Here is a complete, MUHS exam-oriented answer covering every SAQ and LAQ topic you listed. Refer Apurb Shastri pattern - define, enumerate, describe, diagrams.
🧬 IMMUNOGLOBULINS & ANTIGEN-ANTIBODY REACTIONS
2nd MBBS Microbiology | MUHS Exam Notes
PART 1 - ANTIBODIES / IMMUNOGLOBULINS
📌 DEFINITION OF ANTIBODY
Antibody (Immunoglobulin): A glycoprotein produced by plasma cells (derived from B-lymphocytes) in response to an antigen, which reacts specifically and non-covalently with that antigen. Also called immunoglobulins (Ig).
📌 CLASSIFICATION OF IMMUNOGLOBULINS
Five classes based on heavy chain type:
| Class | Heavy Chain | Valency | Form | % of Serum Ig |
|---|
| IgG | γ (gamma) | 2 | Monomer | 75-80% |
| IgA | α (alpha) | 2 (serum) / 4 (secretory) | Monomer / Dimer | 10-15% |
| IgM | μ (mu) | 10 | Pentamer | 5-10% |
| IgD | δ (delta) | 2 | Monomer | <1% |
| IgE | ε (epsilon) | 2 | Monomer | Trace |
Subclasses:
- IgG: IgG1, IgG2, IgG3, IgG4
- IgA: IgA1, IgA2
- IgM, IgD, IgE: No subclasses
📌 BASIC STRUCTURE OF IMMUNOGLOBULIN (LABELLED DIAGRAM)
Basic Four-Chain Unit:
Antigen-binding sites
↓ ↓
[VL][VH] [VH][VL]
[CL][CH1] ←Fab→[CH1][CL]
\ Hinge /
\ region/
[CH2][CH2] ← Fc region
[CH3][CH3]
Key Points:
- 2 Heavy chains (H) - ~55,000 Da each (IgG/IgA/IgD) or ~70,000 Da (IgM/IgE)
- 2 Light chains (L) - ~24,000 Da each
- Held together by interchain disulfide bonds
- Light chains: Kappa (κ) or Lambda (λ)
- Variable regions (V): N-terminal, antigen binding - contains 3 CDRs (Complementarity Determining Regions / hypervariable regions)
- Constant regions (C): C-terminal, effector functions
