Neck of femur fracture
Reading File
Finding Sources
Finding Sources
Searching PubMed
"femoral neck fracture" AND management
Reading File
Reading File
Reading File
Reading File
Finding Sources
Finding Sources
Finding Sources
Reading File
Reading File
Reading File
Reading File
Loading Image
Loading Image
I now have comprehensive information to deliver a detailed, well-cited answer. Let me compile everything.
Fracture of the Neck of Femur (NOF Fracture / Hip Fracture)
Epidemiology
Femoral neck fractures are among the most common orthopaedic injuries encountered clinically. They occur predominantly in older adults (women > men), with falls accounting for ~90% of cases. Most elderly patients sustain this fracture due to underlying osteoporosis - the fall is often the result of the fracture completing itself, not the cause. In younger patients, high-energy trauma (MVA, falls from height) is required to fracture a normal femoral neck.
- Mortality in the first year after a femoral neck fracture is ~14%, compared with ~9% in a matched control population
- Risk factors for higher mortality: age, male sex, psychiatric illness, end-stage renal disease, congestive heart failure, and institutionalisation (death rate up to 3x higher)
Anatomy & Blood Supply
The femoral neck is almost entirely intracapsular. Its blood supply comes from three sources:
- Retinacular vessels (most important) - branches of the medial circumflex femoral artery running deep to the synovium along the femoral neck in fibrous retinacula
- Medullary cavity vessels - attenuated with age due to fatty marrow replacement
- Ligamentum teres artery - also attenuated with age and atherosclerosis
Key clinical point: In an intracapsular displaced fracture, the retinacular vessels are torn. This is why AVN of the femoral head is the dominant complication. In an extracapsular (intertrochanteric) fracture, these vessels are spared.
Why the leg is shortened and externally rotated: The psoas major inserts on the lesser trochanter - it externally rotates and flexes the hip using the femoral head as a fulcrum. When the neck is disrupted, the psoas pulls the femoral shaft proximally and into external rotation. The adductor muscles exacerbate external rotation through spasm.
Classification
By Location (Anatomical)
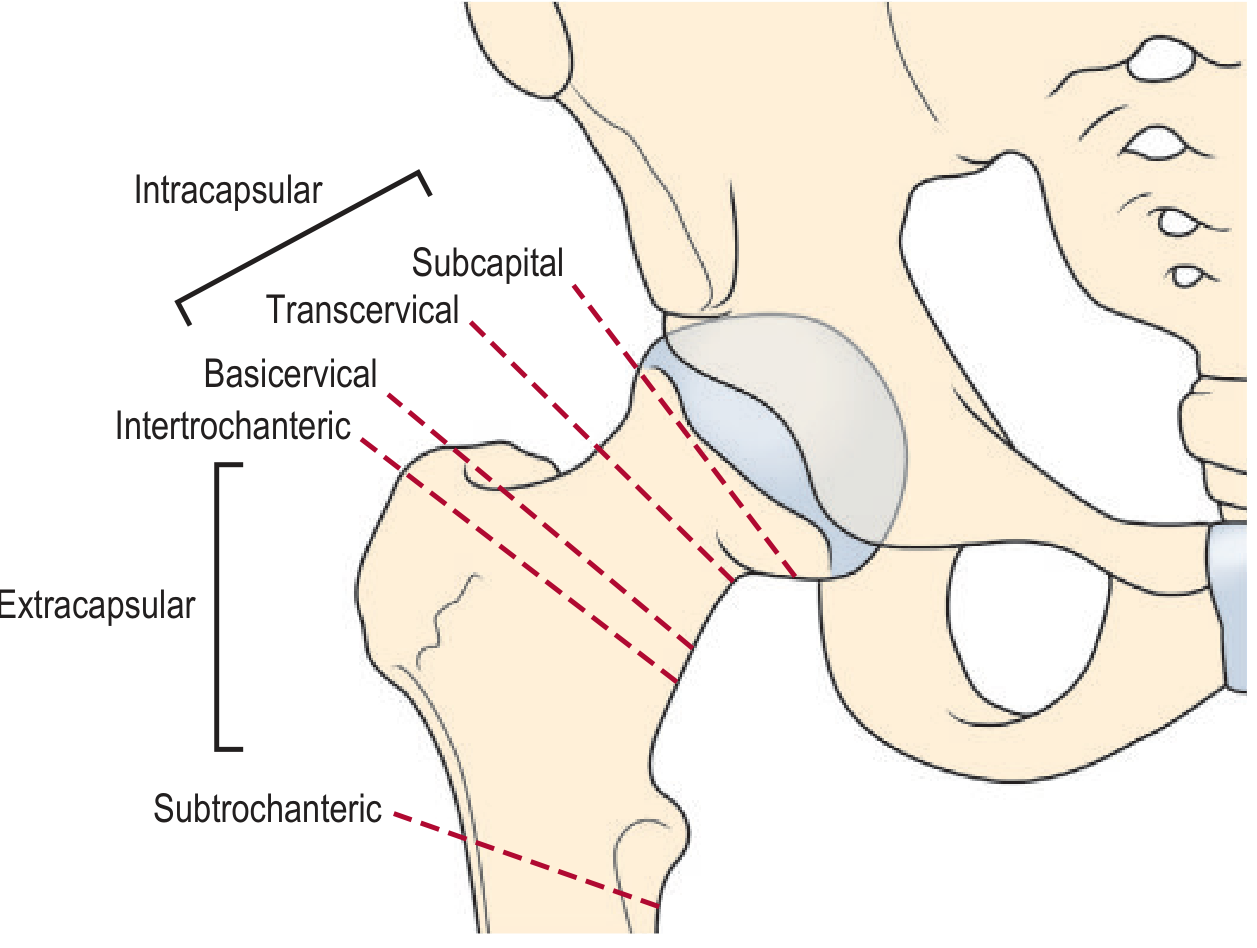
| Region | Type | Capsule | AVN Risk |
