Larynx notes according to exam point of view
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Loading Image
Reading File
Reading File
Reading File
Loading Image
I now have all the comprehensive information needed. Let me compile the complete exam-focused larynx notes:
🫁 LARYNX - Comprehensive Exam Notes
Sources: Gray's Anatomy for Students, Bailey & Love's Short Practice of Surgery 28e, Color Atlas of Human Anatomy Vol.2, Cummings Otolaryngology, Color Atlas of Human Anatomy
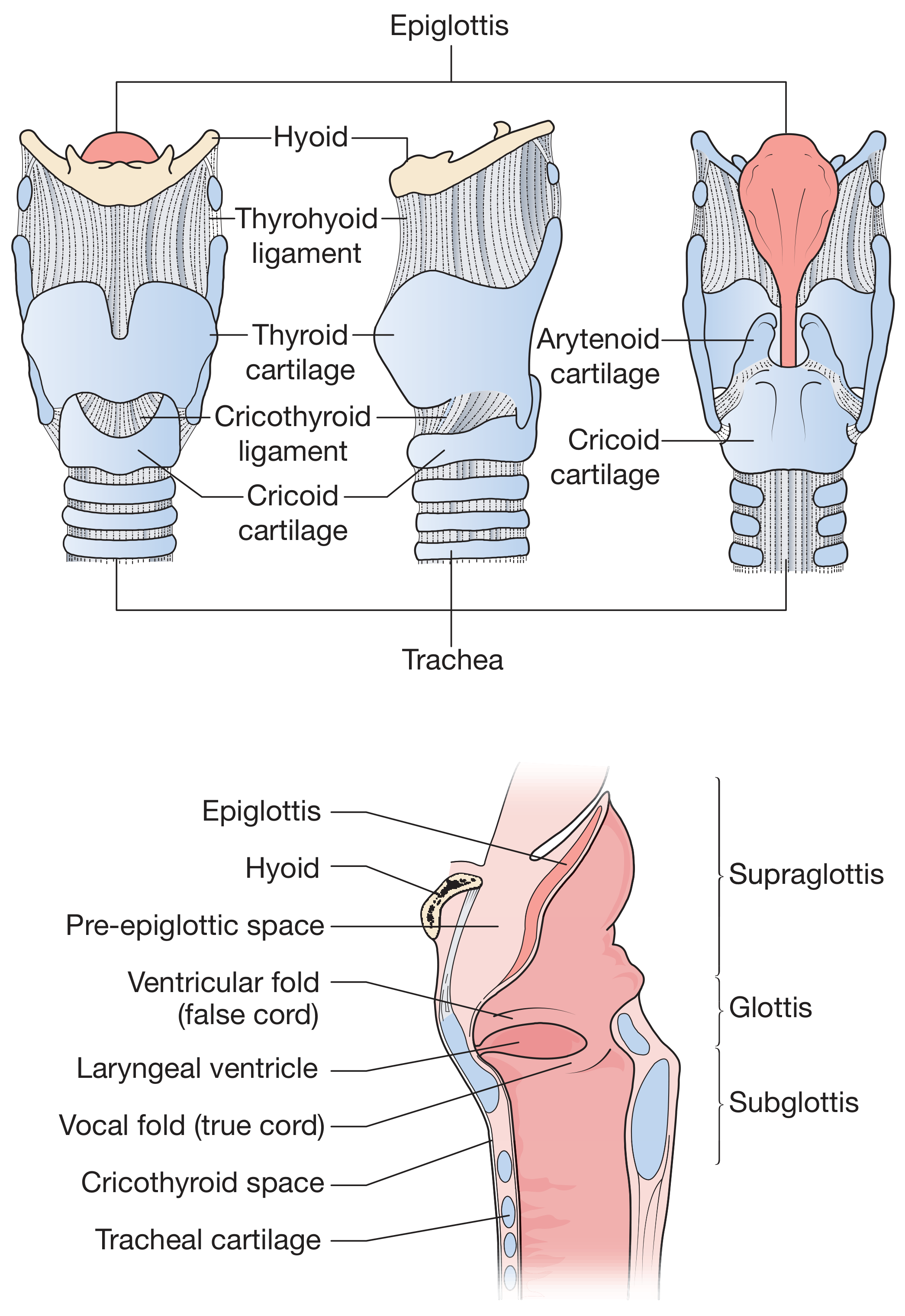
Anatomy of the Larynx - Bailey & Love's view
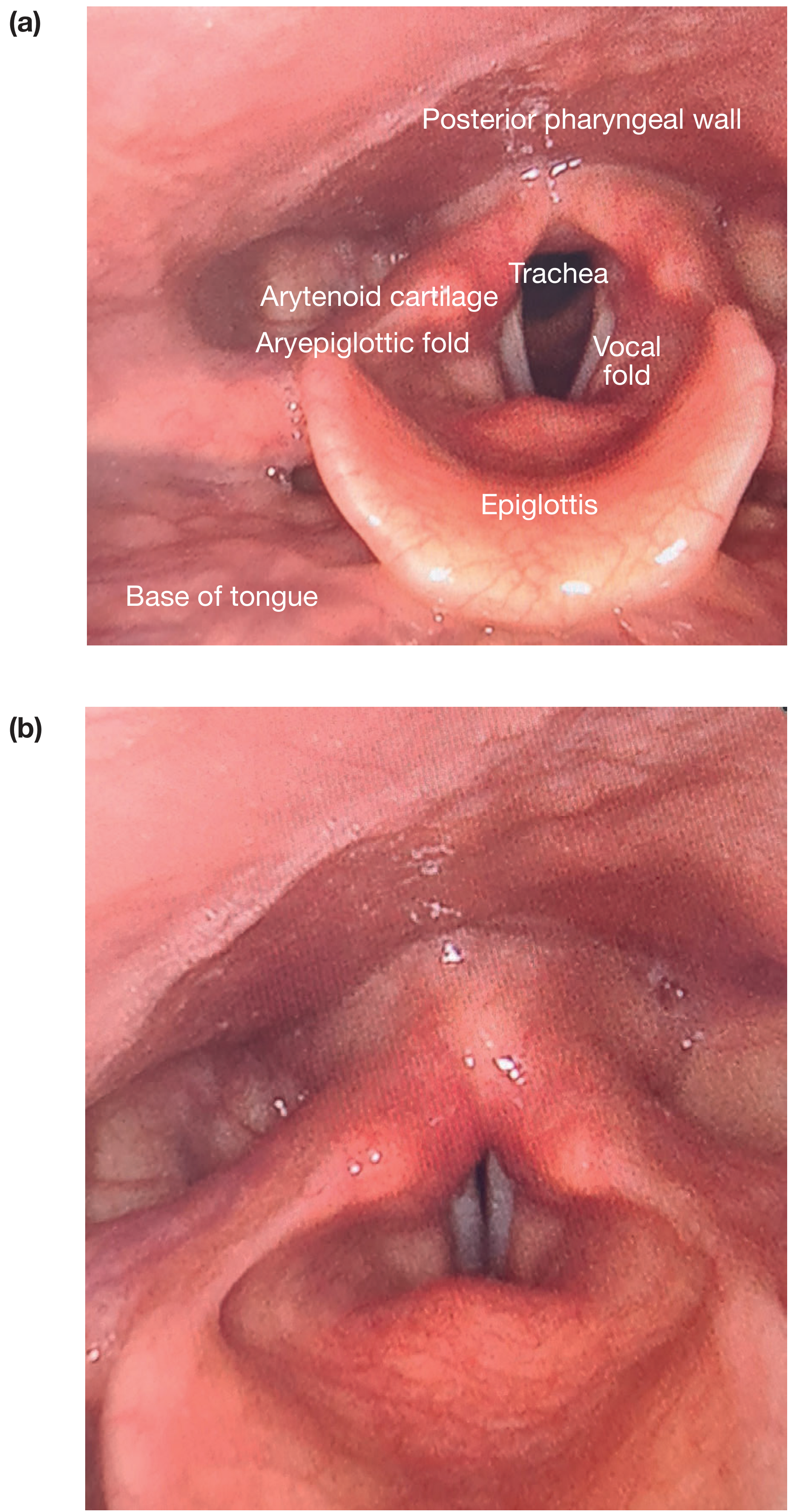
Laryngoscopic view of the larynx (left: abducted vocal folds during inspiration; right: adducted vocal folds):
1. Introduction & Functions
The primary function of the larynx is NOT voice production but protection of the lower respiratory tract - it forms a sphincter with the base of tongue to close the airway during swallowing. Voice is an evolutionary by-product.
