves seizure freedom
4. Biopsy/molecular testing is mandatory for definitive diagnosis and treatment planning
Differential to Exclude
| Diagnosis | Why unlikely here |
|---|---|
| Glioblastoma | Age 26 is unusual; GBM shows ring enhancement with necrotic core, NOT a simple thin-walled cyst; thick irregular wall |
| Brain abscess | Clinical signs of infection; diffusion restriction (DWI bright/ADC dark) in center; no mural nodule |
| Metastasis | Usually multiple; known primary tumor; age 26 is uncommon; ring enhancement typical |
| Cavernous malformation | "Popcorn" hemosiderin on T2*; no cystic component; no enhancement |
| Arachnoid cyst | Purely CSF-signal, no mural nodule, no enhancement, does not suppress on FLAIR differently |
The next step: MRI with full protocol (DWI, SWI, perfusion, spectroscopy) + surgical resection with intraoperative molecular profiling.
Sources: Bradley & Daroff's Neurology in Clinical Practice, p. 1576-1577; Grainger & Allison's Diagnostic Radiology, pp. 1408-1409
analyse_media
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Finding Sources
Finding Sources
I now have comprehensive information to deliver a complete answer.
Diagnosis: Ganglioglioma (WHO Grade I) - Most Likely; DNET as Close Differential
This case is a classic: young patient, status epilepticus, temporal lobe lesion, cystic mass with calcification on CT and an enhancing nodule on MRI.
What the Imaging Shows
CT (top-right panel):
- Axial non-contrast CT shows a right temporal lobe lesion with dense, clumped calcification - this is the single most diagnostic CT feature
- Calcification is "gritty" and coarse - classic for ganglioglioma ("solid portions are firm, gray, and gritty due to calcium deposits")
- The surrounding low-density region represents the cystic component
MRI - Three axial + one coronal (bottom row):
| Panel | Sequence | Finding |
|---|---|---|
| 1st (Axial T1) | Axial T1 | Right temporal lesion - hypointense cystic component with a solid nodular component; well-circumscribed |
| 2nd (Axial T2) | Axial T2 | Large hyperintense cystic component (bright, near-CSF signal); solid nodule adjacent; minimal surrounding edema |
