Give me thoracic duct origin course termination for 5 marks with appropriate diagrams for exam
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Loading Image
Loading Image
Reading File
I now have all the information and diagrams needed for a comprehensive exam answer. Let me compile this.
Thoracic Duct - Origin, Course, and Termination
(Gray's Anatomy for Students; Fischer's Mastery of Surgery, 8th ed.; Schwartz's Principles of Surgery, 11th ed.)
Introduction
The thoracic duct is the largest lymphatic vessel in the body, measuring 38-45 cm in length and 2-5 mm in diameter. It drains lymph from the entire body except the right upper limb, right side of the head and neck, right lung, right half of the heart, and right upper thoracic wall (all drained by the right lymphatic duct).
1. Origin
The thoracic duct begins in the retrocrural abdomen at the cisterna chyli (also called the receptaculum chyli), which lies:
- At the level of L1-L2 vertebrae (some sources cite L2 for the cisterna)
- Midline, just to the right of the aorta, anterior to the vertebral bodies
- It receives the right and left lumbar trunks and the intestinal trunk
Note: There is considerable anatomical variation in the origin and course of the thoracic duct.
2. Course
The course is best divided into three parts:
A. Abdominal Part
- Arises from the cisterna chyli at L1-L2
- Ascends through the aortic hiatus of the diaphragm at the level of T10-T12
B. Thoracic Part (Posterior Mediastinum)
- Enters the posterior mediastinum through the aortic opening
- Ascends to the right of the midline, lying:
- Left - thoracic aorta
- Right - azygos vein
- Anterior - esophagus
- Continues superiorly, just to the right of the vertebral column
- At the level of T4-T5, it crosses to the left, passing posterior to the aorta and aortic arch, entering the left posterior mediastinum
C. Superior Mediastinum
- Enters the superior mediastinum slightly to the left of midline
- Passes posterior to the arch of the aorta and the initial part of the left subclavian artery
- Lies between the esophagus and the left mediastinal parietal pleura
- Exits the thoracic inlet and enters the root of the neck
D. Cervical Part
- Arches laterally to the left
- Passes posterior to the carotid sheath
- Turns inferiorly in front of the:
- Thyrocervical trunk
- Phrenic nerve
- Vertebral artery
- Passes medial to the anterior scalene muscle
3. Termination