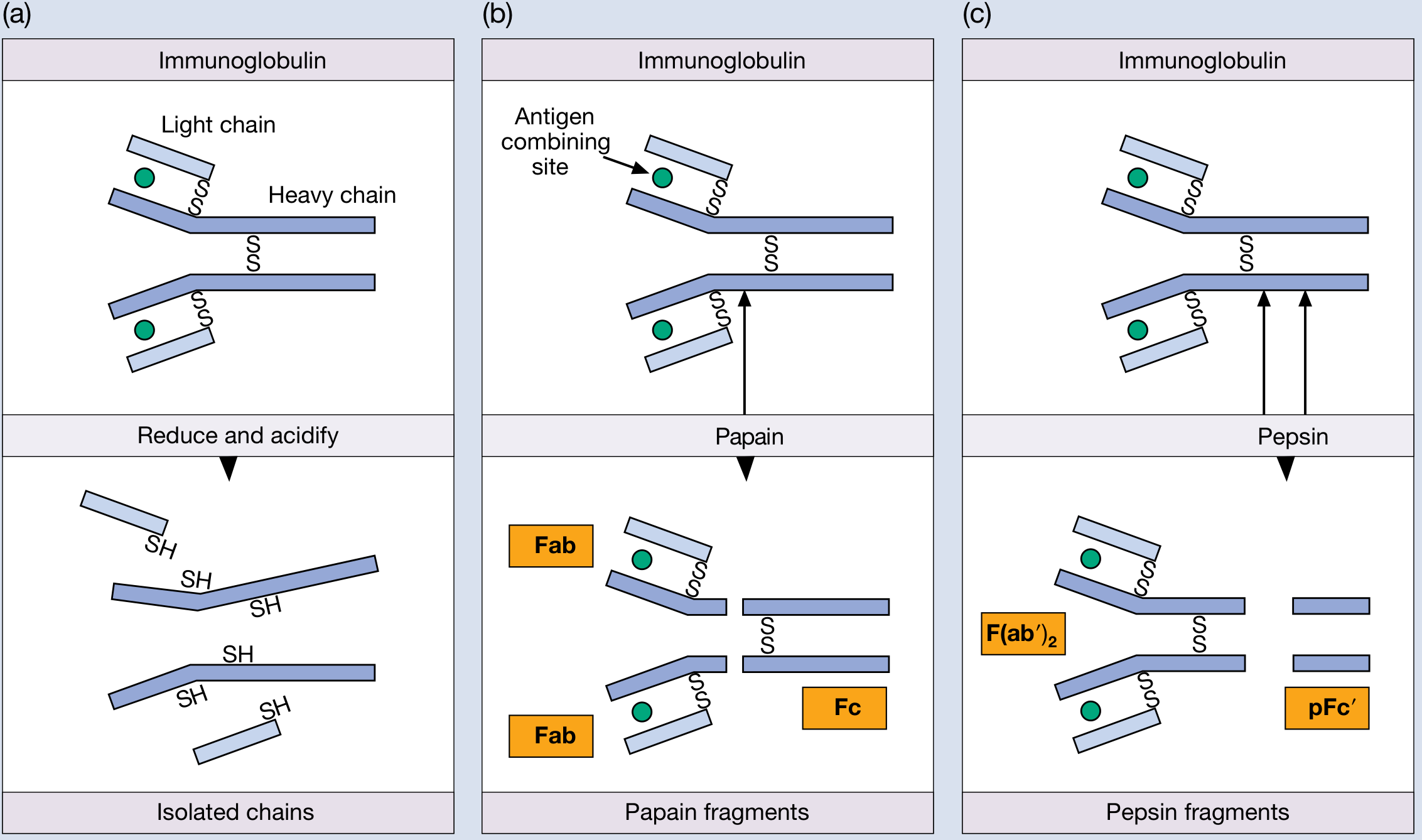
Enzymatic Fragments:
| Enzyme | Fragments | Antigen Binding | Complement |
|---|
| Papain | 2 Fab + 1 Fc | Yes (monovalent) | No |
| Pepsin | 1 F(ab')₂ + pFc' | Yes (divalent) | Yes |
Figure: Immunoglobulin basic unit (IgG), fragmentation by papain (Fab + Fc) and pepsin [F(ab')₂ + pFc'] - Roitt's Essential Immunology
📌 IgG - STRUCTURE & FUNCTION ⭐(MUHS Frequent)
Structure:
- Monomer - basic 4-chain unit (2H + 2L)
- Heavy chain: γ (gamma), MW 55,000 Da
- Domains: VH - CH1 - Hinge - CH2 - CH3
- Hinge region present between CH1 and CH2 (flexible, protease-sensitive)
- 4 subclasses: IgG1 > IgG2 > IgG3 > IgG4 (differ mainly in hinge region)
- Contains N-linked carbohydrate on CH2 domain
- MW: ~150,000 Da
- 2 antigen-binding sites (divalent)
Functions of IgG:
- Major serum antibody - 75-80% of total serum immunoglobulins
- Only Ig that crosses the placenta - provides passive immunity to newborn (via FcRn receptor)
- Opsonization - Fc region binds Fc receptors (FcγR) on phagocytes, enhancing phagocytosis
- Complement activation - IgG1, IgG2, IgG3 activate classical pathway (IgG4 cannot)
- Neutralization of toxins and viruses
- ADCC (Antibody-Dependent Cell-mediated Cytotoxicity)
- Secondary immune response - main antibody produced
- Half-life: ~23 days (longest of all Ig classes)
- Involved in Type II and Type III hypersensitivity
📌 IgM - STRUCTURE, PROPERTIES & FUNCTIONS ⭐⭐⭐ (MUHS Very Frequent)
Structure:
- Pentamer - 5 monomeric units joined by J chain and disulfide bonds
- Heavy chain: μ (mu), MW 70,000 Da
- No hinge region - has extra domain CH2 instead (domains: VH-CH1-CH2-CH3-CH4)
