Diverticular disease
Reading File
Finding Sources
Searching PubMed
"diverticular disease" OR "diverticulitis"
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
I now have comprehensive content. Let me compile the full answer.
Diverticular Disease
Definition and Classification
A diverticulum is a hollow outpouching of the bowel wall. Diverticula are classified as:
- Congenital (true) diverticula: All three coats of the bowel wall are present (e.g. Meckel's diverticulum)
- Acquired (false/pseudo) diverticula: No muscularis layer - only mucosa and serosa herniate through the muscular coat (e.g. sigmoid diverticular disease)
Diverticulosis = presence of diverticula without inflammation (usually asymptomatic)
Diverticular disease = symptomatic diverticulosis or diverticulitis
Epidemiology
- Found in the left colon (predominantly sigmoid) in ~75% of those over 70 years in the Western world
- 10-30% of those with diverticulosis will develop symptomatic complications
- Right-sided diverticular disease is more common in South-East Asia
- Rare in Africa and Asia, where dietary fibre intake is high (Burkitt's observation)
Aetiology and Pathogenesis
The mucosal herniation occurs at points where the vasa recta (blood vessels) penetrate the circular muscle layer - these are weak points. The mechanism involves:
- Low-fibre Western diet - decreased stool bulk increases intraluminal pressure
- Altered collagen structure with ageing - weakens bowel wall
- Disordered colonic motility - segmentation contractions generate high pressure
- Narrow sigmoid lumen - highest pressure generated here
The rectum is virtually never affected because it has a complete outer longitudinal muscle coat (taeniae coli fuse) and a wider lumen.
Complications
| Complication | Features |
|---|---|
| Diverticulitis | Microperforation and pericolic inflammation |
| Abscess | Pericolic / pelvic collection |
| Peritonitis | Free perforation |
| Haemorrhage | Typically painless, profuse, from vasa recta erosion |
| Fistula | Colovesical (most common), colovaginal, colocutaneous |
| Intestinal obstruction | Stricture from chronic inflammation |
Hinchey Classification of Complicated Diverticulitis
| Grade | Description |
|---|---|
| I | Mesenteric or pericolic abscess |
| II | Pelvic abscess |
| III | Purulent (generalised) peritonitis |
| IV | Faecal (generalised) peritonitis |
Mortality: inflammatory mass ~3% vs. faecal peritonitis ~33-50%.
Clinical Features
Uncomplicated / mild disease:
- Distension, flatulence, lower abdominal heaviness - often indistinguishable from IBS
- Symptoms thought to arise from increased luminal pressure and visceral hypersensitivity
Acute diverticulitis:
- Persistent left iliac fossa pain (can be right-sided if sigmoid loops across midline - "left-sided appendicitis")
- Accompanying diarrhoea or constipation
- Tenderness over the left iliac fossa
- Tender, thickened sigmoid on palpation
- Tender rectal mass if abscess has formed
- Systemic upset (fever, raised WBC, raised CRP)
Generalised peritonitis (free perforation):
- Systemic sepsis
- Generalised tenderness and guarding
Diverticular haemorrhage:
- Typically painless and profuse
- Bright red blood per rectum (sigmoid) or darker blood (right-sided)
- Torrential bleeding is rare; angiodysplasia is more common cause of massive LGI haemorrhage
Fistula:
- Colovesical (most common): recurrent UTIs, pneumaturia (pathognomonic), faecaluria
- Colovaginal: more common post-hysterectomy
- Colocutaneous: rare without prior intervention
Investigations
Bloods: FBC (leukocytosis), CRP (elevated), U&E, blood cultures if septic
Imaging:
- CT abdomen/pelvis (spiral/contrast): Investigation of choice. Excellent sensitivity/specificity for bowel wall thickening, abscess, extraluminal gas, free perforation. Has transformed management of complicated diverticular disease
- Plain AXR/CXR: Can demonstrate pneumoperitoneum in free perforation
- Contrast enema or CT colonography: Used after 6 weeks (not acutely - risk of perforation) to exclude coexisting carcinoma and assess extent of disease; can demonstrate fistulae