| 3rd (Axial T1+Gd) | Axial post-contrast | Focal nodular/patchy enhancement of the solid component; cyst wall does not enhance |
| 4th (Coronal T1+Gd) | Coronal post-contrast | Confirms right temporal lobe location; cyst + enhancing nodule; extends toward temporal cortex surface |
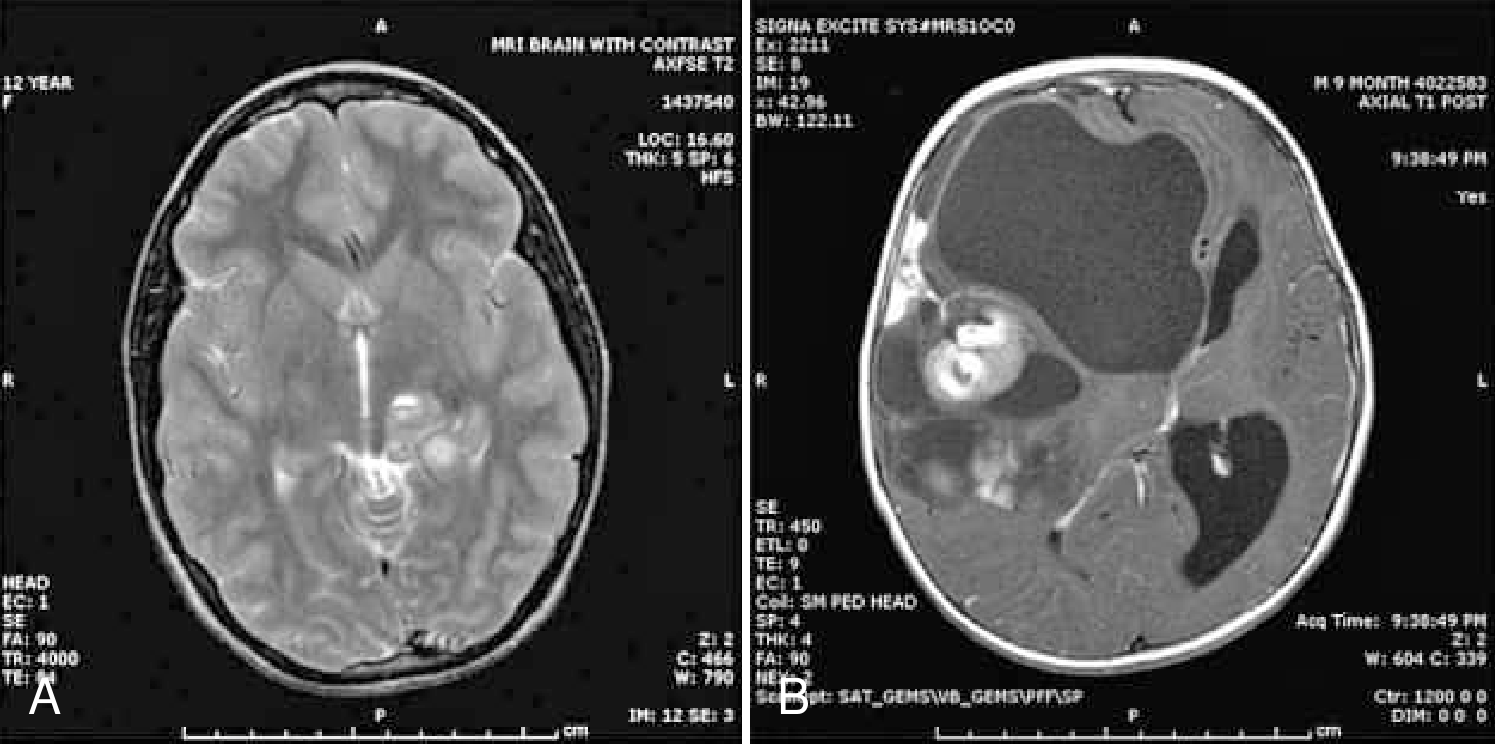
The textbook MRI (from Bradley & Daroff's Neurology) below shows a ganglioglioma in a 12-year-old - T2 prolongation in the medial temporal lobe (panel A) and a multicystic enhancing solid component (panel B), identical morphology:
Why Ganglioglioma Fits Perfectly
| Feature | This Case | Ganglioglioma |
|---|---|---|
| Age | 30 years | 80% occur < age 30 |
| Presentation | Status epilepticus | Seizures in ~50% at presentation; typical complex partial seizures |
| Location | Right temporal lobe | Most common location: medial temporal lobe |
| CT | Dense calcification | "Solid portions gritty due to calcium deposits" - CT calcification highly characteristic |
| MRI | Cystic + enhancing nodule | "Contrast-enhanced MRI reveals supratentorial cystic mass; T1 hypointense, T2 hyperintense; enhancement nodular to solid" |
| Surrounding edema | Minimal | Absent or minimal - reflects slow-growing benign tumor |
Ganglioglioma - Key Facts
What it is: A mixed tumor containing both neoplastic ganglion cells (neurons) AND glial elements (astrocytes) - hence "ganglio-glioma"
Epidemiology:
- 4-8% of all pediatric brain tumors; 80% occur in patients < age 30
- Most common site: temporal lobe >> other lobes >> cerebellum >> spinal cord
Histology:
- Dysmorphic ganglion cells (clustered, binucleate/multinucleate, lack polarity) - pathognomonic
- Eosinophilic granular bodies (EGBs)
- Perivascular lymphocytic cuffing
- Rosenthal fibers at tumor edges
- Microcystic spaces + collagen deposition
- Calcification in the solid component
Molecular biology:
- BRAF V600E mutation in 18-50% of cases - targetable
- Other MAPK pathway mutations: KRAS, NF1, FGFR1/2
- These mutations distinguish gangliogliomas from reactive/entrapped neurons in diffuse gliomas
WHO Grading:
- Grade I (vast majority) - typical ganglioglioma
- Grade III (rare) - anaplastic ganglioglioma; almost always in the glial component
Why Status Epilepticus?