Functions (Summary Box - Bailey & Love):
- Protection of lower airway via:
- Closure of the laryngeal inlet
- Closure of the false cords (vestibular folds)
- Closure of the glottis
- Cessation of respiration
- Cough reflex
- Phonation - vocal folds produce sound by quasiperiodic vibration
- Respiration - control of airway diameter
- Effort closure - fixes thorax to stabilize trunk (heavy lifting, Valsalva, defecation)
2. Cartilaginous Framework
The larynx has 3 unpaired + 3 paired cartilages:
Unpaired Cartilages (3)
| Cartilage | Key Features |
|---|---|
| Thyroid | Largest cartilage; two laminae fused anteriorly. Angle 90° in men, 120° in women → more prominent Adam's apple in males. Has superior and inferior horns (cornua). Oblique line on lateral surface for muscle attachment |
| Cricoid | Only complete ring in the entire airway. Signet ring-shaped: broad posterior lamina + narrow anterior arch. Most inferior laryngeal cartilage. Subglottis bounded by cricoid = narrowest point in children's airway (prone to damage from endotracheal tubes) |
| Epiglottis | Leaf-shaped elastic cartilage attached to inner surface of thyroid angle. Attached to hyoid by hyoepiglottic ligament. Attached to tongue by median and lateral glossoepiglottic folds, creating the valleculae (important landmark for intubation) |
Paired Cartilages (3 pairs)
| Cartilage | Key Features |
|---|---|
| Arytenoid | Most important paired cartilage. Pyramidal shape; sits on superior facet of cricoid lamina. Has vocal process (anteriorly - for vocal ligament attachment) and muscular process (posterolaterally - for muscle attachment). Rotatory + gliding movements at cricoarytenoid joint |
| Corniculate | Small, elastic; sit atop arytenoids; form corniculate tubercles in mucosa |
| Cuneiform | Elongated, in aryepiglottic folds; form cuneiform tubercles in mucosa |
Exam tip: Thyroid, cricoid, most of arytenoid = hyaline cartilage (may ossify with age). Epiglottis, corniculate, cuneiform, vocal process of arytenoid = elastic cartilage (never ossifies).
3. Joints of the Larynx
| Joint | Between | Movements |
|---|---|---|
| Cricothyroid joint | Inferior horn of thyroid + lateral surface of cricoid lamina | Rotation + gliding → tilts thyroid forward → tenses vocal folds |
| Cricoarytenoid joint | Base of arytenoid + superolateral facet of cricoid lamina | Rotation → abducts/adducts vocal folds; Gliding → brings/separates arytenoids |
4. Membranes & Ligaments
| Structure | Connects | Significance |
|---|---|---|
| Thyrohyoid membrane | Thyroid cartilage to hyoid bone | Superior laryngeal vessels & internal branch of SLN pierce it |
| Cricothyroid (median) ligament | Thyroid to cricoid cartilage | Site of cricothyrotomy in emergency airway obstruction above vocal folds |
| Cricotracheal ligament | Cricoid to 1st tracheal ring | Marks junction of larynx and trachea |
| Quadrangular membrane | Lateral aryepiglottic folds; free inferior margin = vestibular ligament (false cord) | Forms upper part of fibro-elastic membrane |
| Conus elasticus (cricovocal membrane) | Free superior margin = vocal ligament (true cord) | Forms lower part of fibro-elastic membrane |
5. Divisions of the Larynx (VERY HIGH YIELD)
The laryngeal cavity is divided by two pairs of folds into 3 regions:
Laryngeal Inlet
↓
VESTIBULE (supraglottis)
↓
Vestibular folds (false cords) — pink mucosa
↓
MIDDLE CAVITY (laryngeal ventricle bulges laterally)
↓
Vocal folds (true cords) — WHITE appearance
↓
INFRAGLOTTIC SPACE (subglottis)
↓
Trachea
| Region | Extent | Contents |
|---|---|---|
| Supraglottis | Laryngeal inlet to vestibular folds | Epiglottis, aryepiglottic folds, false cords, laryngeal ventricle |
| Glottis | Vocal folds + rima glottidis (5 mm below) | True vocal folds (vocal cords) |
| Subglottis | Below vocal folds to inferior border of cricoid | Bounded by cricoid cartilage |
Rima glottidis = space between the vocal folds. V-shaped (meeting anteriorly at thyroid angle; separated posteriorly at arytenoids). True vocal folds are WHITE in color (avascular stratified squamous epithelium).
Laryngeal Ventricle: Lateral outpouching between vestibular and vocal folds. Its anterosuperior extension = laryngeal saccule (contains mucous glands).