- Has tailpieces at C-terminus of heavy chains (help polymerization)
- MW: ~900,000 Da
- 10 antigen-binding sites (decavalent) - but functionally 5 are usually accessible
- J chain (joining chain, MW ~15,000 Da) links the pentamer
Properties of IgM (Enumerate): ⭐⭐
- Pentameric structure - largest immunoglobulin
- Confined mainly to intravascular compartment (large size prevents tissue entry)
- First antibody produced in primary immune response
- Indicator of acute/recent infection
- Most efficient complement activator (classical pathway) - one IgM molecule sufficient
- Best agglutinating antibody - 10 combining sites
- Does NOT cross placenta
- IgM in cord blood = intrauterine infection (congenital infection marker)
- Found on surface of B lymphocytes as BCR (monomeric form)
- Half-life: ~10 days
- Isohemagglutinins (ABO blood group antibodies) are IgM
- Cold agglutinins are IgM
- Rheumatoid factor (RF) is IgM anti-IgG
Functions of IgM:
- Primary humoral immune response
- Agglutination of particulate antigens
- Complement activation (classical pathway)
- Bactericidal/bacteriolytic reactions
- Acts as BCR on naive B cells
📌 IgA - STRUCTURE & DIAGRAM ⭐
Forms:
| Form | Location | Structure |
|---|
| Serum IgA | Blood | Mostly monomer; small amount dimer |
| Secretory IgA (sIgA) | Saliva, tears, colostrum, respiratory, GI, urogenital secretions | Dimer + J chain + Secretory Component (SC) |
Secretory IgA Diagram:
[Fab][Fab] [Fab][Fab]
\ /
[Fc]—J chain—[Fc]
| |
[Secretory Component (SC)]
(wraps around the dimer - protects from proteases)
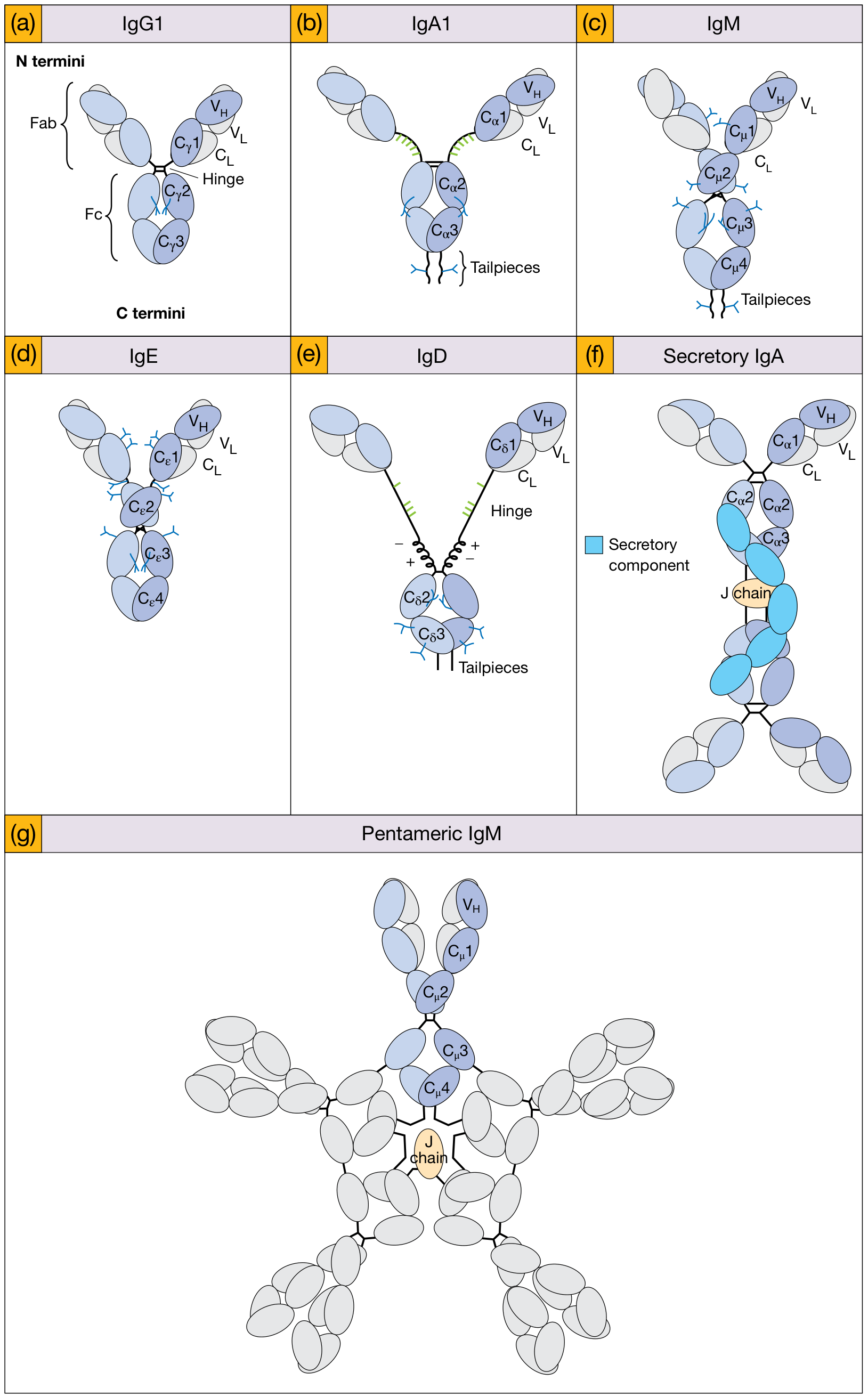
