what are the consequences of dyslipidemia?
Reading File
Finding Sources
Searching PubMed
"dyslipidemia"[MeSH Terms] AND "cardiovascular disease"[MeSH Terms]
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Loading Image
I now have all the information needed for a comprehensive answer. Here it is:
Consequences of Dyslipidemia
Dyslipidemia refers to abnormal levels of lipids in the blood - elevated LDL cholesterol, elevated triglycerides, reduced HDL cholesterol, or some combination. Its consequences span multiple organ systems, with cardiovascular disease being the most significant.
1. Atherosclerosis - The Central Pathological Process
Dyslipidemia is a major, modifiable cause of atherosclerosis. Hypercholesterolemia alone is sufficient to initiate atherosclerotic lesions even without other risk factors (Robbins & Kumar Basic Pathology).
The pathological cascade works as follows:
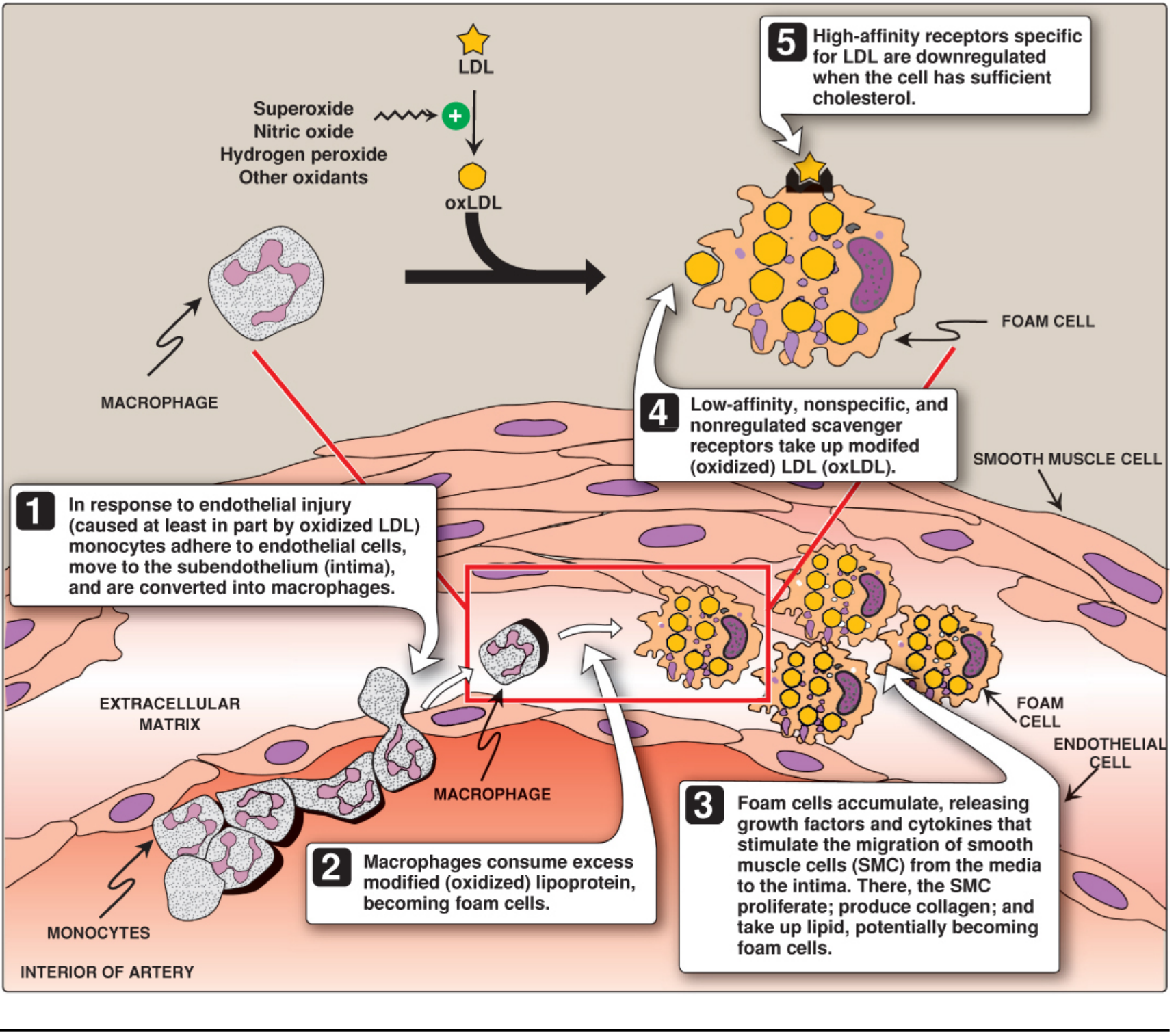
Endothelial dysfunction: Chronic hyperlipidemia increases local reactive oxygen species, which accelerate nitric oxide (NO) decay and impair endothelium-dependent vasodilation.