Status epilepticus (SE) in this context is symptomatic (structural) SE - caused by the temporal lobe tumor acting as an epileptogenic focus:
- Temporal lobe gangliogliomas are intimately associated with refractory focal epilepsy
- SE may be the first presentation in a patient with a long-standing but previously undiagnosed slow-growing tumor
- The combination of cortical irritation from tumor + direct involvement of the hippocampal circuit drives the hyperexcitable focus
- BRAF V600E mutation → constitutive MAPK activation → abnormal neuronal excitability
Differential Diagnosis
| Diagnosis | Why consider | Why less likely here |
|---|---|---|
| Ganglioglioma ✓ | Temporal, calcified, cystic+nodule, young, seizures | - |
| DNET | Temporal cortex, young adult, seizures, cystic, intractable epilepsy | DNET: "bubbly"/multicystic, does NOT enhance (or minimal), cortical not deep, rarely calcifies, usually no nodule |
| PXA | Young adult, seizures, cystic+nodule, superficial, meningeal abutment | Less calcification; more solid; temporal but more surface-based |
| Pilocytic Astrocytoma | Cyst + nodule, young | PA rarely calcifies; less temporal preference; IDH-negative but BRAF fused |
| Low-grade glioma (IDH-mutant) | Young, temporal, seizures | Non-cystic, non-calcified, non-enhancing, diffuse T2 signal |
| Neurocysticercosis | Calcification, cysts, seizures, young | Multiple lesions typically; ring-enhancing; scolex visible; geographic/travel history |
| Oligodendroglioma | Calcification, seizures, young, temporal | Cortical ribbon-like calcification; non-enhancing or mild; 1p19q codeletion |
Management
1. Surgical resection (treatment of choice):
- Gross total resection (GTR) is curative in most cases
- Should include the tumor + epileptogenic cortex (if temporal: amygdalohippocampectomy may be needed)
- After GTR: 5-year survival ~89%; seizure freedom achieved in majority
- Incomplete resection → local recurrence risk (significant given propensity for recurrence despite low grade)
2. Pre-surgical workup:
- Video-EEG to confirm seizure focus localization
- fMRI/Wada test for language and memory lateralization (right temporal - dominant only if left-handed)
- Neuropsychological testing
- Molecular testing (BRAF V600E) on surgical specimen
3. Targeted therapy (if unresectable/recurrent with BRAF V600E):
- Dabrafenib ± trametinib (BRAF + MEK inhibition) - active in BRAF V600E+ CNS tumors
- Carboplatin/vincristine if BRAF wildtype
4. Status Epilepticus - immediate management (on presentation):
- Phase 1 (0-5 min): Lorazepam IV (0.1 mg/kg) or diazepam
- Phase 2 (5-20 min): Levetiracetam IV, valproate IV, or fosphenytoin IV
- Phase 3 (>20 min - refractory SE): Anesthesia - propofol, midazolam infusion, or pentobarbital
- Definitive treatment: Surgical removal of the epileptogenic tumor
5. Anti-seizure maintenance:
- Levetiracetam (preferred; no enzyme induction)
- Surgical resection often achieves complete seizure freedom
Summary
This 30-year-old presented with status epilepticus caused by a right temporal lobe ganglioglioma - a classic presentation. The calcification on CT is the most characteristic single feature. The management priority is two-fold: break the status epilepticus acutely, then refer to neurosurgery for definitive resection with concurrent epilepsy surgery evaluation.