Figure: Schematic structures of all antibody classes (a) IgG1 (b) IgA1 (c) IgM monomer (d) IgE (e) IgD (f) Secretory IgA (g) Pentameric IgM - Roitt's Essential Immunology
Functions of IgA:
- Mucosal immunity - first line of defense at mucosal surfaces
- Prevents microbial attachment to mucosa ("immune exclusion")
- Present in colostrum - passive immunity to newborn via gut
- Secretory component protects sIgA from proteolytic digestion
- IgA1 - more in serum; IgA2 - shorter hinge, more resistant to bacterial proteases
📌 TABLE: PROPERTIES OF ALL IMMUNOGLOBULINS
| Property | IgG | IgA | IgM | IgD | IgE |
|---|
| MW (kDa) | 150 | 160/400 | 900 | 185 | 200 |
| H chain | γ | α | μ | δ | ε |
| Subclasses | 4 | 2 | - | - | - |
| Serum % | 75-80 | 10-15 | 5-10 | <1 | Trace |
| Half-life (days) | 23 | 6 | 10 | 3 | 2.5 |
| Valency | 2 | 2/4 | 10 | 2 | 2 |
| Placental transfer | ✅ Only one | ❌ | ❌ | ❌ | ❌ |
| Complement (classical) | ✅ (G1,2,3) | ❌ | ✅✅ Best | ❌ | ❌ |
| Secretory form | ❌ | ✅ | ❌ | ❌ | ❌ |
| Opsonization | ✅✅ | + | + | - | - |
| Mast cell binding | ❌ | ❌ | ❌ | ❌ | ✅✅ |
| BCR | ❌ | ❌ | ✅ | ✅ | ❌ |
| 1st in primary response | ❌ | ❌ | ✅ | ❌ | ❌ |
| Allergy/Atopy | ❌ | ❌ | ❌ | ❌ | ✅✅ |
PART 2 - ANTIGEN-ANTIBODY (Ag-Ab) REACTIONS
📌 ANTIGEN-ANTIBODY REACTIONS - DEFINITION & GENERAL FEATURES ⭐
Definition: The specific reaction between an antigen and its corresponding antibody. The antigen binds to the antigen-combining site (paratope) of the antibody's Fab region. The interaction is non-covalent (hydrogen bonds, ionic bonds, van der Waals forces, hydrophobic interactions).