|---|---|---|---|
| Subcapital | Intracapsular | Inside | High |
| Transcervical | Intracapsular | Inside | High |
| Basicervical | Intracapsular | Inside | Moderate |
| Intertrochanteric | Extracapsular | Outside | Low |
| Subtrochanteric | Extracapsular | Outside | Very low |
Garden Classification (Intracapsular Fractures)
| Grade | Description | Displacement |
|---|---|---|
| I | Incomplete/impacted - valgus impacted | Undisplaced |
| II | Complete, no displacement | Undisplaced |
| III | Complete, partial displacement | Displaced |
| IV | Complete, full displacement | Displaced |
Garden III and IV carry the greatest risk of disrupting the retinacular blood supply and causing AVN (15-35% of patients). For clinical purposes, they are most usefully described as simply displaced (Garden III/IV) or undisplaced (Garden I/II).
Delbet Classification (Paediatric)
| Type | Fracture | AVN Risk |
|---|---|---|
| I | Transphyseal | ~100% |
| II | Transcervical | ~50% |
| III | Basicervical/cervicotrochanteric | 20-30% |
| IV | Intertrochanteric | 10-15% |
Clinical Presentation
Displaced fracture:
- Severe groin/hip pain, unable to weight-bear
- Limb held in shortening, external rotation, and abduction
- Range-of-motion assessment should be deferred to avoid further vascular disruption
Undisplaced / stress fracture:
- May be ambulatory
- Groin or inner thigh pain, aggravated by walking and weight-bearing
- Night pain can develop if diagnosis is delayed (athletes)
- On examination: discomfort at extremes of rotation (especially internal rotation)
Investigations
Plain radiographs - AP pelvis and lateral hip view (mandatory)
- Displaced fractures are obvious on AP view
- A lateral view is critical - it often reveals fractures not visible on AP
- Look for: disruption of the bony cortex or trabecular lines
- Impacted undisplaced fractures show a sclerotic line and/or disrupted trabecular pattern
- ~15% of fractures are difficult to detect on plain films
- ~6-9% have an ipsilateral femoral shaft fracture (always check in high-energy trauma)
- Note: Shenton's line and neck-shaft angle are unreliable for fracture identification
MRI - Now considered the standard of care when plain radiographs are normal but clinical suspicion remains. More sensitive and specific than bone scan or CT for stress fractures.
CT - Useful when MRI is unavailable; confirms subtle fractures.