Sources: Bradley & Daroff's Neurology in Clinical Practice, pp. 1582-1583; Grainger & Allison's Diagnostic Radiology, p. 1267; Goldman-Cecil Medicine (ganglioglioma section)
analyse_media
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Finding Sources
Finding Sources
Finding Sources
Searching the Web
cavernous malformation intraventricular lateral ventricle MRI popcorn hemosiderin obstructive hydrocephalus treatment
I now have comprehensive information for a complete answer.
Diagnosis: Intraventricular Cavernous Malformation (Cavernoma) with Obstructive Hydrocephalus
A 21-year-old woman with pre-existing epilepsy now presenting with worsening headache and blurred vision - this combination signals raised intracranial pressure from obstructive hydrocephalus caused by a growing intraventricular cavernous malformation.
Imaging Analysis - Five Panels
| Panel | Modality | Key Finding |
|---|---|---|
| a | Non-contrast CT | Large, hyperdense, lobulated intraventricular mass in the right lateral ventricle with heterogeneous density; internal calcification foci; extends toward/across midline; bilateral lateral ventricle dilatation = obstructive hydrocephalus |
| b | Contrast-enhanced CT | Heterogeneous, moderate-to-strong enhancement of the solid mass components; complex vascularized architecture confirmed |
| c | Axial T1 MRI | Mass is predominantly iso-to-hypointense with scattered T1-hyperintense foci (subacute blood/methemoglobin = bright on T1) - indicates blood products in multiple stages of evolution |
| d | Axial T2 MRI | Classic "popcorn" or "mulberry" appearance - heterogeneous mixed-signal core with multiple locules of varying signal (blood products at different ages) + a hypointense hemosiderin rim at the periphery - the most pathognomonic MRI sign |
| Coronal | Coronal T2 MRI | Confirms the intraventricular location; shows the extent of hydrocephalus; hemosiderin rim confirmed; bilateral temporal horn dilatation |
The "Popcorn Sign" - Why It Is Pathognomonic
The appearance arises because cavernous malformations consist of:
- Distended, back-to-back vascular channels (no intervening brain parenchyma) with collagenized walls
- Recurrent micro- and macrohemorrhages at different time points → blood products in all stages simultaneously:
| Blood product stage | T1 signal | T2 signal |
|---|---|---|
| Hyperacute (<24h) - oxyhemoglobin | Iso | Bright |
| Acute (1-3d) - deoxyhemoglobin | Dark | Dark |
| Early subacute (3-7d) - intracellular methemoglobin | Bright | Dark |
| Late subacute (>7d) - extracellular methemoglobin | Bright | Bright |
| Chronic - hemosiderin | Dark | Very dark (rim) |
The mixture of all these stages simultaneously creates the "popcorn" heterogeneity. The peripheral hemosiderin ring on T2 is from macrophage processing of chronic old blood - this is the hallmark.
SWI/T2 gradient echo* (not shown but would be ideal): hemosiderin causes "blooming artifact" - the lesion appears dramatically larger and darker than on conventional T2.
Cavernous Malformation - Key Facts
What it is: A low-flow vascular malformation consisting of clusters of dilated, thin-walled capillary channels (sinusoidal spaces) lined only by endothelium + subendothelial stroma; no smooth muscle or elastic fibers; no intervening brain parenchyma between channels.