General Features (Enumerate): ⭐
- Specificity - Ag reacts only with its specific antibody (lock and key)
- Non-covalent bonds - reversible
- Both Ag and Ab must be multivalent for visible reactions (precipitation/agglutination)
- Equivalence zone - optimal ratio of Ag:Ab for maximum precipitation/agglutination
- Temperature dependent - most reactions optimal at 37°C (some at 4°C, e.g. cold agglutinins)
- Electrolyte (NaCl) required for lattice formation in precipitation
- pH - optimal 6.5-8.0
- Prozone and postzone phenomena occur at extremes of ratio
TYPES of Ag-Ab Reactions:
- Precipitation - soluble Ag + Ab → precipitate
- Agglutination - particulate Ag + Ab → clumping
- Complement fixation
- Neutralization (toxin/virus)
- Opsonization
- ADCC
- Immunofluorescence
- RIA (Radioimmunoassay)
- ELISA
- Western Blot
📌 PROZONE PHENOMENON ⭐
Definition: False-negative result in agglutination or precipitation tests due to excess antibody relative to antigen.
Explanation:
- In prozone: Antibody excess → each antigen molecule is saturated by antibodies → no lattice formation → no visible clumping or precipitation
- When dilutions are made, optimal ratio is reached → reaction becomes visible
- Also called "hook effect" in immunoassays
Postzone:
- Antigen excess → no lattice formation
Equivalence Zone:
- Optimal Ag:Ab ratio → maximum lattice → visible precipitate/agglutinate
PROZONE EQUIVALENCE POSTZONE
(Ab excess) ZONE (Ag excess)
Rxn: ❌ ❌ ❌ ✅✅✅ ❌ ❌
Clinical Significance:
- Widal test - if undiluted serum shows no agglutination but diluted serum does → prozone
- RPR/VDRL for syphilis - prozone common in secondary syphilis
- Always test serial dilutions to avoid missing the reaction
📌 PRECIPITATION REACTIONS ⭐⭐
Principle: When a soluble antigen reacts with its specific antibody in the presence of electrolytes at optimal temperature and pH, insoluble precipitates form at the equivalence zone.
- Requires multivalent antigen and antibody
- Precipitate = lattice of cross-linked Ag-Ab complexes
- Visible only at equivalence zone (not in prozone or postzone)
Types of Precipitation Reactions:
A. In Liquid Medium:
| Test | Description |
|---|
| Ring test (Ascoli's test) | Antigen solution layered over antibody in a tube; precipitate ring forms at interface. Used for anthrax Ag |
| Tube precipitation | Mix Ag + Ab in tube; precipitate at bottom |
| Flocculation test | Fine precipitate (floccules). E.g. VDRL, RPR for syphilis |
B. In Gel (Immunodiffusion):
| Test | Description | Example |
|---|
| Ouchterlony double diffusion | Ag and Ab in separate wells; diffuse toward each other; precipitin line at equivalence | Fungal Ag (Histoplasma), ARC test |
| Single radial immunodiffusion (SRID/Mancini) | Ag diffuses into Ab-containing agar; ring diameter ∝ Ag concentration | Quantify IgG, IgA, IgM levels |
| Immunoelectrophoresis | Ag separated by electrophoresis then reacted with Ab | M-proteins in myeloma |
| Rocket electrophoresis | Ag driven into Ab-agar by electrophoresis; rocket-shaped precipitate | Quantitative |
| Counter-current immunoelectrophoresis (CIEP) | Ag and Ab moved electrophoretically toward each other | HBsAg detection (rapid) |
Agglutination vs Precipitation - Difference: ⭐
| Feature | Agglutination | Precipitation |
|---|
| Nature of Antigen | Particulate (cells, bacteria) | Soluble antigen |
| Sensitivity | More sensitive | Less sensitive |
| Electrolyte | Required | Required |
| Lattice | Visible clumping | Visible precipitate |
| Prozone | Yes | Yes |
| Examples | Widal, ABO typing, Coombs | VDRL, Ouchterlony, SRID |
Two examples of Precipitation tests:
- VDRL / RPR - for syphilis (flocculation/precipitation)
- Ouchterlony double diffusion - for fungal antigens (Histoplasma, Aspergillus)
Two examples of Agglutination tests:
- Widal test - for typhoid fever (tube agglutination)
- ABO blood grouping - slide agglutination
📌 AGGLUTINATION REACTIONS ⭐⭐ (LAQ - MUHS Very Frequent)
Definition: When a particulate antigen (bacteria, RBCs, latex particles coated with antigen) reacts with specific antibody, visible clumping (agglutination) occurs.