Laryngocele: Abnormal distension of the saccule due to increased intraglottic pressure (seen in horn players, glass blowers) or obstruction by tumor/inflammation. Internal laryngocele stays inside thyrohyoid space; external (mixed) laryngocele pierces thyrohyoid membrane and presents as neck swelling.
6. Intrinsic Muscles of the Larynx (HIGHEST YIELD)
All intrinsic muscles are innervated by the recurrent laryngeal nerve (RLN), EXCEPT cricothyroid which is innervated by the external branch of the superior laryngeal nerve (eSLN).
| Muscle | Action | Nerve |
|---|---|---|
| Posterior cricoarytenoid (PCA) | ABDUCTS vocal folds (opens rima glottidis) - the ONLY abductor | RLN |
| Lateral cricoarytenoid (LCA) | Adducts vocal folds (closes rima glottidis - intermembranous part) | RLN |
| Transverse arytenoid | Adducts (closes rima glottidis - intercartilaginous part) - only unpaired intrinsic muscle | RLN |
| Oblique arytenoid | Adducts + helps close laryngeal inlet (fibers continue as aryepiglottic) | RLN |
| Cricothyroid | Tenses/lengthens vocal folds (tilts thyroid forward on cricoid) | External SLN |
| Thyroarytenoid (vocalis) | Relaxes/shortens vocal folds; closes rima glottidis | RLN |
| Thyroepiglotticus | Widens laryngeal inlet | RLN |
| Aryepiglotticus | Narrows laryngeal inlet | RLN |
MNEMONICS:
- "PCA is the lifesaver" - Posterior CricoArytenoid is the only Abductor. If both are paralyzed → stridor + respiratory distress.
- "All muscles Adduct, only PCA Abducts"
- Cricothyroid = extrinsic to larynx (outside larynx proper) → supplied by eSLN, NOT RLN.
7. Nerve Supply (VERY HIGH YIELD)
Both nerves are branches of Vagus nerve (CN X):
| Nerve | Branch | Sensory Supply | Motor Supply |
|---|---|---|---|
| Superior Laryngeal Nerve (SLN) | Internal branch (sensory only) | Mucosa above vocal folds (supraglottis) | - |
| Superior Laryngeal Nerve (SLN) | External branch (motor only) | - | Cricothyroid muscle only |
| Recurrent Laryngeal Nerve (RLN) | - | Mucosa below vocal folds (subglottis) | All intrinsic muscles EXCEPT cricothyroid |
Course of RLN:
- Right RLN: Loops under right subclavian artery → shorter intrathoracic course
- Left RLN: Loops under arch of aorta → longer intrathoracic course → more vulnerable to mediastinal pathology (aortic aneurysm, lung cancer, enlarged nodes)
Human communicating nerve: Anastomosis between eSLN and RLN, seen in ~70% of larynges - provides sensory supply to subglottis and motor to thyroarytenoid.
8. Blood Supply
| Vessel | Artery | Vein | Region |
|---|---|---|---|
| Superior laryngeal artery | Branch of superior thyroid artery (from ECA) | Superior laryngeal vein → internal jugular vein | Upper larynx |
| Inferior laryngeal artery | Branch of inferior thyroid artery (from thyrocervical trunk) | Inferior laryngeal vein → brachiocephalic vein | Lower larynx |
The superior laryngeal artery and internal branch of SLN pierce the thyrohyoid membrane together.
9. Lymphatic Drainage (HIGH YIELD for cancer staging)
| Region | Drainage |
|---|---|
| Supraglottis (above vocal folds) | Upper/superior deep cervical lymph nodes (jugulodigastric) - rich lymphatic supply |
| Glottis | Almost NO lymphatics - early glottic cancers rarely metastasize |
| Subglottis (below vocal folds) | Middle and lower deep cervical + pretracheal + paratracheal nodes |
Exam Key: Glottic (true cord) cancers have the best prognosis because of poor lymphatic supply → late metastasis. Supraglottic cancers are often bilateral because of rich bilateral lymphatics.