Foam cell formation and plaque development: LDL particles accumulate in the intima and are oxidized by macrophage- and endothelial-derived free radicals, forming oxidized LDL (oxLDL). Macrophages ingest oxLDL via unregulated scavenger receptors, transforming into lipid-laden "foam cells" - the hallmark of early atheromatous plaques. Foam cells release growth factors, cytokines, and chemokines that recruit more monocytes and stimulate smooth muscle cell migration from the media to the intima.
Cholesterol crystals and inflammasome activation: Cholesterol crystals activate cytosolic innate immune receptors (the inflammasome), triggering IL-1 release and a chronic inflammatory state that drives further plaque progression and complication.
The Framingham study and multiple epidemiologic analyses confirm a significant correlation between total plasma cholesterol/LDL levels and severity of atherosclerosis. Lowering serum cholesterol slows progression, causes partial regression of plaques, and reduces cardiovascular events (Robbins & Kumar Basic Pathology, p. 318).
2. Cardiovascular Consequences
Coronary Artery Disease (CAD) and Myocardial Infarction
Elevated LDL and reduced HDL are among the strongest predictors of coronary heart disease. Plaque rupture in coronary arteries leads to acute myocardial infarction. Familial hypercholesterolemia (defective LDL receptors) can cause MI by age 20 in homozygotes.
Small, dense LDL is an independent risk factor for CAD beyond total LDL-C levels. The ARIC study demonstrated that small, dense LDL independently predicted incident coronary heart disease. These particles are more susceptible to oxidation and more readily enter the vascular wall, inducing ICAM-1, VCAM-1, and monocyte chemoattractant protein-1 (Fuster and Hurst's The Heart, 15th ed).
Stroke
Dyslipidemia promotes carotid artery atherosclerosis and is a major risk factor for ischemic stroke (alongside hypertension, smoking, and diabetes). Carotid stenosis from atherogenic dyslipidemia is a direct precursor to cerebrovascular events (Sabiston Textbook of Surgery).
Peripheral Arterial Disease (PAD)
Atherosclerotic plaques in the arteries of the limbs cause claudication, critical limb ischemia, and gangrene. Dyslipidemia is one of the leading modifiable risk factors for PAD, often coexisting with hypertension and diabetes.
Heart Failure
As ischemic cardiomyopathy from recurrent MI or chronic coronary underperfusion progresses, heart failure develops. Dyslipidemia-driven atherosclerosis is a leading upstream cause.
3. Metabolic Syndrome and Diabetes
Dyslipidemia is both a cause and consequence of insulin resistance. The dyslipidemia of insulin resistance is characterized by:
- Excessive/prolonged postprandial chylomicronemia
- Elevated plasma triglycerides (from increased hepatic VLDL production)
- Low HDL-C (small, dense HDL is rapidly catabolized)
- Increased small, dense LDL (formed via CETP-mediated lipid exchange and hepatic lipase activity)
This pattern creates a highly atherogenic lipid environment even when total LDL-C appears normal, making it particularly dangerous and easy to miss on standard panels (Fuster and Hurst's The Heart, 15th ed).