Principle:
- Antibody acts as a bridge between particulate antigens
- IgM is the best agglutinating antibody (10 binding sites)
- Requires electrolytes and optimal pH/temperature
- Lattice formation → visible clump
Types / Enumerate:
1. Direct (Active) Agglutination:
Antibody reacts directly with antigen naturally present on the particle.
| Test | Antigen | Detects |
|---|
| Slide agglutination | Bacterial suspension | Rapid ID of unknown culture |
| Tube agglutination (Widal) | Killed Salmonella | Ab titer in patient serum |
| ABO blood grouping | RBCs | ABO antigens on RBCs |
| ASO test | Streptolysin O (particulate) | ASO antibody |
2. Passive (Indirect) Agglutination:
Soluble antigen is coated onto carrier particles (RBCs, latex beads); then agglutination with specific antibody is detected.
| Test | Carrier | Antigen | Detects |
|---|
| TPHA (Treponema pallidum HA) | Sheep RBCs | T. pallidum antigen | Syphilis Ab |
| Latex agglutination | Latex beads | Various | RF, CRP, meningitis Ag |
| PHA (Passive Hemagglutination) | Tanned RBCs | Soluble Ag | Specific Ab |
| RPR | Carbon particles | Cardiolipin | Syphilis screening |
3. Reverse Passive Agglutination:
Antibody coated onto particles; detects antigen in specimen.
- Example: Latex coated with anti-HBsAg antibody → detects HBsAg
4. Agglutination Inhibition:
Patient's antigen competes with particle-bound antigen for limited antibody.
- Example: Latex pregnancy test - detects hCG
- HI test (Hemagglutination Inhibition) - detects antibodies to viruses
5. Coagglutination:
Antibody attached to Protein A of Staphylococcus aureus Cowan I strain (Protein A binds Fc of IgG); unknown antigen causes visible clumping.
- Used for: Rapid identification of bacterial antigens (Streptococcus, N. meningitidis)
6. Antiglobulin / Coombs Test:
Uses anti-human immunoglobulin (AHG) to detect incomplete / non-agglutinating antibodies.
📌 WIDAL TEST ⭐ - DESCRIBE IN DETAIL
Definition: Tube dilution agglutination test to detect agglutinating antibodies against Salmonella Typhi (O and H antigens) in the patient's serum. Described by Fernand Widal (1896).