10. Phonation and Respiration
Phonation mechanism:
- Vocal folds adduct; subglottic air pressure forces them apart momentarily → quasiperiodic vibration → sound column
- Pitch controlled by tension (cricothyroid lengthens/tenses; vocalis relaxes/shortens)
- Rima glottidis is V-shaped; intermembranous part (anterior) closed by LCA; intercartilaginous part (posterior) closed by transverse arytenoid
Respiratory positions:
- Quiet respiration: rima glottidis triangular
- Forced inspiration: PCA contracts → arytenoids rotate laterally → rima glottidis opens wide (rhomboid shape)
- Effort closure: rima glottidis + rima vestibuli both closed (e.g., lifting, coughing, defecation)
Swallowing:
- Larynx moves up and forward → epiglottis tilts over laryngeal inlet
- Rima glottidis + rima vestibuli both close
- Laryngeal elevation also opens esophagus (attached to posterior cricoid)
11. Embryology (Exam Points)
| Pharyngeal Arch | Contribution to Larynx |
|---|---|
| 4th arch | Cricothyroid muscle, laryngeal cartilages (thyroid, cricoid); innervated by superior laryngeal nerve |
| 6th arch | All other intrinsic laryngeal muscles; innervated by recurrent laryngeal nerve |
12. Clinical High-Yield Points
Recurrent Laryngeal Nerve Palsy
- Unilateral RLN injury: Vocal fold on affected side lies in adducted/paramedian position → hoarseness (dysphonia)
- Bilateral RLN injury: Both folds adduct → stridor + respiratory obstruction → may need tracheostomy (bilateral PCA paralyzed; no abduction possible)
- Causes: Thyroid surgery (most common), aortic aneurysm (especially left), mediastinal tumors, lung cancer, neck trauma
Superior Laryngeal Nerve Injury
- External branch injury (during thyroidectomy) → weakness of cricothyroid → loss of voice pitch control, loss of high-pitched singing → common in singers
Cricothyrotomy
- Emergency airway access when obstruction is above the vocal folds (e.g., anaphylaxis, foreign body supraglottis)
- Site: Median cricothyroid ligament, lower third of cricothyroid membrane
- Preferred over tracheotomy in emergencies (faster, more accessible)
Subglottic Stenosis
- Cricoid cartilage = narrowest part of airway in children (not true in adults where glottis is narrowest)
- Prolonged endotracheal intubation in ICU patients → pressure necrosis → subglottic stenosis
- Presents with stridor and respiratory distress
Laryngocele
- Abnormal air-filled dilation of laryngeal saccule
- Internal: Within paralaryngeal fat - may present as airway compromise
- External (mixed): Extends through thyrohyoid membrane → neck swelling (increases with Valsalva)
- Association with glottic tumors causing obstruction of the saccule
Epiglottitis
- H. influenzae type B (children) or Streptococcus (adults)
- "Thumbprint sign" on lateral soft tissue X-ray (thickened epiglottis)
- "Cherry red epiglottis" on laryngoscopy
- NEVER do throat examination in children - can precipitate complete obstruction
Laryngeal Cancer
- Most common site: Glottis (true vocal folds) - 60-65%
- Supraglottis: 30-35%; Subglottis: rare (<5%)
- Glottic: Best prognosis (avascular area, early hoarseness alerts patient, poor lymphatics)
- Supraglottic: Late presentation, bilateral nodal metastasis common
- Risk factors: Smoking + alcohol (synergistic), GERD, voice abuse
Reinke's Space (Reinke's Edema)
- Potential space between the vocal fold epithelium and the vocal ligament
- Edema here (from smoking, voice abuse, hypothyroidism) → Reinke's edema → hoarse low-pitched voice
13. Quick Summary Table - Nerve to Muscle
| Nerve | Muscles |
|---|---|
| External SLN | Cricothyroid only |
| Recurrent LN | Posterior cricoarytenoid, Lateral cricoarytenoid, Transverse arytenoid, Oblique arytenoid, Thyroarytenoid (Vocalis), Aryepiglotticus, Thyroepiglotticus |
14. Vertebral Level Relations
| Structure | Vertebral Level |
|---|---|
| Hyoid bone | C3 |
| Thyroid cartilage (superior notch) | C4-C5 |
| Vocal folds / Glottis | C5 |
| Cricoid cartilage | C6 |
| Trachea begins | C6 |
Exam tip: Cricoid cartilage at C6 = landmark for: (1) Start of trachea, (2) End of pharynx/start of esophagus, (3) Change of common carotid to internal carotid, (4) Inferior thyroid artery entry, (5) Level of cricothyrotomy
Sources: Gray's Anatomy for Students, p.1192-1204 | Bailey and Love's Surgery 28e, p.798 | Color Atlas of Human Anatomy Vol.2, p.196-203 | Cummings Otolaryngology Head & Neck Surgery
This is a shared conversation. Sign in to Orris to start your own chat.