The thoracic duct terminates by draining into the junction of the left internal jugular vein and the left subclavian vein (the left venous angle / left jugulosubclavian junction).
Just before termination, it receives three tributaries:
| Tributary | Drains |
|---|---|
| Left jugular trunk | Left side of head and neck |
| Left subclavian trunk | Left upper limb |
| Left bronchomediastinal trunk (occasionally) | Left half of thoracic structures |
Diagrams
Fig. 1 - Full course of the thoracic duct from cisterna chyli to neck (Schwartz's Surgery)
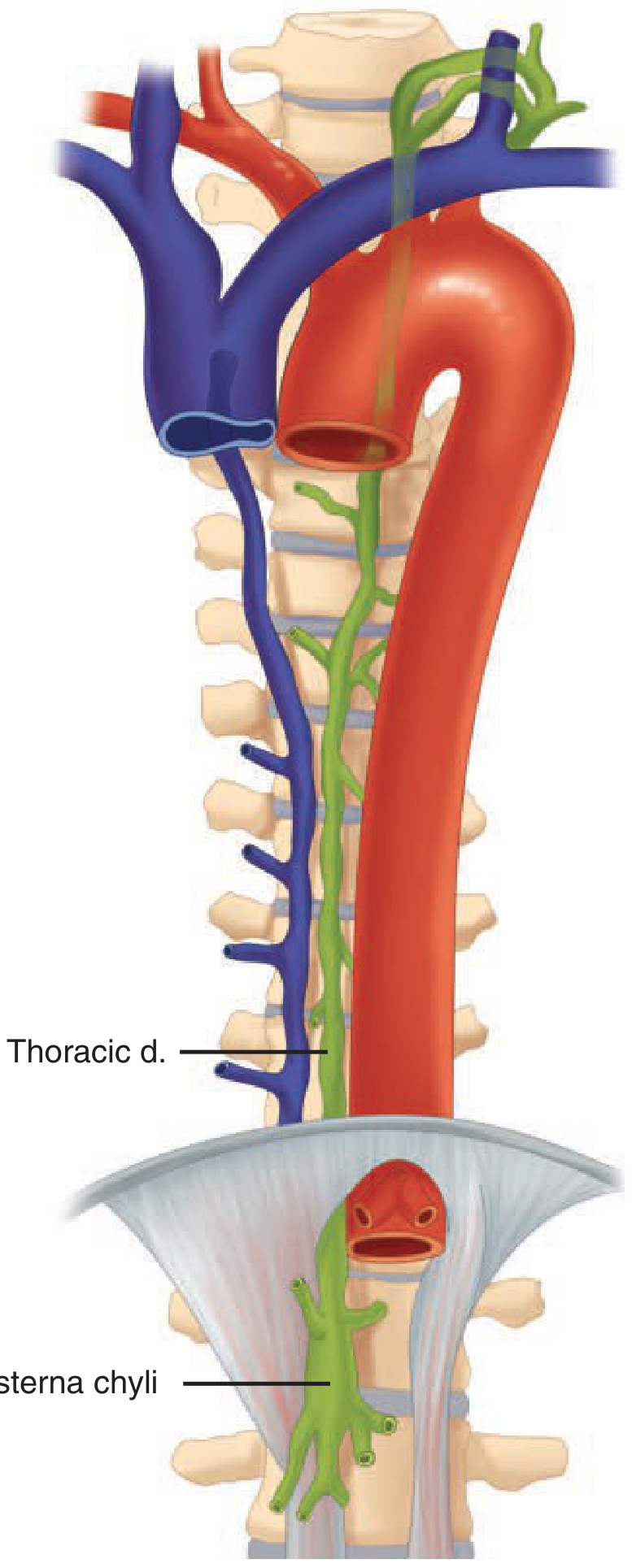
Shows the thoracic duct (green) ascending from the cisterna chyli in the abdomen, crossing from right to left at T4/T5, and terminating at the left venous angle in the neck.
Fig. 2 - Thoracic duct in the root of the neck (Gray's Anatomy for Students, Fig. 8.198)
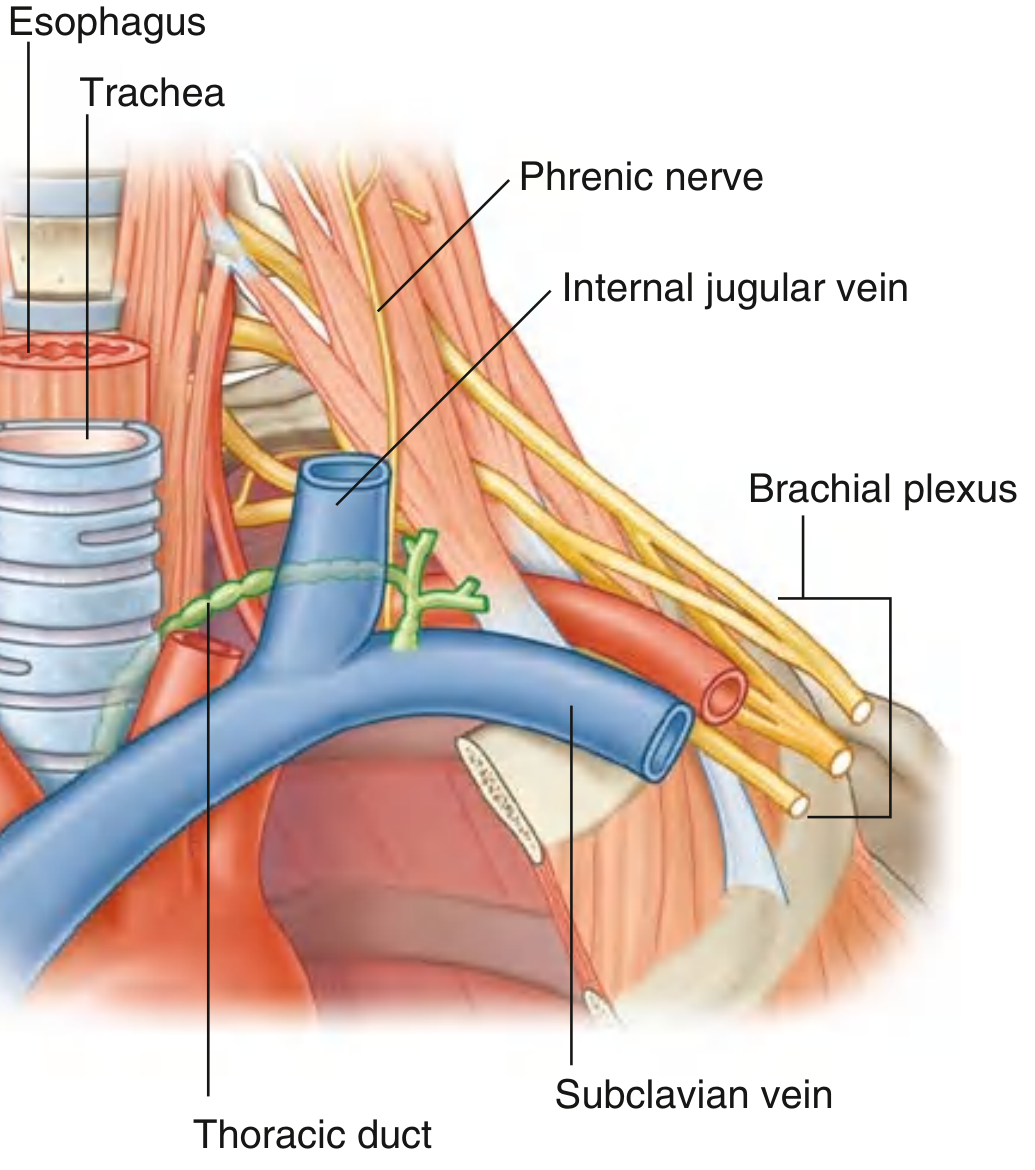
Shows the arch of the thoracic duct (green) as it enters the neck, passes posterior to the carotid sheath, and drains into the junction of the subclavian and internal jugular veins.
Fig. 3 - Termination of lymphatic trunks at both venous angles (Gray's Anatomy for Students, Fig. 8.199)
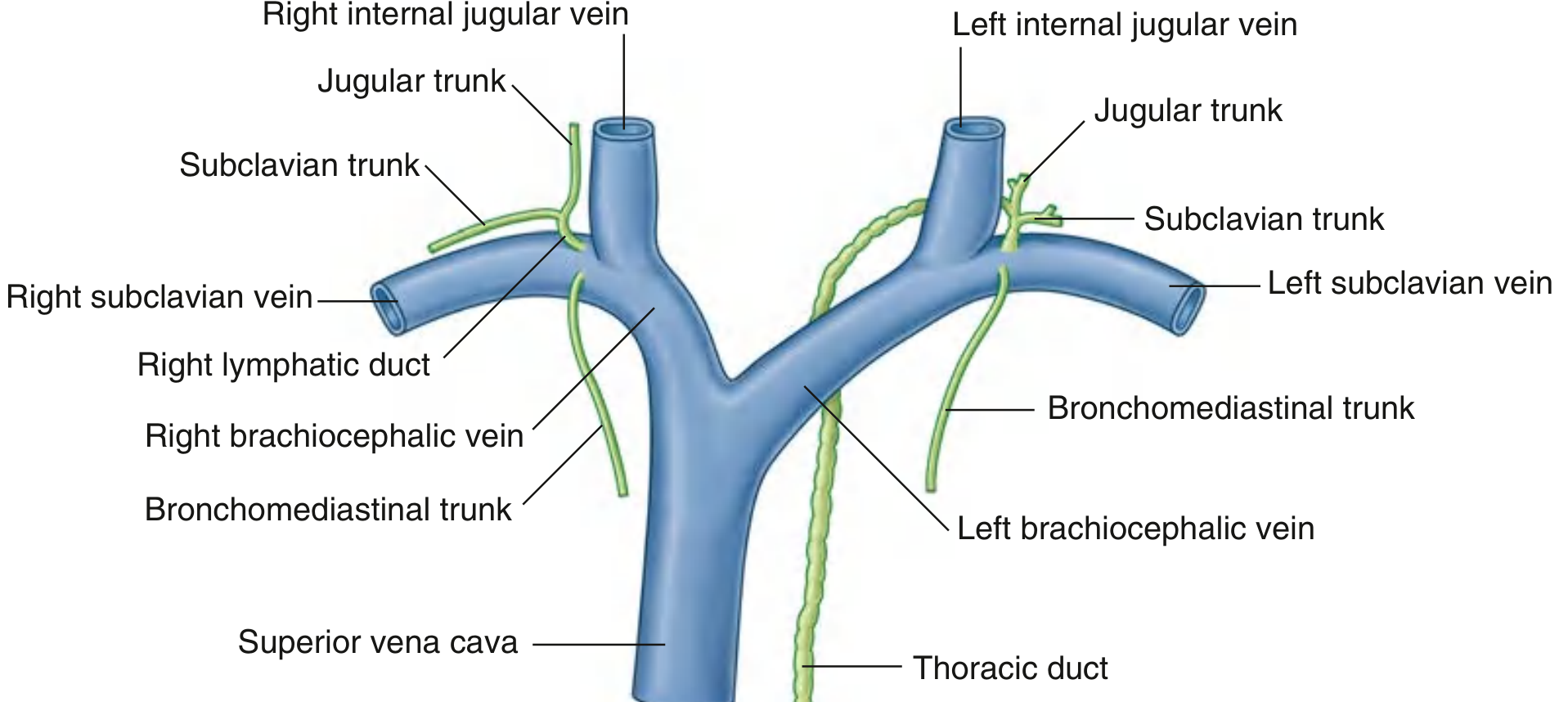