4. Acute Pancreatitis (Hypertriglyceridemia-Specific)
Severely elevated triglycerides (>1000 mg/dL) - typically from accumulation of chylomicrons and/or large VLDL - cause acute pancreatitis. Hypertriglyceridemia is the third most common cause of acute pancreatitis after gallstones and alcohol, accounting for approximately 9% of all cases. Three typical patient profiles:
- Poorly controlled diabetic with hypertriglyceridemia
- Alcoholic patient with elevated triglycerides
- Non-diabetic, non-alcoholic patient with drug- or diet-induced hypertriglyceridemia
Risk of pancreatitis rises sharply when fasting triglycerides exceed 1000 mg/dL, and is considered very high at levels ≥2000 mg/dL (Sleisenger and Fordtran's GI and Liver Disease; Washington Manual of Medical Therapeutics).
5. Cutaneous Manifestations (Xanthomas)
Lipid deposition in the skin and tendons leads to:
- Xanthelasmas (periorbital) - can cause obstructive blindness if large
- Tendinous xanthomas - may restrict range of motion
- Eruptive xanthomas - appear with severe hypertriglyceridemia, a clinical warning sign
- Plane xanthomas - may be the first sign of hematologic malignancy
Xanthomas are cosmetically significant but also serve as clinical markers of severe underlying dyslipidemia with the attendant cardiovascular and pancreatic risks (Fitzpatrick's Dermatology).
6. Renal Consequences
Dyslipidemia is a complication of nephrotic syndrome and in turn worsens renal outcomes. In chronic kidney disease (CKD) and end-stage renal disease (ESRD), dyslipidemia takes an atypical pattern: high triglycerides and low HDL with relatively normal total/LDL cholesterol. This pattern still accelerates vascular calcification and cardiovascular mortality in renal patients, though it is not the classic atherosclerosis-risk profile (Brenner and Rector's The Kidney).
7. Other Associations
- Pancreatitis in diabetes: Poorly controlled diabetes drives extreme hypertriglyceridemia via overproduction of VLDL, creating a vicious cycle
- Psoriatic arthritis / chronic inflammation: Systemic inflammation accelerates dyslipidemia-driven atherosclerosis
- HIV and antiretroviral therapy: ART (especially protease inhibitors, notably ritonavir) causes marked hypertriglyceridemia and increases LDL-C, creating iatrogenic dyslipidemia with added cardiovascular risk
- Anabolic-androgenic steroids: Cause dyslipidemia with accelerated atherosclerosis, cardiomyopathy, and sudden death
Summary Table
| Consequence | Lipid Driver | Key Outcome |
|---|---|---|
| Atherosclerosis | High LDL, low HDL | Plaque formation, vessel narrowing |
| Myocardial infarction | High LDL, small dense LDL | Plaque rupture, coronary occlusion |
| Stroke | Carotid atherosclerosis | Cerebral ischemia |
| Peripheral artery disease | Systemic atherosclerosis | Claudication, ischemia |
| Acute pancreatitis | TG >1000 mg/dL | Pancreatic inflammation, necrosis |
| Xanthomas | Chylomicrons/LDL | Skin/tendon deposits |
| Metabolic syndrome | Insulin resistance dyslipidemia | T2DM, CVD risk amplification |
| Renal disease progression | Uremic dyslipidemia | Vascular calcification |
Sources: Robbins & Kumar Basic Pathology | Fuster and Hurst's The Heart, 15th ed | Fitzpatrick's Dermatology | Sleisenger and Fordtran's GI and Liver Disease | Washington Manual of Medical Therapeutics | Brenner and Rector's The Kidney
which chapter in lippincott can I find it?
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
which chapter in lippincott can I find it?
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
which chapter in lippincott can I find it?
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
which chapter in lippincott can I find it?
Your credits are exhausted. You can purchase a top-up or subscribe to a plan to continue using Orris. If you're already subscribed, your daily credits will reset tomorrow.
This is a shared conversation. Sign in to Orris to start your own chat.