Karititis
Reading File
Finding Sources
Searching the Web
karititis medical condition
Finding Sources
Reading File
Reading File
Reading File
Reading File
Reading File
Reading File
Loading Image
I now have all the information needed for a comprehensive answer. Here it is:
Keratitis (Karititis)
"Karititis" appears to be an alternate spelling or phonetic transcription of keratitis - inflammation of the cornea, the clear dome-shaped tissue covering the front of the eye.
Definition
Keratitis is inflammation of the corneal stroma, epithelium, or both. It may be infectious (bacterial, viral, fungal, protozoal) or non-infectious (trauma, exposure, autoimmune, toxic).
Types and Causes
1. Bacterial Keratitis
The most common form in contact lens wearers. Key pathogens:
- Pseudomonas aeruginosa - Gram-negative rod; ubiquitous in the environment; responsible for >60% of contact lens-related keratitis. Typically aggressive.
- Staphylococcus aureus - Gram-positive commensal of skin/nares; presents as a focal, fairly well-defined white/yellow-white infiltrate.
- Streptococci (S. pneumoniae, S. pyogenes) - often aggressive course.
- Special organisms like Neisseria gonorrhoeae and Corynebacterium diphtheriae can penetrate an intact corneal epithelium - this is unusual.
Risk factors:
- Contact lens wear (especially extended-wear soft lenses) - the single most important risk factor
- Corneal trauma, including refractive surgery (LASIK)
- Chronic ocular surface disease
- Systemic immunosuppression
2. Viral Keratitis (Herpetic / HSV Keratitis)
The classic form is epithelial (dendritic) keratitis - caused by active HSV replication.
Clinical features (in chronological order):
- Reduced visual acuity
- Swollen opaque epithelial cells in a coarse punctate or stellate pattern
- Central desquamation producing a linear-branching (dendritic) ulcer - the hallmark finding
- Branches have characteristic terminal buds; bed stains with fluorescein
- Virus-laden cells at the margin stain with rose Bengal
- Corneal sensation is reduced
- Mild subepithelial haze
- Anterior chamber activity usually mild
Important warning: Topical steroids can promote progressive enlargement of the ulcer to a "geographic" or "amoeboid" configuration.
Classic fluorescein image of herpetic dendritic keratitis:
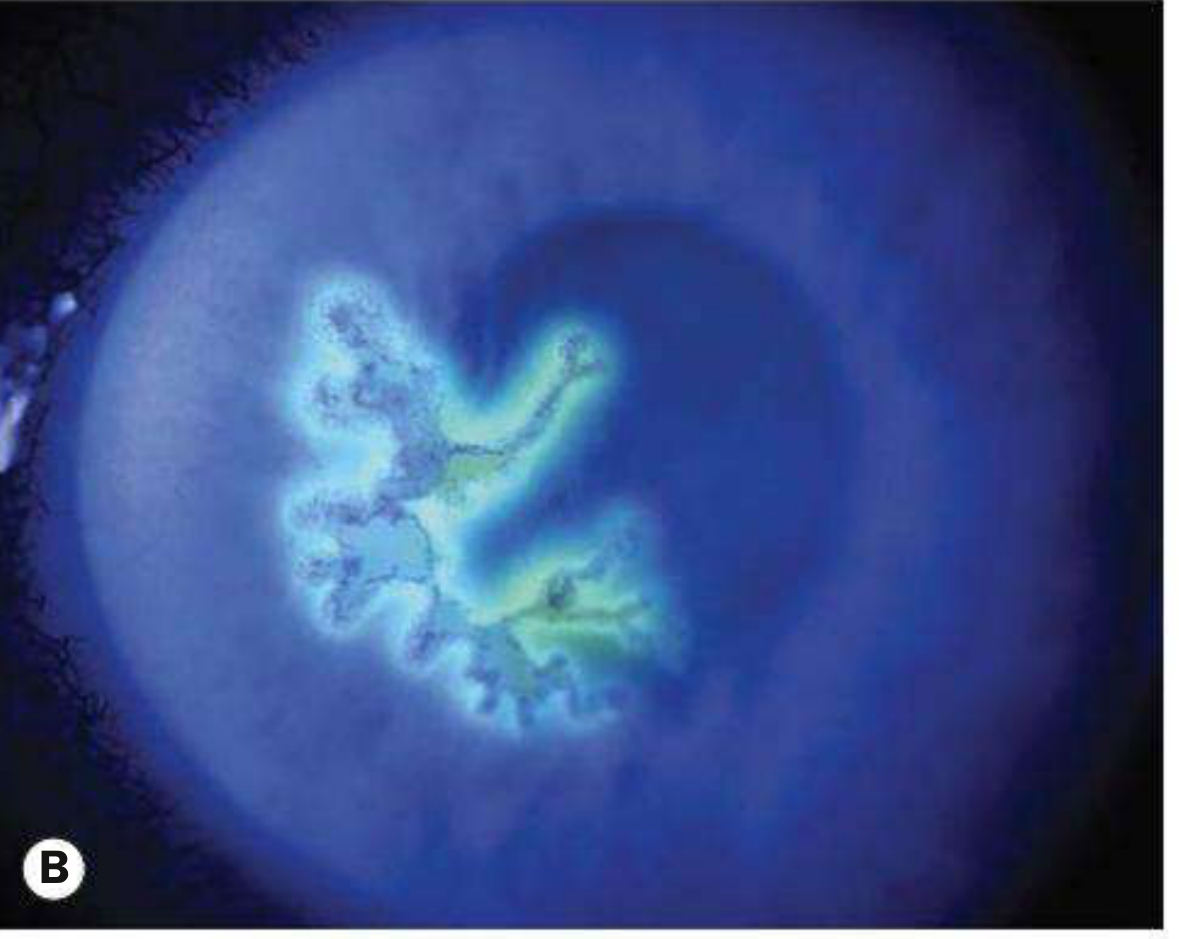
Fluorescein staining showing the characteristic branching (dendritic) pattern of HSV epithelial keratitis - Kanski's Clinical Ophthalmology, 10th ed.