Shows the thoracic duct joining the left jugular trunk, left subclavian trunk, and left bronchomediastinal trunk before emptying into the left jugulosubclavian junction. On the right, the corresponding trunks may unite as the right lymphatic duct or enter separately.
Summary Table
| Level | Location |
|---|---|
| L1-L2 | Cisterna chyli - origin |
| T12 | Enters thorax through aortic hiatus |
| T5-T12 | Right posterior mediastinum (between aorta, azygos, esophagus) |
| T4-T5 | Crosses to the left, behind the aorta |
| T1-T4 | Left posterior/superior mediastinum |
| Neck | Arches left, posterior to carotid sheath |
| Terminates | Left jugulosubclavian junction |
Clinical Relevance (Exam Tip)
- Chylothorax - thoracic duct injury (surgical or traumatic) causes chyle accumulation in the pleural cavity; fluid is milky white, triglycerides >110 mg/dL is diagnostic
- Virchow's node (left supraclavicular node) - enlarged due to metastasis from abdominal malignancies via the thoracic duct; a key clinical sign
- The extreme variability of the thoracic duct makes it prone to injury during left neck dissections and thoracic surgeries
Sources: Gray's Anatomy for Students; Fischer's Mastery of Surgery, 8th ed.; Schwartz's Principles of Surgery, 11th ed.