Management
Emergency Department
- Maintain the extremity in a position of comfort
- No additional external immobilisation required
- Skeletal traction is contraindicated - may worsen AVN by stretching retinacular vessels
- "Buck's" boot traction is no longer recommended
Surgical Management
Treatment depends on fracture location, displacement status, patient age, and functional demands.
Undisplaced Intracapsular Fractures (Garden I/II)
- Cannulated screws - 3 partially threaded screws (6.5-7.3 mm) in an inverted triangle configuration, inserted under fluoroscopy
- Allows preservation of the native femoral head
- Internal fixation reduces hospitalisation length and improves rehabilitation
Displaced Intracapsular Fractures (Garden III/IV)
-
Elderly patients / low functional demand:
- Hemiarthroplasty (Austin Moore, Thompson, bipolar) - femoral head replaced, acetabulum left native. Allows immediate weight-bearing.
- Recent evidence (2025 meta-analysis, PMID 40270012) suggests dual mobility cups may reduce dislocation risk vs conventional hemiarthroplasty
-
Younger, independently mobile patients:
- Total hip arthroplasty (THA) - better functional outcomes, more appropriate when acetabular cartilage may be worn
- A 2024 systematic review (PMID 39436746) compared supercapsular percutaneous approaches vs standard posterior approach for THA in this setting
-
Young patients (<60 years) with undisplaced intracapsular fractures:
- ORIF with dynamic hip screw (DHS) or multiple cannulated screws, aiming to preserve the native head
Extracapsular Fractures (Intertrochanteric / Subtrochanteric)
- Stable extracapsular fractures:
- Dynamic hip screw (DHS) - a sliding screw in a barrel that allows controlled compression at the fracture site on weight-bearing, protecting the femoral head from screw penetration in osteoporotic bone

- Unstable extracapsular fractures (reverse oblique pattern, comminuted medial calcar/lesser trochanter):
- Intramedullary device (cephalomedullary nail) preferred due to unfavourable mechanics with DHS
Paediatric Fractures (Delbet Types I-III)
- Surgical emergencies - ORIF urgently
- Smooth pins in younger children; threaded pins in adolescents
- Post-op spica casting may be required in younger/more severe injuries
Complications
| Complication | Details |
|---|---|
| Avascular necrosis (AVN) | Most common. 15-35% of displaced intracapsular fractures. Due to disruption of retinacular vessels. |
| Nonunion | Second major complication. Due to poor blood supply and shear forces at the fracture site. |
| Pulmonary embolism | Leading cause of death 7 days post-fracture. DVT prophylaxis is mandatory. |
| Deep infection | Osteomyelitis or septic arthritis (fracture line extends into the joint). Perioperative antibiotics reduce risk. |
| Coxa vara | Especially in paediatric cases. |
| Physeal arrest | In children with transphyseal fractures. |
Recent Evidence Note: A 2025 meta-analysis (PMID 41303766) found that thromboembolic risk after THA vs hemiarthroplasty may differ - review VTE prophylaxis protocols accordingly.
Key Teaching Points
- Femoral neck fractures are mostly intracapsular - subcapital, transcervical, basicervical
- Blood supply is tenuous at baseline in the elderly (attenuated medullary and ligamentum teres vessels); a displaced fracture tears the retinacular vessels, making AVN nearly inevitable
- Extracapsular fractures (intertrochanteric) do not disrupt femoral head blood supply - DHS is the treatment of choice
- The classification that matters most clinically: displaced vs undisplaced (not Garden I/II/III/IV in isolation)
- MRI is the gold standard for occult fractures when plain films are negative
- Skeletal traction is contraindicated - it stretches and may occlude the retinacular vessels
Sources: Gray's Anatomy for Students, p.784 | Bailey and Love's Short Practice of Surgery 28th Ed, p.458 | Rosen's Emergency Medicine | Tintinalli's Emergency Medicine | Pfenninger and Fowler's Procedures for Primary Care, p.1312 | Grainger & Allison's Diagnostic Radiology | Campbell's Operative Orthopaedics 15th Ed 2026 | Miller's Review of Orthopaedics 9th Ed
This is a shared conversation. Sign in to Orris to start your own chat.