Genetics:
- Sporadic (single lesion) in most cases
- Familial (autosomal dominant, multiple lesions) - mutations in:
- CCM1 (KRIT1, chromosome 7q)
- CCM2 (chromosome 7p)
- CCM3 (PDCD10, chromosome 3q)
- Rapidly growing lesions also require gain-of-function PIK3CA mutations (cancer-like second hit)
Epidemiology:
- Prevalence ~0.4-0.6% on MRI
- Accounts for 10-25% of all cerebral vascular malformations
- 80% supratentorial, 15% infratentorial, 5% intraspinal
- Intraventricular cavernomas: ~2.5-10% of all cavernomas; arise from choroid plexus or ventricular wall
Natural history:
- "Low-flow" lesions - do NOT participate in arteriovenous shunting
- Grow by recurrent microhemorrhages - each bleed expands the lesion and deposits hemosiderin
- Annual hemorrhage risk: ~0.25-0.7% per year (parenchymal); rebleed risk ~4.5%
Why This Patient Has Her Symptoms
| Symptom | Mechanism |
|---|---|
| Pre-existing epilepsy | Cortical irritation from repeated microhemorrhages depositing hemosiderin (iron) → seizure focus. Hemosiderin is directly epileptogenic |
| Worsening headache | Obstructive hydrocephalus - mass blocks foramen of Monro → raised ICP |
| Blurring of vision | Raised ICP → papilledema → visual blurring; if severe → Cushing's triad |
Differential Diagnosis for Intraventricular Mass with Hemorrhage
| Diagnosis | Key distinguishing feature |
|---|---|
| Cavernous malformation ✓ | "Popcorn" mixed T2 + hemosiderin rim + prior seizure history; no feeding/draining vessels |
| Central neurocytoma | Young adult, lateral ventricle attached to septum pellucidum; calcification; "bubbly" T2 but no hemosiderin; moderate enhancement; NeuN+ on histology |
| Subependymal giant cell astrocytoma (SEGA) | Near foramen of Monro; TSC stigmata (as in previous case); no hemosiderin |
| Choroid plexus papilloma/carcinoma | Cauliflower-like, intensely enhancing, produces CSF (communicating hydrocephalus); no hemosiderin |
| Ependymoma | Fourth ventricle > lateral ventricle; "plastic" growth through foramina; calcification; periventricular spread |
| AVM with hemorrhage | Nidus of tangled vessels; flow voids; arterial feeders and draining veins on MRA/DSA |
| Intraventricular meningioma | Trigone of lateral ventricle; middle-aged women; homogeneous intense enhancement; dural tail |
Management
Emergency (acute hydrocephalus):
- Urgent neurosurgical consultation
- External ventricular drain (EVD) if acutely decompensating (rapidly rising ICP → herniation risk)
- Osmotherapy (mannitol) as bridge
Definitive treatment - Surgery:
- Complete surgical resection is the gold standard for intraventricular cavernomas
- Approach options: transcallosal, transcortical (transventricular)
- Complete removal resolves hydrocephalus and removes the hemorrhage source
- Reported cure rates high after GTR
- The associated developmental venous anomaly (DVA) (found in 20-60% of cases alongside cavernomas) must be preserved - do NOT resect it (causes venous infarction)
When is observation appropriate?
- Small, asymptomatic, non-eloquent location, no recurrent hemorrhages → watchful waiting
- This patient's obstructive hydrocephalus makes surgery mandatory
Anti-seizure medication:
- Continue/optimize (levetiracetam preferred)
- Post-resection seizure freedom expected in most cases once the hemosiderin-laden epileptogenic focus is removed
Radiosurgery (Gamma Knife):
- Controversial; considered for deep eloquent/inaccessible lesions
- Does NOT acutely resolve hydrocephalus
Zabramski MRI Classification (for completeness)
| Type | T1 | T2 | Pathology |
|---|---|---|---|
| I | Hyperintense core | Mixed | Subacute hemorrhage |
| II | Mixed | Mixed "popcorn" + hypointense rim | Recurrent hemorrhage at various stages ← This case |
| III | Iso/hypointense | Hypointense | Chronic resolved hemorrhage |
| IV | Iso | Punctate hypointense (only on GRE/SWI) | Capillary telangiectasia-like microhemorrhage |
This is a Type II cavernous malformation - the most symptomatic and surgically important type.
Sources: Robbins, Cotran & Kumar Pathologic Basis of Disease, p. 3820; Localization in Clinical Neurology 8e; Radiopaedia - Cerebral Cavernous Venous Malformation; Intraventricular CM treatment - PMC
This is a shared conversation. Sign in to Orris to start your own chat.