Principle:
- Patient serum (containing antibodies) + killed Salmonella suspensions (O and H antigens) → agglutination
- The titer (highest dilution showing agglutination) is determined
- A rising titer in paired sera (≥4-fold rise) is diagnostic
Antigens Used:
- O antigen (somatic, lipopolysaccharide) - appears in 2nd week
- H antigen (flagellar) - rises later, persists longer
- Vi antigen (capsular) - detects carriers
Procedure (Tube Agglutination):
- Take a row of 8 tubes
- Add 0.9 mL normal saline to tube 1; 0.5 mL to tubes 2-8
- Add 0.1 mL patient serum to tube 1 → mix → transfer 0.5 mL to tube 2 → serial dilution up to tube 7; tube 8 = antigen control (no serum)
- Dilutions: 1:10, 1:20, 1:40, 1:80, 1:160, 1:320, 1:640
- Add 0.5 mL of specific antigen suspension to all tubes
- Incubate at 37°C for O antigen and 50°C for H antigen for 4-16 hours
- Read results: H agglutination - large fluffy clumps; O agglutination - compact granular deposit
Interpretation:
| Titer | Significance |
|---|
| O antigen >1:80 (in non-endemic) or >1:160 (in endemic) | Suggestive of enteric fever |
| O antigen >1:320 | Significant (diagnostic) |
| H antigen >1:640 | Significant |
| Rise in titer (≥4x) in paired sera 10-14 days apart | Definitive |
Significance / Applications:
- Diagnosis of enteric fever (typhoid) - especially where blood culture is unavailable
- Retrospective diagnosis
- Useful in resource-limited settings
Limitations:
- False positives: other Salmonella infections, malaria, liver disease, immunization
- False negatives: early disease, antibiotic treatment, immunocompromised
- Single serum specimen - unreliable; need paired sera
- Cannot differentiate typhoid from paratyphoid with anti-O only
- Prozone phenomenon possible
📌 PASSIVE AGGLUTINATION TESTS ⭐
Definition: Agglutination tests in which soluble antigens are coated onto carrier particles (usually RBCs or latex beads) so that they can be detected by agglutinating antibodies.
Why "Passive"?
The antigen is NOT naturally part of the particle; it is artificially adsorbed/coupled to it.
Types:
1. Passive Hemagglutination (PHA):
- Soluble Ag adsorbed to tanned (tannic acid-treated) sheep RBCs
- Patient serum added → agglutination = Ag-specific Ab present
- Examples:
- HA test for ABO typing
- Detection of antibodies to soluble polysaccharide or protein antigens
2. TPHA (Treponema pallidum Hemagglutination Assay):
- T. pallidum antigens coated on sheep RBCs
- Detects anti-treponemal antibodies (syphilis)
- Confirmatory test for syphilis
3. Latex Agglutination:
- Latex beads coated with antigen
- Rapid, simple, no need for blood cells
- Examples:
- Rheumatoid factor detection (latex coated with IgG)
- CRP test
- Cryptococcal antigen test (meningitis)
- Bacterial antigen tests in CSF (meningococcal, pneumococcal)
- Pregnancy test (hCG detection - agglutination inhibition)
4. Passive Agglutination Inhibition:
- Soluble antigen in patient specimen competes with latex/RBC-bound antigen for limited specific antibody
- If patient has antigen → no agglutination (positive test)
- Example: Latex pregnancy test, HI (Hemagglutination inhibition) test
5. Reversed Passive Agglutination:
- Antibody coated on particles
- Detects antigen in patient specimen
- Example: Latex coated with anti-HBsAg → detects HBsAg in blood
Advantages of Passive Agglutination:
- More sensitive than direct agglutination
- Can detect soluble antigens/antibodies
- Rapid (minutes to hours)
- No need for intact organisms
📌 ELISA - ENZYME-LINKED IMMUNOSORBENT ASSAY ⭐⭐
Definition: An immunoassay technique in which an enzyme is used as a label on either antigen or antibody to allow detection and quantification through an enzymatic color reaction.