Endoscopy (colonoscopy):
- Deferred 6 weeks after acute episode
- Used to exclude concurrent colorectal carcinoma
- Can be technically difficult / dangerous due to narrowed lumen; significant perforation risk
- May be supplemented by CT virtual colonoscopy
Management
Conservative / Medical
- High-fibre diet (at least 25 g/day, insoluble fibre preferred - wheat bran, bran muffins) and bulk-forming laxatives - evidence for benefit in diverticulosis is limited but widely recommended
- Antispasmodics (e.g. mebeverine) for recurrent pain
- Patients should NOT be told to avoid nuts or seeds - no evidence these precipitate diverticulitis, per Sleisenger and Fordtran's GI and Liver Disease
Acute Diverticulitis - Uncomplicated
- Outpatient management if mild, immunocompetent, no systemic sepsis
- Antibiotics: Selective use only - emerging evidence that uncomplicated diverticulitis is self-limiting and may not require antibiotics in immunocompetent patients without systemic infection signs (confirmed by CT)
- Bowel rest, analgesia, hydration
Acute Diverticulitis - Complicated
- Hospital admission, IV antibiotics (broad-spectrum, cover gram-negatives and anaerobes)
- Hinchey I/II (abscess): CT-guided percutaneous drainage in stable patients avoids emergency surgery
- Hinchey III/IV (peritonitis): Emergency surgery required
Surgical Management
Elective indications: Recurrent attacks, chronic complications (stricture, fistula), inability to exclude carcinoma
Emergency indications:
- Generalised peritonitis
- Failure to respond to optimum medical management
Operative options:
-
Hartmann's procedure (traditional emergency approach):
- Sigmoid resection + end colostomy (left iliac fossa) + closure of rectal stump
- Colostomy reversal as a second stage
- High morbidity; ~40% of colostomies never reversed
-
Primary resection with anastomosis + defunctioning loop ileostomy
- Increasingly favoured in selected patients (less contamination, good performance status)
-
Laparoscopic lavage and drainage
- For Hinchey III (purulent peritonitis) in selected patients
- Avoids stoma; growing evidence base but remains controversial
Elective: Laparoscopic sigmoid resection with primary anastomosis is standard of care for recurrent/complicated disease in fit patients.
Diet, Lifestyle, and Prevention
- High-fibre diet reduces intraluminal pressure and risk of diverticulum formation
- Obesity and physical inactivity increase risk of symptomatic diverticular disease in both men and women
- Probiotics (especially Lactobacillus strains): one systematic review of 11 studies showed symptom regression in the majority of 764 patients, but high-quality data are lacking; current AGA guidelines recommend against routine probiotic use after uncomplicated diverticulitis
Key Points Summary
| Feature | Detail |
|---|---|
| Most common site | Sigmoid colon (75%+ in West) |
| Pathology | False (pseudo) diverticula at vasa recta entry points |
| Key risk factor | Low-fibre Western diet |
| Investigation of choice (acute) | CT abdomen/pelvis |
| Classification system | Hinchey (I-IV) |
| Most common fistula | Colovesical (pneumaturia) |
| Emergency surgery | Hartmann's procedure OR primary anastomosis |
| Mortality (faecal peritonitis) | ~33-50% |
Sources:
- Bailey and Love's Short Practice of Surgery, 28th Ed., Ch. 77 (pp. 1389-1390)
- Sleisenger and Fordtran's Gastrointestinal and Liver Disease
- Rosen's Emergency Medicine: Concepts and Clinical Practice
Recent evidence note: A 2025 systematic review (PMID 41160390) confirms current evidence on preventing onset and recurrence of acute diverticulitis, broadly consistent with the above guidelines.
Image
Loading Image
Loading Image
Finding Sources
Reading File
Finding Sources
Loading Image
Loading Image
All three textbook images retrieved. Here they are with full context:
Diverticular Disease - Textbook Images
(Bailey and Love's Short Practice of Surgery, 28th Ed.)