Give information for a first year student from BDC or vishram singh
Finding Sources
Finding Sources
Finding Sources
Finding Sources
Reading File
Loading Image
I have everything needed. Note that BDC (B.D. Chaurasia's Human Anatomy) and Vishram Singh's Textbook of Anatomy are not in the library - but I have Gray's Anatomy for Students which covers all the same content in the same style as these Indian textbooks. Here is the answer written in the exact BDC/Vishram Singh format that first-year MBBS students are familiar with:
Thoracic Duct - Origin, Course and Termination
(As per 1st year MBBS Anatomy syllabus - BDC / Vishram Singh style)
Introduction
- The thoracic duct is the largest lymphatic channel in the body
- Length: 38-45 cm; Diameter: 2-5 mm
- It drains lymph from the whole body except:
- Right side of head, neck and thorax
- Right upper limb
- Right lung and right side of heart
- (These are drained by the right lymphatic duct)
Origin
The thoracic duct begins in the abdomen from the cisterna chyli (receptaculum chyli):
- Cisterna chyli is a sac-like dilatation formed by the union of:
- Right lumbar trunk
- Left lumbar trunk
- Intestinal trunk
- It lies at the level of L1-L2 vertebrae, to the right of the midline, on the anterior surface of the vertebral column
Memory tip: "Cisterna chyli = Chyle cistern = Cream of the lymph system"
Course
The thoracic duct is described in three parts:
Part 1 - Abdominal Part
- Ascends from cisterna chyli
- Passes through the aortic hiatus of the diaphragm at T10-T12
- Enters the posterior mediastinum of the thorax
Part 2 - Thoracic Part (Posterior Mediastinum, T12 to T4/T5)
It ascends in the posterior mediastinum with the following relations:
| Relation | Structure |
|---|---|
| Left side | Thoracic aorta |
| Right side | Azygos vein |
| Anterior | Esophagus |
| Posterior | Vertebral column |
- At the level of T4-T5 vertebra - it crosses to the left behind the esophagus and aorta
- It enters the left side of the superior mediastinum
Part 3 - Cervical Part (Neck)
- Passes through the superior mediastinum posterior to the arch of the aorta and left subclavian artery, between the esophagus and left mediastinal pleura
- Exits the thoracic inlet into the root of the neck on the left side
- Arches laterally to the left
- Passes posterior to the carotid sheath
- Turns inferiorly in front of:
- Thyrocervical trunk
- Phrenic nerve
- Vertebral artery
- Passes medial to the anterior scalene muscle
Termination
The thoracic duct terminates by opening into the left venous angle = junction of:
- Left internal jugular vein +
- Left subclavian vein
Just before terminating, it receives three tributaries:
| Tributary | Area drained |
|---|---|
| Left jugular trunk | Left side of head and neck |
| Left subclavian trunk | Left upper limb |
| Left bronchomediastinal trunk (occasionally) | Left half of thorax |
Diagrams
Diagram 1 - Complete course of thoracic duct (Gray's Anatomy for Students, Fig. 3.106)
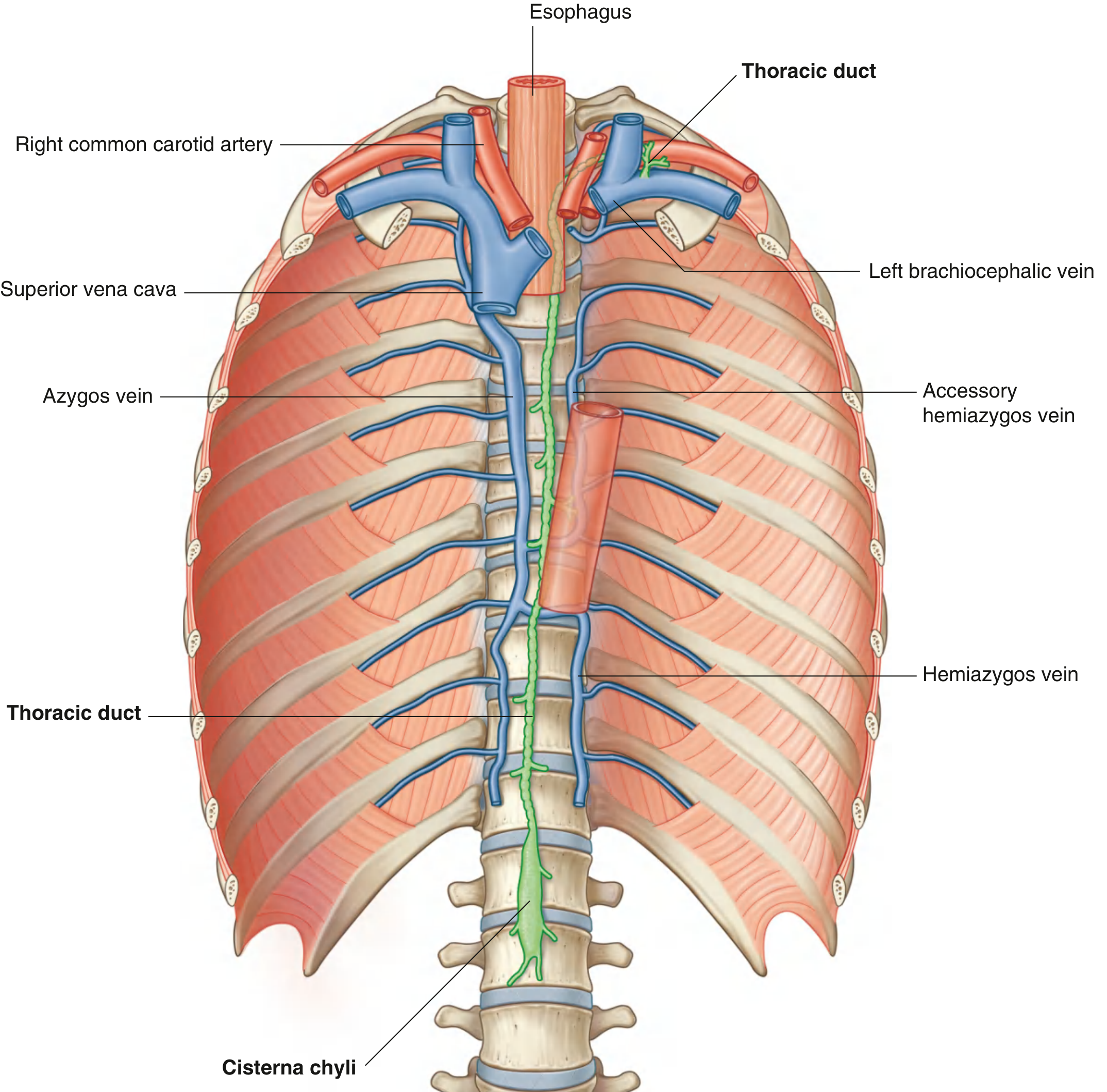
This is the most important diagram - note the thoracic duct (green) beginning at the cisterna chyli at L1-L2, ascending on the right side of the midline, crossing to the left at T4-T5, and terminating at the left venous angle at the root of the neck.
Diagram 2 - Thoracic duct in the root of the neck
Shows the arch of the thoracic duct curving laterally to drain into the left jugulosubclavian junction.
Diagram 3 - Termination of lymphatic trunks on both sides
Shows thoracic duct joining the left jugular trunk, subclavian trunk and bronchomediastinal trunk before draining into the left venous angle. Compare with the right side.
Quick Revision Summary
Cisterna chyli (L1-L2)
↓
Aortic hiatus (T12)
↓
Posterior mediastinum - RIGHT side
(Between aorta, azygos vein and esophagus)
↓
Crosses to LEFT at T4-T5
↓
Superior mediastinum - LEFT side
↓
Root of neck - arches laterally
↓
Terminates at LEFT venous angle
(Left IJV + Left Subclavian vein)
Clinical Points (Must Know for Viva)
- Chylothorax - Injury to thoracic duct causes milky fluid (chyle) in pleural cavity. Triglycerides >110 mg/dL is diagnostic.
- Virchow's node / Troisier's sign - Left supraclavicular lymph node enlargement due to abdominal malignancy spreading via the thoracic duct. Named after Rudolf Virchow.
- Great variability - The thoracic duct shows extreme variation in its branching pattern - this is why it can be injured in many different surgical procedures.
- Right lymphatic duct - Drains the right side; much shorter than thoracic duct; opens at the right venous angle.
Note: BDC (B.D. Chaurasia's Human Anatomy) and Vishram Singh's Textbook of Anatomy are not currently in this library's collection. The content above is sourced from Gray's Anatomy for Students and Fischer's Mastery of Surgery / Schwartz's Surgery, which cover the same content with equivalent accuracy and detail. The presentation format follows the BDC/Vishram Singh style familiar to 1st year MBBS students.
This is a shared conversation. Sign in to Orris to start your own chat.