Principle:
- Antigen or antibody is immobilized on a solid surface (polystyrene microtitre plate)
- Enzyme-labeled antibody or antigen binds to the analyte
- On addition of substrate, the enzyme converts it to a colored product
- Color intensity is proportional to the amount of antigen/antibody
- Read by spectrophotometer (ELISA reader)
Enzymes Used:
- Horseradish peroxidase (HRP) - substrate: TMB (turns blue/yellow)
- Alkaline phosphatase - substrate: p-nitrophenyl phosphate (turns yellow)
Types of ELISA:
1. Indirect ELISA (Most Common for Ab detection):
Solid phase (Ag) → Patient Ab → Enzyme-labeled anti-human Ig (secondary Ab) → Substrate → Color
- Detects: Antibody in patient serum
- Used for: HIV antibody detection, ANA, anti-HCV
2. Sandwich / Double Antibody Sandwich ELISA (Best for Ag detection):
Solid phase (Capture Ab) → Antigen → Enzyme-labeled Detection Ab → Substrate → Color
- Detects: Antigen
- Two antibodies bind different epitopes of antigen
- Used for: HBsAg, HCV antigen, hormone quantitation (TSH, hCG, LH)
- High sensitivity and specificity
3. Competitive ELISA:
- Patient antigen competes with enzyme-labeled antigen for limited antibody
- High antigen = less color (inverse relationship)
4. Direct ELISA:
- Antigen immobilized → directly add enzyme-labeled antibody
- Simple but less sensitive
Applications of ELISA: ⭐
| Application | Example |
|---|
| HIV diagnosis | Anti-HIV antibody (screening test) |
| Hepatitis | HBsAg, anti-HCV, anti-HBs |
| Hormones | hCG (pregnancy), TSH, LH, FSH |
| Drugs | Therapeutic drug monitoring |
| Autoimmune | ANA, anti-dsDNA, ANCA |
| Allergy | Total IgE, specific IgE |
| Infectious diseases | Dengue NS1 Ag, Dengue IgM/IgG, malaria Ag |
| Blood bank | Screening donor blood |
| Food safety | Toxin detection |
| Research | Cytokine quantitation, protein measurement |
Advantages:
- Very high sensitivity and specificity
- Can be automated
- Suitable for large-scale screening
- No radioactive material (unlike RIA)
- Long shelf life of enzyme-conjugated reagents
- Quantitative
Limitations:
- False positives (rheumatoid factor interference)
- Prozone/hook effect at very high antibody concentration
- Technical expertise needed
- Cannot distinguish active from past infection (IgG)
📌 COMPARISON: AGGLUTINATION vs PRECIPITATION
| Feature | Agglutination | Precipitation |
|---|
| Antigen | Particulate | Soluble |
| Sensitivity | Higher | Lower |
| Electrolyte needed | Yes | Yes |
| Optimal temperature | Varies | 37°C typically |
| Prozone | Yes | Yes |
| Examples | Widal, ABO typing, Coombs, TPHA | VDRL, Ouchterlony, SRID, CIEP |
| Antibody class | IgM best (direct); IgG (indirect) | IgG best |
| Lattice | Visible clumps | Visible precipitate line/floccule |
📌 QUICK REVISION TABLE - MUHS EXAM POINTS
| Topic | Key Point to Remember |
|---|
| IgG | Only Ig crossing placenta; longest half-life (23 days); 4 subclasses |
| IgM | Pentamer; first in immune response; best complement activator; BCR |
| IgA | Secretory IgA - mucosal immunity; J chain + SC (secretory component) |
| IgE | Mast cell bound; anaphylaxis; allergy; anti-helminthic |
| Prozone | Ab excess → false negative |
| Widal | Tube agglutination; O>1:320, H>1:640 significant |
| Ouchterlony | Double diffusion in agar; lines of identity, non-identity, partial identity |
| ELISA | Sandwich = best for Ag; Indirect = best for Ab; enzyme = HRP/ALP |
| Passive agglutination | Soluble Ag on carrier particle; TPHA, latex, PHA |
| Coombs test | Detects incomplete/non-agglutinating Ab; Direct = on RBC; Indirect = in serum |
📌 EXAM TIP - MUHS PATTERN
- SAQ (5 marks): Define + enumerate/list + brief description + diagram if applicable
- LAQ (10 marks): Define + classify + elaborate each type with principle + examples + table/diagram
- Most repeated: IgG structure+function, IgM properties, Widal test, ELISA, Ag-Ab reactions, Prozone
- Always draw the Y-shaped Ig diagram with labels (VH, VL, CH1-3, hinge, Fab, Fc, disulfide bonds, CDRs)
Sources: Roitt's Essential Immunology 14e; Jawetz, Melnick & Adelberg's Medical Microbiology 28e; Cellular and Molecular Immunology (Abbas); Medical Microbiology 9e (Murray); Harper's Biochemistry 32e