Fig. 77.13 - CT Scan: Diverticular Abscess
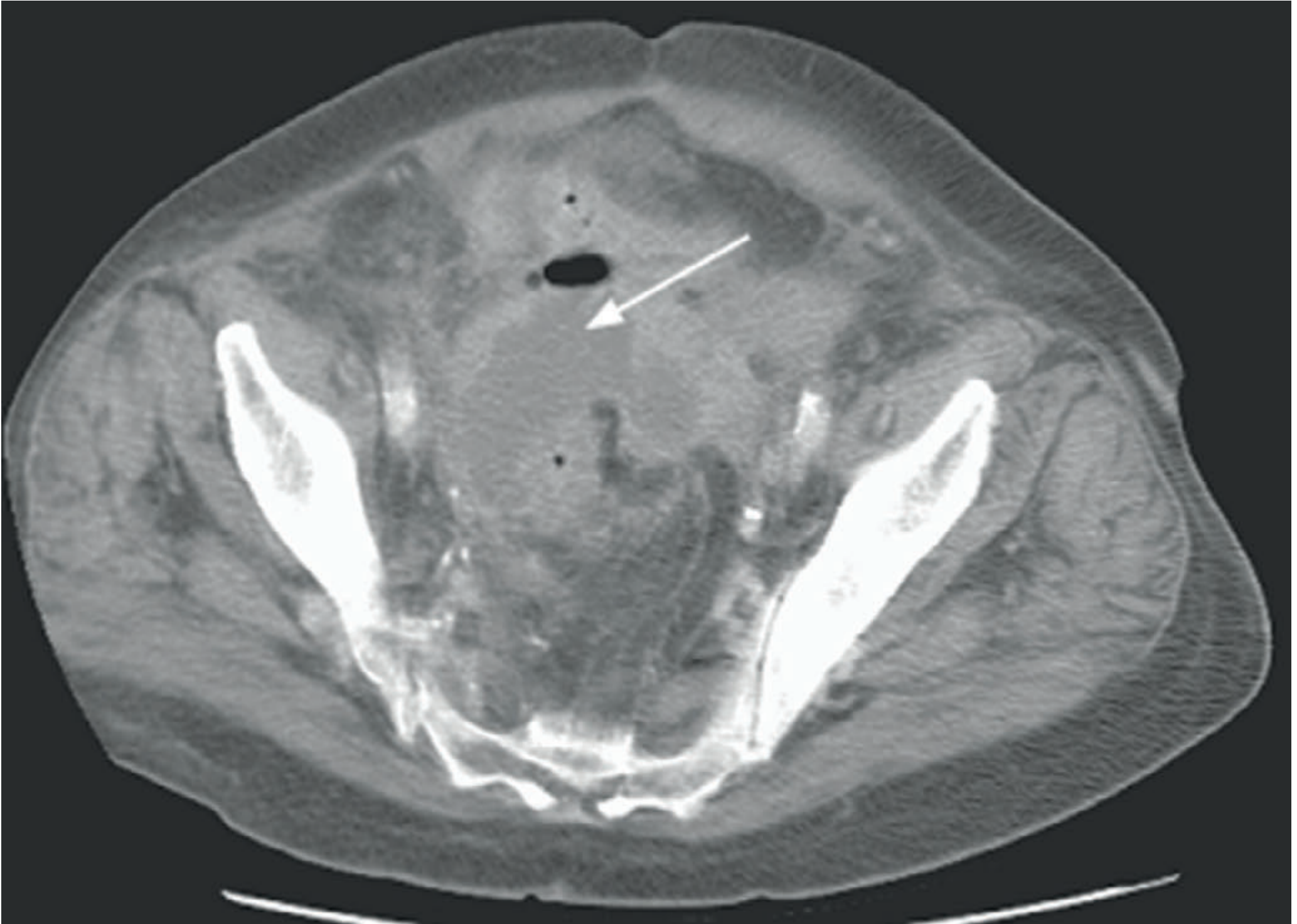
Axial CT of the pelvis showing a pericolic/pelvic abscess (white arrow pointing to the oval hypodense fluid collection) associated with acute diverticulitis. The surrounding soft tissue haziness reflects pericolic fat stranding from inflammation. This is consistent with Hinchey Grade I-II disease. CT is the investigation of choice with excellent sensitivity and specificity for abscess formation, bowel wall thickening, and extraluminal disease.
Fig. 77.14 - Colonoscopy: Right-Sided Diverticula

Colonoscopic view showing multiple diverticular ostia (dark oval openings) along the haustral folds of the right colon. The diverticula appear as clearly defined round/oval pits in the mucosa - these represent the necks of the pseudodiverticula herniating through the circular muscle. Note the otherwise normal-looking mucosa around them. Right-sided diverticular disease like this is more common in South-East Asian populations.