3. Fungal Keratitis
Rare in temperate climates but a major cause of visual loss in tropical/low-income regions.
- Yeasts (Candida): most common in temperate climates; yellow-white densely suppurative infiltrate
- Filamentous fungi (Fusarium, Aspergillus): dominant in tropical climates; associated with plant/agricultural trauma
- Grey or yellow-white stromal infiltrate with indistinct fluffy margins
- Satellite lesions; feathery branch-like extensions
- Can penetrate an intact Descemet membrane and cause endophthalmitis without perforation
Predisposing factors: Long-term topical steroids, chronic ocular surface disease, contact lens wear, systemic immunosuppression, diabetes.
4. Acanthamoeba Keratitis
- Associated with contact lens wear and exposure to contaminated water (tap water, swimming pools)
- Potentially devastating; often initially culture-negative for bacteria
- Increasing in frequency
- Pain classically out of proportion to clinical signs
Clinical Features (General)
| Feature | Details |
|---|---|
| Symptoms | Eye pain, redness, photophobia, blurred vision, watering/discharge |
| Signs | Corneal infiltrate, epithelial defect, anterior uveitis, hypopyon (in severe cases) |
| Severe complications | Descemetocoele, corneal perforation, endophthalmitis, vision loss |
In moderate-severe bacterial keratitis: stromal oedema, Descemet folds, anterior uveitis with hypopyon, chemosis, eyelid swelling. Severe Pseudomonas infections can perforate rapidly.
Investigations
- Corneal scraping - recommended for ulcers that are: >2 mm, involve mid-to-deep stroma, are within the visual axis, chronic, or atypical in appearance
- Gram stain, bacterial/fungal cultures, viral PCR
- Use non-preserved topical anaesthetic (preservatives lower bacterial viability)
- Scrape from the margins and base of the ulcer
Management Principles
Infectious Keratitis
- Topical fluoroquinolones (e.g., ciprofloxacin) are first-line for bacterial keratitis - active against most common pathogens, though resistance exists
- Culture before starting antibiotics when possible
- For viral (HSV): topical antivirals (e.g., aciclovir, ganciclovir); avoid steroids in epithelial disease
- For fungal: topical antifungals (natamycin for filamentous, amphotericin B for Candida)
- Urgent ophthalmology referral - always; if not possible, phone guidance within 24 hours
Caution with Steroids
Topical corticosteroids can promote HSV and fungal replication and retard re-epithelialization. They must be used carefully and only under specialist supervision.
Promoting Epithelial Healing
- Artificial tears, antibiotic ointment prophylaxis
- Bandage soft contact lenses (with close supervision)
- Corneal cross-linking with UV-A + riboflavin (PACK-CXL) for resistant infections with corneal melting
- Amniotic membrane grafting for persistent epithelial defects
- Tissue cyanoacrylate glue for small perforations
- Tarsorrhaphy for exposure or neurotrophic cases
Key Differentials
- Marginal keratitis (peripheral; often immune-mediated)
- Sterile inflammatory infiltrates from contact lens wear
- Peripheral ulcerative keratitis (autoimmune)
- Toxic keratitis
- Conjunctivitis / keratoconjunctivitis
Bottom line: Keratitis is an ophthalmologic emergency. Early slit-lamp examination, culture where indicated, and prompt antimicrobial therapy are the cornerstones of management. Any patient with eye pain, redness, and reduced vision should be seen by an ophthalmologist urgently to prevent permanent vision loss.
Sources: Kanski's Clinical Ophthalmology, 10th ed.; Roberts and Hedges' Clinical Procedures in Emergency Medicine; Goldman-Cecil Medicine
This is a shared conversation. Sign in to Orris to start your own chat.