Fig. 77.15 - Hartmann's Procedure Diagram
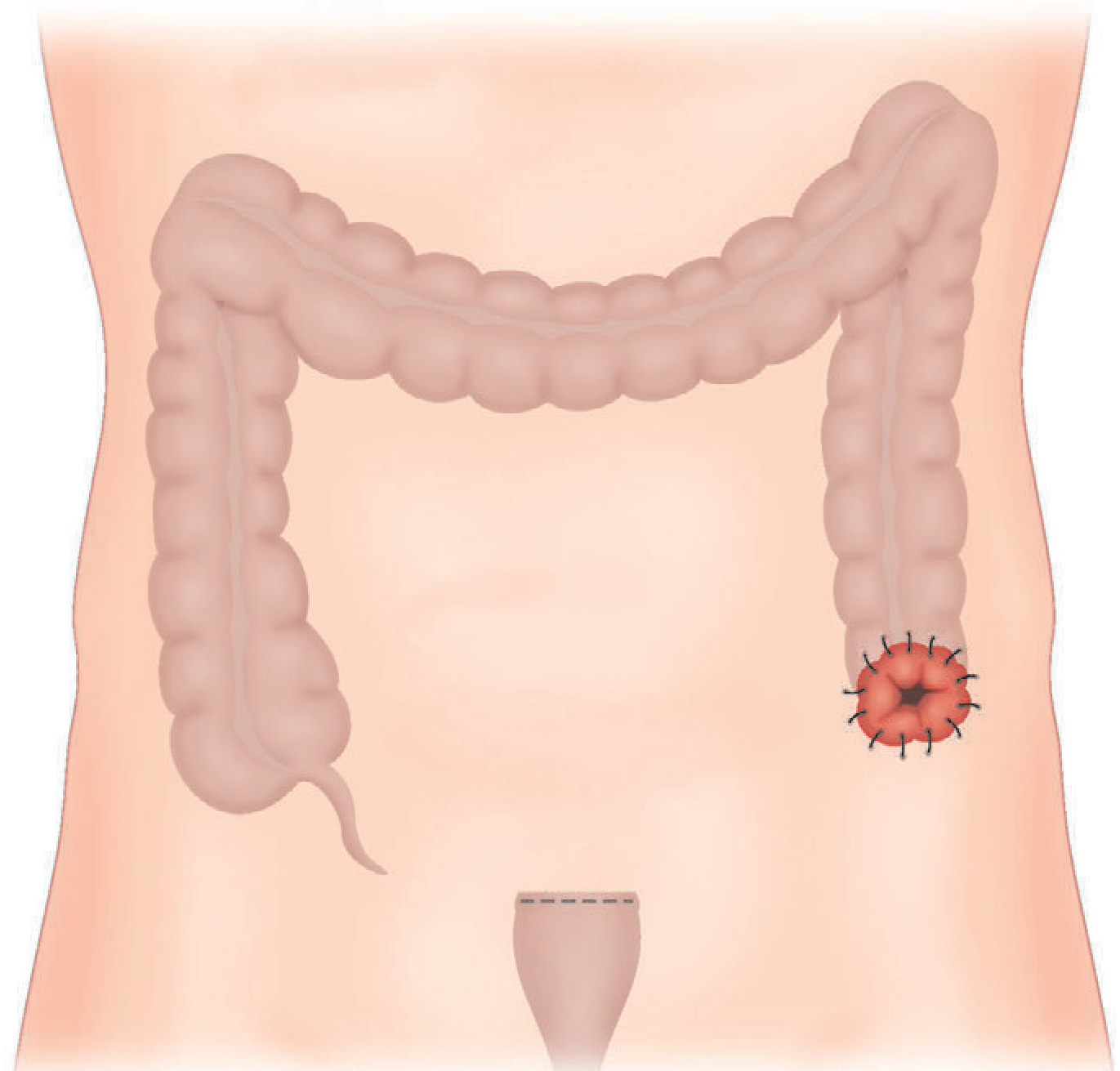
Surgical diagram of Hartmann's procedure - the standard emergency operation for complicated diverticulitis (Hinchey III/IV). The diseased sigmoid colon has been resected. Key features shown:
- End colostomy brought out through the left iliac fossa (red stoma with sutures, visible on the patient's left)
- Oversewn rectal stump (shown as a small capped remnant at the pelvis, marked with dashed line) - the rectum is closed and left in situ
- The remaining colon (ascending, transverse, descending) remains intact
Reversal of the Hartmann's (reconnecting the colon to the rectal stump) is done as a second-stage elective procedure, though ~40% of colostomies from this operation are never reversed due to patient comorbidity.
.
It looks like your message just has a period. Were you trying to say something, or did that send by accident?
Let me know if you'd like to:
- Continue with another topic
- Go deeper on any aspect of diverticular disease
- Move on to something entirely different
This is a shared conversation. Sign in to Orris to start your own chat.